Rheumatoid arthritis management in adults
Reading File
Finding Sources
Searching PubMed
"rheumatoid arthritis"[MeSH Terms] AND "disease management"[MeSH Terms]
Searching the Web
rheumatoid arthritis management guidelines 2025 ACR EULAR
Finding Sources
Searching PubMed
"rheumatoid arthritis"[MeSH Terms] AND treatment
Reading Web Page
https://ard.eular.org/article/S0003-4967(26)00075-0/fulltext
Finding Sources
Searching PubMed
"rheumatoid arthritis"[MeSH Terms] AND "antirheumatic agents"[MeSH Terms]
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading Web Page
https://rheumnow.com/news/2025-update-eular-recommendations-…
I now have excellent, comprehensive content from multiple textbooks plus the 2025 EULAR update. Let me compile the full answer.
Rheumatoid Arthritis: Management in Adults
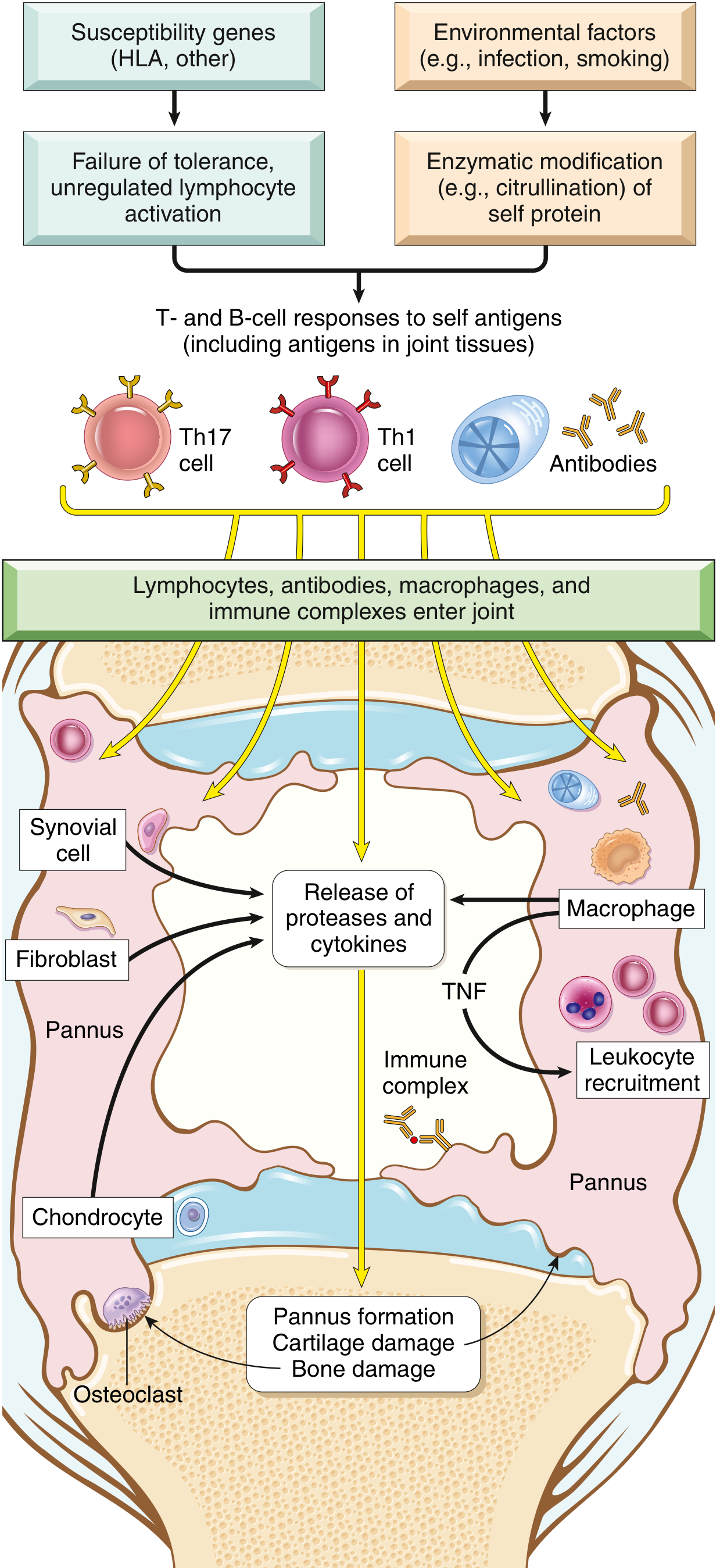
Pathogenesis (Why This Guides Treatment)
RA is driven by a CD4+ T-cell-mediated autoimmune response against joint antigens. Key mediators include:
- TNF, IL-1, IL-6 (from macrophages) - recruit leukocytes, activate proteases destroying cartilage
- IL-17 (from Th17 cells) - recruits neutrophils and monocytes
- RANKL (from activated T cells) - stimulates osteoclasts causing bone resorption
- Anti-citrullinated peptide antibodies (ACPA) - present in ~70% of patients; associated with disease severity
- Rheumatoid factor (RF) - IgM/IgA autoantibodies binding IgG Fc; present in ~80%
Diagnosis and Classification
The 2010 ACR/EULAR criteria (replacing the 1987 criteria) score patients on:
- Joint involvement (large vs. small, number)
- Serology (RF, ACPA - negative, low positive, high positive)
- Acute phase reactants (CRP, ESR)
- Duration (≥6 weeks)
A score ≥6/10 classifies definite RA.
Key clinical features:
- Symmetric synovitis with morning stiffness >1 hour (hallmark)
- Predilection for MCPs, PIPs, wrists, MTPs
- Extraarticular: rheumatoid nodules, pulmonary fibrosis, vasculitis, sicca, pericarditis
- Poor prognostic factors: functional limitation, extraarticular disease, RF/ACPA positivity, bony erosions on imaging
Treatment Philosophy: Treat-to-Target (T2T)
The foundational principle of modern RA management, endorsed by both EULAR (2025 update) and ACR:
Target = sustained clinical remission (or low disease activity in long-standing/refractory disease). Any disease activity above low disease activity is unacceptable.
- Monitor disease activity every 1-3 months when active
- If no improvement at 3 months after starting treatment, or target not reached at 6 months - adjust therapy
- Once target is sustained, monitoring frequency can decrease
Disease activity is measured using composite scores: DAS28, SDAI, CDAI, or ACR/EULAR Boolean remission criteria.
Pharmacological Management
Step 1: Start DMARDs at Diagnosis
NSAIDs provide only symptomatic relief without altering prognosis. DMARDs must be started as soon as RA is diagnosed - before radiographic erosions appear (which can occur within months to 2 years).
Conventional Synthetic DMARDs (csDMARDs)
| Drug | Dose | Key Points | Monitoring |
|---|---|---|---|
| Methotrexate (first-line) | 7.5-25 mg/week (oral or SC) | Anchor drug; combine with folic acid 1 mg/day to reduce toxicity | CBC, LFTs, creatinine monthly x3 months, then every 3-4 months |
| Hydroxychloroquine | 200-400 mg/day | Least toxic csDMARD; mild RA only | Ophthalmology exam at 6 months, then annually |
| Sulfasalazine | 2-3 g/day in divided doses | Check for sulfa allergy first | CBC, LFTs weekly x1 month, then every 4-6 weeks |
| Leflunomide | 20 mg/day (loading 100 mg/day x3) | Alternative if MTX contraindicated; teratogenic | CBC, LFTs monthly x6 months |
MTX is the anchor csDMARD - it is recommended as part of the first treatment strategy in all patients (EULAR 2025). If MTX is contraindicated or not tolerated, use leflunomide or sulfasalazine.
Triple therapy (MTX + hydroxychloroquine + sulfasalazine) has evidence comparable to biologic combinations in some early RA populations.
MTX mechanism: Inhibits dihydrofolate reductase → reduces purine/pyrimidine synthesis; also elevates adenosine (anti-inflammatory). Dose is ramped up while monitoring for toxicity. Subcutaneous dosing improves bioavailability and reduces GI side effects. Dose reduction needed in renal insufficiency. Avoid alcohol; contraindicated in liver disease. - Goldman-Cecil Medicine, p. 2811
Glucocorticoids
- Short-term use at the start of therapy (alongside MTX) is recommended by EULAR 2025 to bridge until DMARDs take effect
- Low-dose prednisone ≤10 mg/day or intraarticular injections for flares
- Not for long-term monotherapy; taper and discontinue once DMARD is effective
- Risks: osteoporosis, hyperglycemia, infection - co-prescribe calcium/vitamin D and consider bisphosphonate
Step 2: Insufficient Response to csDMARDs (3-6 Months)
If target not reached after adequate trial of csDMARDs, add a biologic DMARD (bDMARD) or targeted synthetic DMARD (tsDMARD) in combination with MTX.
Biological DMARDs (bDMARDs)
TNF Inhibitors (first-line biologics):
| Agent | Mechanism | Route |
|---|---|---|
| Etanercept | Soluble TNF receptor fusion protein | SC weekly |
| Adalimumab | Anti-TNF monoclonal antibody | SC every 2 weeks |
| Infliximab | Anti-TNF monoclonal antibody | IV infusion |
| Certolizumab pegol | PEGylated anti-TNF Fab fragment | SC |
| Golimumab | Anti-TNF monoclonal antibody | SC monthly or IV |
Other bDMARDs (after TNF failure or as alternatives):
| Drug | Target | Notes |
|---|---|---|
| Abatacept | CTLA4-Ig (T-cell costimulation) | SC or IV |
| Rituximab | Anti-CD20 (B-cell depletion) | IV infusion; preferred in RF/ACPA+ disease |
| Tocilizumab | Anti-IL-6 receptor | IV or SC; can be used as monotherapy |
| Sarilumab | Anti-IL-6 receptor | SC |
| Anakinra | IL-1 receptor antagonist | SC daily; less used |
Key principle: If one TNF inhibitor or IL-6R inhibitor fails, can switch to a different mechanism OR try a second TNF/IL-6R inhibitor. - EULAR 2025
Targeted Synthetic DMARDs (tsDMARDs) - JAK Inhibitors
| Drug | Selectivity | Dose |
|---|---|---|
| Tofacitinib | JAK1/3 inhibitor | 5 mg BID or 11 mg XR once daily |
| Baricitinib | JAK1/2 inhibitor | 2 mg or 4 mg once daily |
| Upadacitinib | Selective JAK1 | 15 mg or 30 mg once daily |
Important safety signals (FDA black box warning):
JAK inhibitors carry class-wide warnings for:
- Increased risk of major adverse cardiovascular events (MACE) (HR ~1.33 vs. TNFi)
- Increased malignancy risk (HR ~1.48 vs. TNFi, from ORAL Surveillance trial)
- Increased risk of thromboembolism
- Increased all-cause mortality
The ORAL Surveillance trial compared tofacitinib vs. TNF inhibitors in RA patients over age 50 with ≥1 cardiovascular risk factor; tofacitinib did not meet noninferiority. - Firestein & Kelley's Textbook of Rheumatology, 2-Volume Set
EULAR 2025 guidance: JAK inhibitors can be used after careful consideration of risks, particularly in patients without high CV risk, malignancy history, or thromboembolic risk.
EULAR 2025 Updated Recommendations (Published March 2026)
The 2025 update streamlined from 11 to 9 recommendations:
- Start DMARDs as soon as RA is diagnosed
- Treat-to-target: aim for sustained remission (or low disease activity in refractory/long-standing disease)
- Monitor every 1-3 months; adjust at 3 months if no improvement, or at 6 months if target not reached
- MTX (+ short-term glucocorticoids) as first-line; if contraindicated, use leflunomide or sulfasalazine
- In patients with poor prognostic factors (high disease activity, early erosions, high RF/ACPA), combination csDMARDs or early bDMARD addition is considered
- If csDMARDs insufficient, add bDMARD or tsDMARD (JAKi with risk consideration)
- Biosimilars should be used where appropriate (same efficacy as originators)
- If first bDMARD/JAKi fails, try another (same or different class)
- In sustained remission: continue DMARDs but dose tapering may be considered; stopping often leads to flares
The 2025 EULAR recommendations (Smolen et al., Ann Rheum Dis, 2026) provide the current global standard.
Non-Pharmacological Management
| Modality | Role |
|---|---|
| Physiotherapy | Range-of-motion exercises, joint protection, strengthening |
| Occupational therapy | Splints, adaptive devices, activity modification |
| Patient education | DMARD compliance, disease monitoring, self-management |
| Smoking cessation | Smoking is an established environmental trigger and worsens prognosis |
| Cardiovascular risk management | RA is an independent CVD risk factor; manage lipids, BP, diabetes |
| Bone protection | Calcium, vitamin D; bisphosphonates if on prolonged steroids |
| Surgery | Synovectomy, joint replacement for end-stage disease |
Monitoring Schedule Summary
| Drug | Blood Tests | Frequency |
|---|---|---|
| Methotrexate | CBC, LFTs, creatinine | Monthly x3, then every 3-4 months |
| Sulfasalazine | CBC, LFTs | Weekly x1 month, then every 4-6 weeks |
| Hydroxychloroquine | Eye exam (visual fields) | Baseline, then annually |
| Leflunomide | CBC, LFTs | Monthly x6 months |
| All biologics/JAKi | CBC, infection screen, TB screening before starting | Per product labeling |
Special Populations
- Pregnancy: Stop MTX (teratogenic - category X) and leflunomide (teratogenic) before conception. Hydroxychloroquine and sulfasalazine (+ folic acid) are relatively safer. TNF inhibitors generally compatible in first/second trimester; certolizumab has least placental transfer. JAK inhibitors - avoid.
- Elderly/Renal impairment: Reduce MTX dose; JAK inhibitors also need dose adjustment for renal function.
- Infections/TB: Screen for latent TB (TST or IGRA) before all biologics and JAK inhibitors. Hold immunosuppressives during serious infections.
- Pre-surgery: Decision on holding biologics peri-operatively depends on drug half-life and surgical risk.
Sources:
- Textbook of Family Medicine, 9th edition (Swanson), p. 879-887
- Goldman-Cecil Medicine International Edition, p. 2811
- Robbins & Kumar Basic Pathology, p. 792
- Firestein & Kelley's Textbook of Rheumatology, 2-Volume Set
- EULAR 2025 RA Recommendations (Smolen JS et al., Ann Rheum Dis, 2026) - most current global guideline
This is a shared conversation. Sign in to Orris to start your own chat.