Potters syndrome
Reading File
Finding Sources
Finding Sources
Searching PubMed
Potter sequence oligohydramnios renal agenesis
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
I now have all the information needed for a comprehensive answer.
Potter Syndrome (Potter Sequence / Oligohydramnios Sequence)
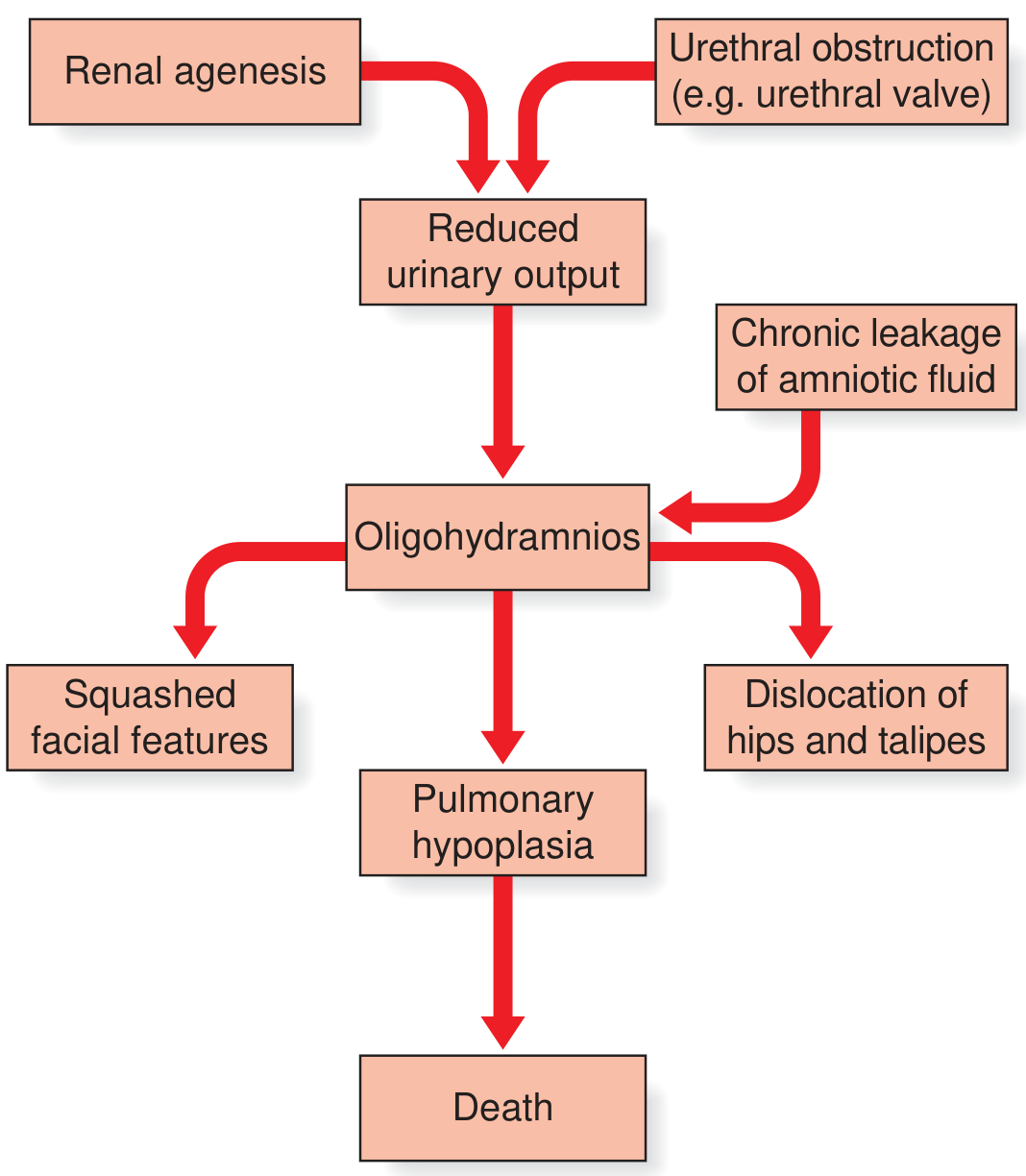
Potter syndrome is better termed the Potter sequence - it is not a primary syndrome but a cascade of secondary deformations triggered by a single upstream cause: oligohydramnios (severely reduced amniotic fluid volume).
Pathophysiology - The Sequence
The underlying logic is that fetal urine is the primary contributor to amniotic fluid after the first trimester. Anything that reduces fetal urine output (or causes fluid to leak out) leads to oligohydramnios, which then drives a cascade of downstream complications.
Causes of Oligohydramnios in Potter Sequence
| Category | Examples |
|---|---|
| Reduced fetal urine output | Bilateral renal agenesis, bilateral multicystic dysplastic kidney, severe bilateral renal hypoplasia/dysplasia |
| Urinary tract obstruction | Posterior urethral valves, urethral atresia (associated with Prune Belly syndrome category I) |
| Chronic amniotic fluid leakage | Prolonged rupture of membranes |
Bilateral renal agenesis is the classic cause - incidence approximately 1 in 4000 births, associated with the full Potter sequence. - Goldman-Cecil Medicine, p. 1258
Clinical Features
The oligohydramnios causes fetal compression, which produces the characteristic physical features:
Potter Facies (compression-related):
- Flattened/squashed nose
- Retrognathia (recessed jaw)
- Low-set ears
- Wide epicanthal folds
- Flattened facial features from in utero compression
Limb and musculoskeletal deformities:
- Dislocation of the hips
- Talipes (club foot)
- Arthrogryposis/limb positional deformities
Pulmonary hypoplasia - the lethal lesion:
- Severe oligohydramnios during the canalicular phase of fetal lung development (16-24 weeks) is particularly damaging
- Results in small, underdeveloped lungs with a bell-shaped chest on imaging
- Leads to neonatal death from respiratory failure in bilateral cases
Associations and Causes - Broader Context
- VACTERL association - vertebral, anal, cardiac, tracheoesophageal, renal, limb defects (30% of VACTERL patients have unilateral renal agenesis)
- Prune Belly syndrome Category I - includes oligohydramnios, pulmonary hypoplasia, Potter features, and urethral atresia
- Bilateral renal agenesis is associated with genital anomalies (absent vas deferens/seminal vesicles in males; mullerian duct anomalies in females), cardiovascular anomalies (30%), and musculoskeletal anomalies (14%)
- Familial/hereditary renal dysplasia syndrome (OMIM 191830) - autosomal dominant with variable penetrance; features unilateral/bilateral agenesis, dysplasia, and hydronephrosis - Creasy & Resnik's Maternal-Fetal Medicine
Diagnosis
Prenatal (Ultrasound):
- Oligohydramnios or anhydramnios
- Non-visualisation of kidneys and/or bladder
- Small, echogenic kidneys (renal dysplasia)
- Absent renal arteries on color Doppler
- Bell-shaped small chest (pulmonary hypoplasia)
- Fetal MRI can be used to confirm bilateral renal agenesis when ultrasound is equivocal
Postnatal:
- Characteristic Potter facies
- Respiratory failure at birth
- Absent urinary output
Prognosis
| Scenario | Mortality |
|---|---|
| Bilateral renal agenesis (classic Potter) | ~100% - critical pulmonary hypoplasia incompatible with survival |
| Severe oligohydramnios/anhydramnios | 95% mortality |
| Abnormal kidneys or fetal urine parameters | 70% mortality |
| Nondysplastic kidneys with normal fetal urine | ~10% mortality |
| Perinatal mortality overall (with obstruction etiology) | ~50% even with fetal intervention |
In survivors (obstructive cases): up to 50% develop chronic renal insufficiency requiring dialysis and/or transplantation; recurrent UTI and vesicoureteral reflux are common. - Creasy & Resnik's, p. 5153
Antenatal Management
- Bilateral renal agenesis with severe oligo/anhydramnios: the condition is lethal; termination of pregnancy is an option to discuss. Unmonitored labor is appropriate; cesarean only for obstetric indications
- Serial amnioinfusion: proposed to prevent pulmonary hypoplasia during canalicular phase (16-24 weeks) but has only rarely achieved long-term survival; should only be undertaken within approved experimental protocols
- One exceptional case of survival with serial amnioinfusions from 23 weeks, followed by postnatal peritoneal dialysis bridging to renal transplant at 1 year, has been published
- Unilateral renal agenesis: serial ultrasound to monitor growth, contralateral kidney, and fluid; weekly AFI assessment after 32-34 weeks; assess maternal kidneys (15% risk of congenital renal abnormalities in first-degree relatives)
Key Distinction
"Potter syndrome" is technically a sequence (one initiating event - oligohydramnios - cascading into multiple structural deformations), not a syndrome in the strict genetic sense. The term is now often replaced by "oligohydramnios sequence" in modern literature to reflect this pathophysiological understanding. - Emery's Elements of Medical Genetics and Genomics, p. 241
This is a shared conversation. Sign in to Orris to start your own chat.