Fate of primary complex in tb Full details for md exams 15marks answer
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Finding Sources
I now have comprehensive material from Robbins & Kumar Pathologic Basis of Disease, Robbins Basic Pathology, and the landmark natural history diagram. Let me compile the complete MD exam answer.
Fate of Primary Complex in Tuberculosis
Introduction
The primary complex (Ghon complex) is the combined lesion of primary tuberculosis — formed when Mycobacterium tuberculosis first infects a previously unsensitized host. It consists of two components:
- Ghon focus — the parenchymal lung lesion (1–1.5 cm, gray-white, caseous centre, subpleural, lower part of upper lobe or upper part of lower lobe)
- Lymph node component — regional hilar/tracheobronchial lymph nodes that undergo caseation
Together, the parenchymal focus + lymphatic vessels + draining nodes = Ghon (primary) complex.
The Primary Complex: Formation
- Inhaled bacilli implant in distal airspaces, subpleurally
- Initially an exudative reaction (neutrophils, then macrophages)
- As cell-mediated immunity (Th1/CD4⁺) develops over 3–6 weeks, the lesion becomes granulomatous
- A 1–1.5 cm gray-white consolidation — the Ghon focus — forms with central caseous necrosis
- Bacilli drain via lymphatics → regional nodes → caseating lymphadenitis
- Early hematogenous dissemination occurs in the first few weeks (seeding liver, spleen, kidneys, meninges, bone) — usually contained
Fate of the Primary Complex — Overview
In ~95% of immunocompetent individuals, cell-mediated immunity successfully controls the infection. The Ghon complex then undergoes one of the following fates:
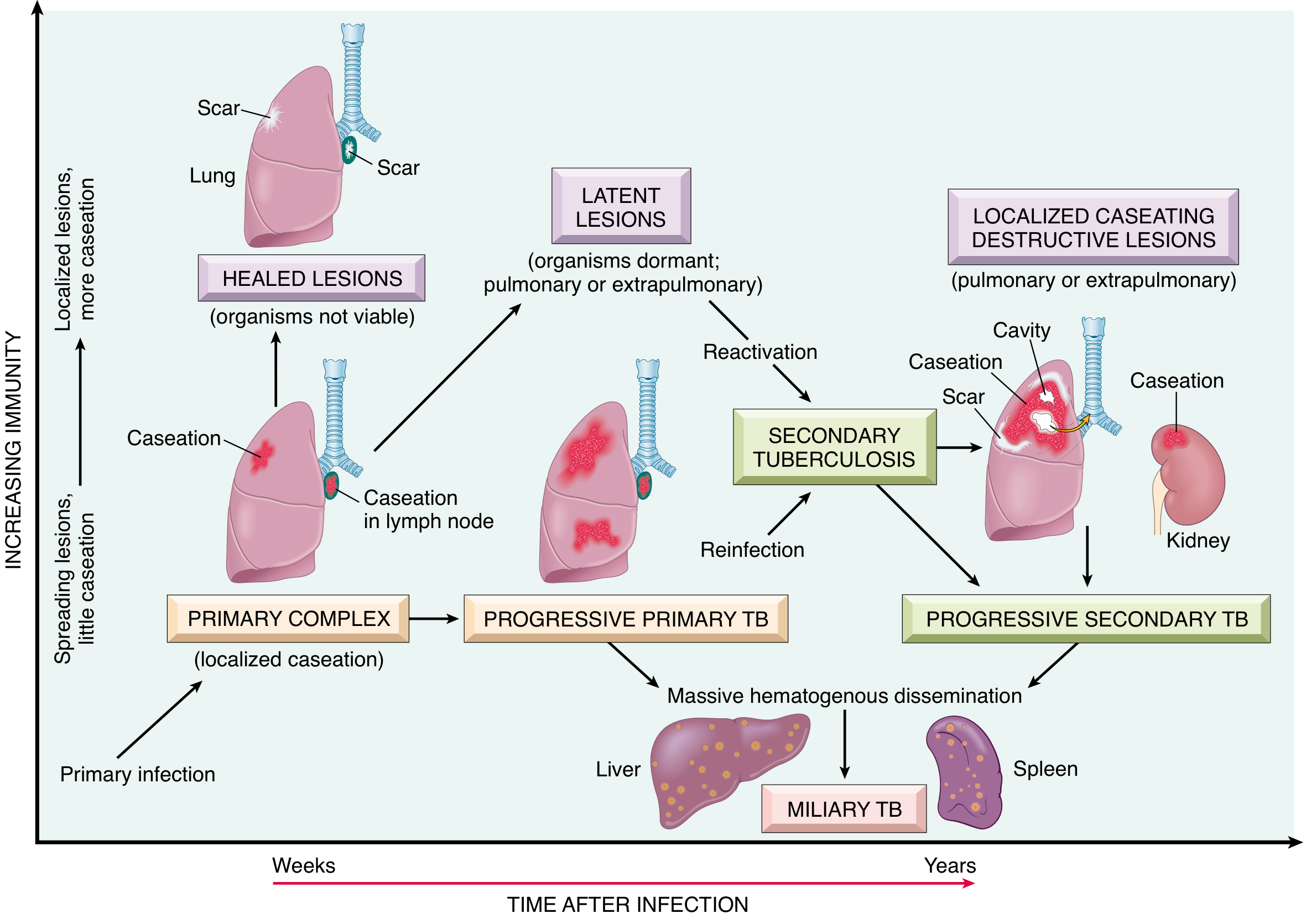
Fate 1: Resolution and Healing (Most Common — ~95%)
The usual fate in immunocompetent hosts.
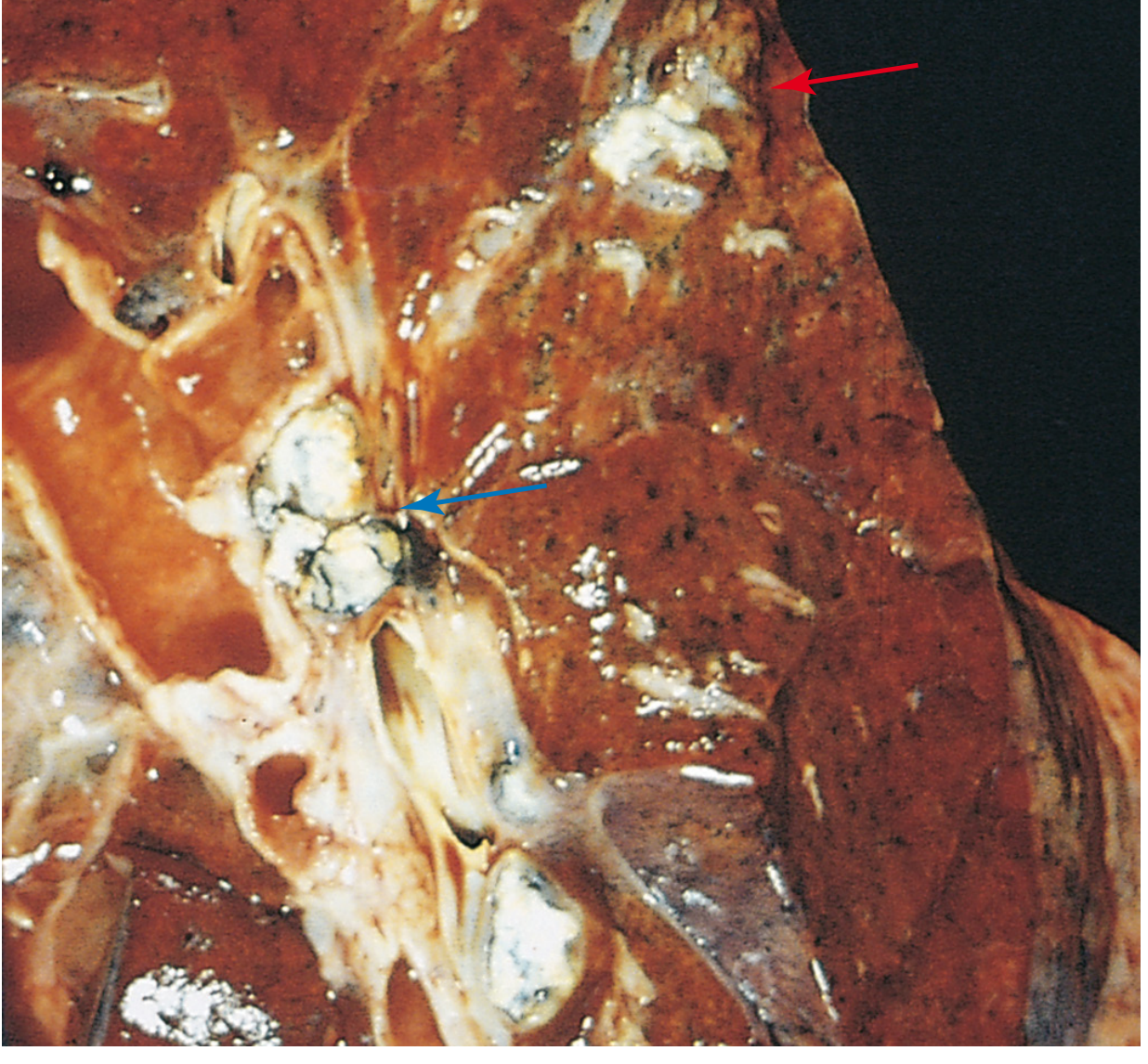
- The Ghon complex undergoes progressive fibrosis → fibrocalcific scar
- The caseated centre gets dystrophic calcification (visible on X-ray as a calcified nodule)
- The hilar lymph nodes also calcify
- Ranke complex = calcified Ghon focus + calcified hilar lymph nodes (radiological term for healed primary complex)
- Organisms are killed or rendered non-viable — latency or complete clearance
- No clinical disease; tuberculin test becomes positive (indicating sensitization)
- Histologically: late fibrocalcific stages show no demonstrable bacilli on acid-fast stain
Key point: The healing is progressive encapsulation by fibroblasts → hyalinization → calcification. Despite early hematogenous seeding of other organs, no lesions develop if immunity is adequate.
Fate 2: Latent Tuberculosis (Dormancy)
- Organisms survive in a dormant state within macrophages/granulomas, particularly at the apices (where pO₂ is highest)
- The individual is tuberculin-positive but has no active disease
- This is latent TB infection (LTBI)
- Years to decades later, if host defenses weaken (HIV, immunosuppressants, malnutrition, diabetes, aging, steroids, anti-TNF therapy, renal failure), reactivation can occur → secondary (postprimary) TB
Fate 3: Progressive Primary Tuberculosis (Uncommon — ~5%)
Occurs in immunocompromised individuals: HIV-positive (CD4⁺ <200 cells/µL), severely malnourished, young infants, or those with inherited Th1 pathway defects (Mendelian susceptibility to mycobacterial disease — e.g., IL-12Rβ1 mutations).
Mechanisms of Progression:
a) Local pulmonary progression:
- The Ghon focus enlarges → consolidates a lobe
- Clinical picture resembles acute bacterial pneumonia (lower/middle lobe consolidation + hilar lymphadenopathy + pleural effusion)
- Cavitation is less common than in secondary TB
b) Lymph node enlargement and complications:
- Massive hilar/mediastinal lymphadenopathy
- Compression/erosion of bronchi → collapse, obstructive pneumonitis
- Lymph node ruptures into bronchus → endobronchial spread of infection (bronchopneumonia)
c) Pleural involvement:
- Extension of infection to the pleural surface → serous pleural effusion, empyema, or obliterative fibrous pleuritis
d) Hematogenous dissemination (Miliary TB):
- Bacilli enter the venous blood via eroded lymphatics → circulate back to lungs and systemic organs
- Miliary tuberculosis: numerous 1–2 mm yellow-white foci in liver, spleen, bone marrow, adrenals, meninges, kidneys, fallopian tubes, epididymis (name "miliary" from resemblance to millet seeds)
- Can involve any organ
e) Tuberculous meningitis:
- Via hematogenous seeding of the brain parenchyma → millet-sized tubercles in parenchyma → rupture into subarachnoid space
- One of the most serious complications of progressive primary TB
Fate 4: Reactivation (Secondary/Postprimary TB) — After Years
- In previously sensitized individuals, the latent Ghon complex reactivates, typically at the apex of the upper lobe (high pO₂ favors bacillary growth)
- Alternatively, may arise from exogenous reinfection with new bacilli
- Because hypersensitivity is pre-established, the immune response is prompt and intense → rapid walling off → but also rapid tissue necrosis
- Regional lymph nodes are less prominently involved than in primary TB (pre-existing immunity)
- Cavitation is characteristic of secondary TB (unlike primary)
- Organisms drain through lymphatics → secondary spread, miliary seeding, or endobronchial spread
Summary Table: Fates of Primary Complex
| Fate | Frequency | Mechanism | Outcome |
|---|---|---|---|
| Resolution/Healing | ~95% | Fibrosis → calcification | Ranke complex, no disease; LTBI |
| Latent TB | Common | Dormant organisms in granuloma | Risk of reactivation later |
| Progressive primary TB | ~5% (immunocompromised) | Failure of cell-mediated immunity | Lobar pneumonia, miliary TB, meningitis |
| Secondary (reactivation) TB | Years later | Waning immunity / reinfection | Apical cavitary disease |
| Miliary TB | Rare but serious | Massive hematogenous spread | Multiorgan seeding |
| Pleural/lymph node complications | Variable | Local extension | Effusion, empyema, scrofula |
Extrapulmonary Seeding — Organs Commonly Involved
From early hematogenous dissemination during primary complex, the following organs may be seeded and develop isolated tuberculosis:
| Organ | Disease |
|---|---|
| Meninges | Tuberculous meningitis |
| Kidneys | Renal tuberculosis |
| Adrenal glands | Addison disease (historically important) |
| Vertebrae | Pott disease (spinal TB) — with potential "cold abscess" tracking along tissue planes |
| Fallopian tubes | Salpingitis, infertility |
| Epididymis | Epididymal tuberculosis |
| Cervical lymph nodes | Scrofula (most common extrapulmonary presentation) |
| Liver, spleen, bone marrow | Miliary deposits |
Key Histological Features
- Active granuloma: Epithelioid histiocytes + Langhans-type multinucleated giant cells + central caseous necrosis + peripheral lymphocytes + fibroblastic rim
- Caseation: Amorphous, eosinophilic, "cheese-like" necrosis (hallmark of TB)
- Healing stages: Progressive fibrosis → hyalinization → calcification → acid-fast bacilli no longer demonstrable
- Immunocompromised: Poorly formed or absent granulomas; macrophages laden with bacilli (no effective containment)
Important Exam Points
- Ghon focus = parenchymal lesion only; Ghon/primary complex = parenchymal + lymph node + lymphatics
- Ranke complex = fully calcified Ghon complex (both Ghon focus + hilar nodes calcified) — indicates healed primary TB
- In 95% of cases, immunity resolves the primary complex → fibrocalcific scar
- In ~5%, progressive primary TB occurs — predominantly in immunocompromised patients
- Tuberculin positivity (Mantoux/IGRA) indicates sensitization — does NOT differentiate active vs. latent disease
- Loss of tuberculin reactivity in a previously positive patient = ominous sign of waning immunity
- Pott disease (vertebral TB) + "cold abscess" tracking along tissue planes is a classic exam scenario
- Miliary TB = hematogenous dissemination → millet-seed (2 mm) foci in multiple organs; most prominent in liver, bone marrow, spleen, adrenals, meninges, kidneys
Sources: Robbins & Cotran Pathologic Basis of Disease, 10th Ed.; Robbins Basic Pathology (Robbins Pathology); Harrison's Principles of Internal Medicine 22E
This is a shared conversation. Sign in to Orris to start your own chat.