Bullous lung diseases full details for md exam answer 15 marks from fishman crofton Murray combined points
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Finding Sources
I now have comprehensive material. Let me compile the full 15-mark MD exam answer integrating all sources.
Bullous Lung Disease — MD Examination Answer (15 Marks)
Sources: Fishman's Pulmonary Diseases and Disorders (Chapter 50), Murray & Nadel's Textbook of Respiratory Medicine
1. DEFINITIONS AND TERMINOLOGY
Bulla (pl. bullae): An air-containing space within the lung parenchyma that arises from destruction, dilation, and confluence of airspaces distal to terminal bronchioles, >1 cm in diameter. Its walls are composed of attenuated and compressed parenchyma. — Fishman's, Ch. 50
Distinction from related entities:
| Entity | Definition | Key Distinction |
|---|---|---|
| Bulla | Air space >1 cm, within parenchyma, deep to internal elastic layer of visceral pleura | Confined by connective tissue septa |
| Bleb | Air accumulation between the two layers of visceral pleura (sub-pleural), not confined by septa | Superficial; leads to primary spontaneous pneumothorax |
| Cyst | Epithelial-lined cavity; may be developmental (bronchogenic cyst, CPAM) | Has true epithelial lining |
Bullous disease: Multiple bullae in lungs that are otherwise normal — a distinct entity from bullae occurring with COPD/emphysema.
Giant bullous emphysema (Vanishing Lung Syndrome): Bullae occupying ≥1/3 of a hemithorax, rapidly replacing parenchyma.
2. CLASSIFICATION OF BULLAE
Bullae occur in four distinct clinical contexts (Fishman's):
- With emphysema — "bullous emphysema" (most common)
- With pulmonary fibrosis — late-stage sarcoidosis, complicated pneumoconiosis, post-COVID-19
- Vanishing lung — parenchyma rapidly replaced by multiple bullae
- Otherwise normal lungs — "bullous lung disease" proper; different etiology and natural history
3. ETIOLOGY AND PATHOGENESIS
Risk factors:
- Cigarette smoking (most important)
- α₁-antitrypsin deficiency — measure α₁-AT level in all patients
- Marijuana smoking
- Intravenous drug abuse
- Marfan syndrome / connective tissue disorders (defect in elastin/fibrillin)
- Ehlers-Danlos syndrome (cutis laxa variant with elastase gene defect)
Pathogenetic mechanisms by which bullae form:
- Emphysema of distal acini — destruction of alveolar walls → airspace coalescence
- Scar tissue formation — traps areas of normal lung, enlarges airspaces by traction on surrounding intact alveoli
- Chronic inflammation — neutrophil-mediated protease/antiprotease imbalance
- Check-valve mechanism — partial bronchiolar obstruction → progressive air trapping
- Intravenous drug abuse — talc granulomatosis, septic emboli
The protease-antiprotease imbalance is central: excess elastase activity (from neutrophils, macrophages) degrades the elastin scaffold, leading to confluent airspace enlargement. In α₁-AT deficiency, this is amplified by absence of the primary anti-elastase defense.
4. DISTRIBUTION OF BULLAE
Bullae preferentially involve the upper lobes — attributed to greater mechanical stress:
- Intrapleural pressure at apices is more negative than at bases
- Apical alveoli are subjected to greater expanding (distending) stresses
- Radioactive gas studies confirm apical alveoli are considerably larger than basal alveoli at normal lung volumes
- By contrast, panacinar emphysema of α₁-AT deficiency affects lower lobes — a key distinguishing point (Fishman's)
- Paraseptal emphysema (subpleural, upper lobe) → bleb formation → primary spontaneous pneumothorax in young men
5. CLINICAL FEATURES
Symptoms:
- Asymptomatic — bullae found incidentally on CXR/CT (small bullae rarely symptomatic)
- Progressive dyspnea — the most common presenting symptom in symptomatic patients; due to compression of adjacent normal lung and wasted ventilation
- Pleuritic chest pain
- Sudden severe breathlessness — secondary spontaneous pneumothorax (rupture) or sudden increase in bulla size
- Fever, cough, purulent sputum — infected bulla
Physical examination:
- Usually reflects the overall state of the lungs
- Giant bullae → localized absent breath sounds + increased percussion resonance over the affected area
- In otherwise-normal lungs with small bullae: examination may be normal
- Hyperinflation signs if associated COPD: barrel chest, reduced diaphragmatic excursion
6. INVESTIGATIONS
A. Laboratory
- Hemoglobin/hematocrit — detect anemia (contributing to dyspnea) or secondary polycythemia (chronic hypoxemia)
- α₁-antitrypsin level — mandatory in all patients to detect deficiency
- Arterial blood gases — essential in severe respiratory insufficiency and pre-operative bullectomy assessment; PaCO₂ >45 mmHg = relative contraindication to bullectomy
B. Pulmonary Function Tests (PFTs)
| Test | Bullous Disease (isolated) | Bullae + Obstructive Disease |
|---|---|---|
| TLC | Normal | Normal to ↑ |
| RV | Normal | ↑ |
| FRC (plethysmography) | ↑ | ↑ |
| RV/TLC% | Normal | ↑ |
| FEV₁/FVC | Normal | ↓ |
| DLCO/VA | Normal | ↓ |
| Raw | Normal to ↑ | ↑ |
| Static compliance | Normal to ↑ | ↑ |
Key point: DLCO is the best discriminator between isolated bullae and widespread emphysema — DLCO correlates better with morphologic emphysema than most other tests. If DLCO is normal or near-normal with large bullae → underlying lung may be well-preserved → better surgical candidate.
C. Exercise Testing
- Isolated bullous disease (normal lungs): A-a gradient, dead space/tidal volume ratio, and arterial oxygenation remain normal or near-normal with exercise
- Bullae with panacinar emphysema: A-aDO₂ widened at rest and worsens with exercise
D. Imaging
Chest Radiograph:
- Hyperlucent area with visible wall (thin hairline shadow)
- Compresses adjacent lung
- May show air-fluid level with infected bulla
- Giant bulla: may mimic pneumothorax — differentiation critical (CXR alone may be unreliable)
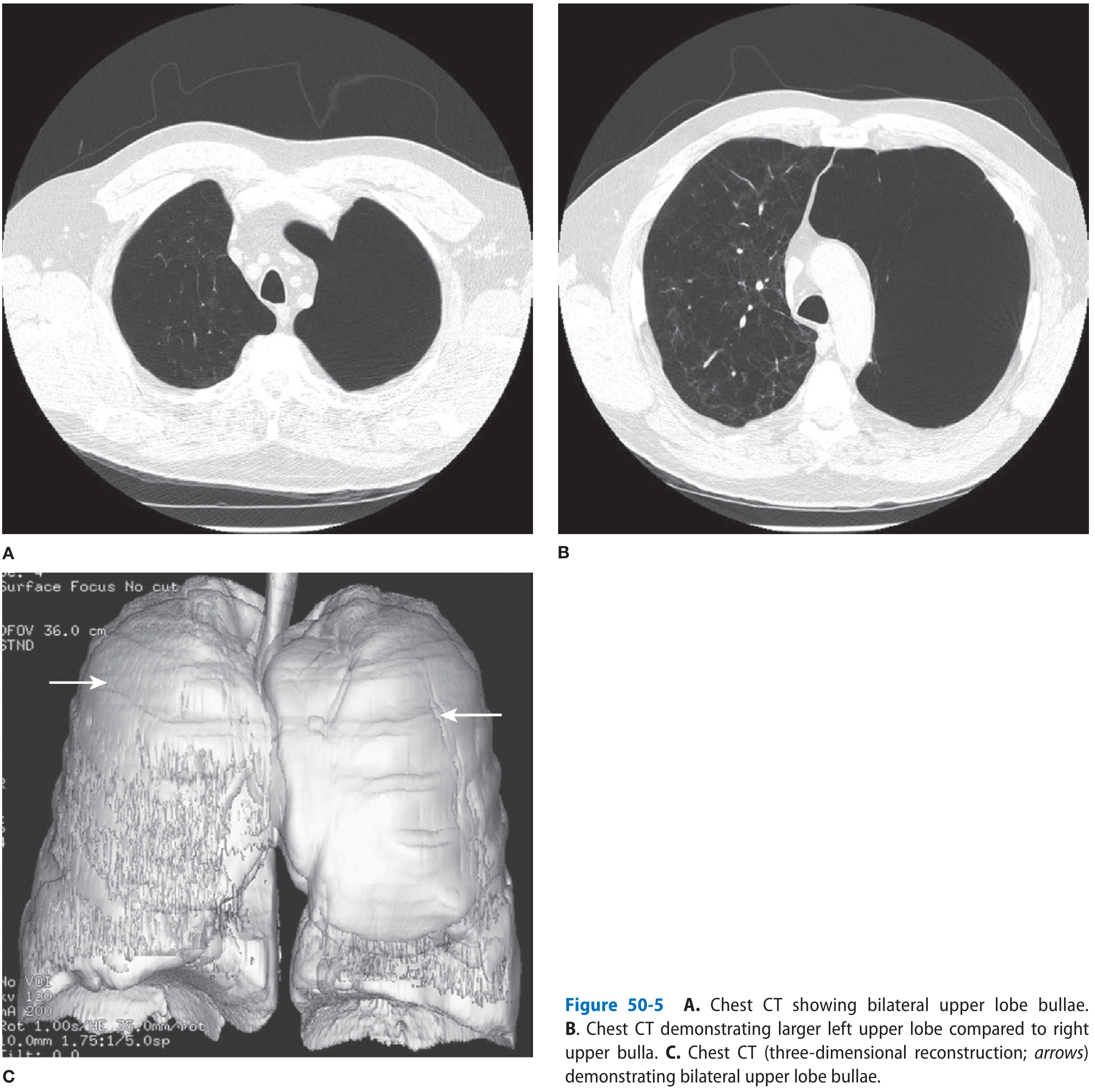
HRCT Chest (investigation of choice):
- Demonstrates extent, size, number, and distribution of bullae
- Detects underlying emphysema type (centrilobular, panacinar, paraseptal)
- Identifies compressed adjacent parenchyma and its quality (key surgical planning tool)
- Assesses presence of air-fluid levels (infected bulla)
- Detects nodules/mural thickening suggesting malignancy
- 3D reconstruction possible for surgical planning
Nuclear Medicine:
- Ventilation-perfusion scintigraphy: bullae show absent ventilation AND absent perfusion
- Helps assess functional contribution of compressed adjacent lung
7. COMPLICATIONS
A. Spontaneous Pneumothorax
- Most important acute complication
- Paraseptal emphysema → bleb rupture → primary spontaneous pneumothorax (typically young, tall men)
- Secondary spontaneous pneumothorax with diffuse bullous emphysema
- Bullae rupture → prolonged air leaks, pleural and parenchymal infections
- Ultrastructural evidence: air leaks through bulla wall with mesothelial cell sloughing; CT density measures suggest valve-like air-trapping mechanism
- Management: Tube thoracostomy → VATS pleurodesis (mechanical abrasion); bullectomy at time of pleurodesis if minimal surrounding emphysema
B. Infected Bulla
- Clinical: Fever, cough, purulent sputum, dyspnea, pleuritic pain, leukocytosis
- Radiology: Air-fluid level within bulla
- Organisms: MRSA, Bacteroides, Pseudomonas aeruginosa, mycobacteria
- Treatment: Empiric antibiotics (as per CAP-COPD regimen); prolonged course; parenteral or intrabulla instillation
- If no improvement → CT-guided percutaneous aspiration (risk: pneumothorax, empyema); tube thoracostomy; endoscopic drainage
- Infected bulla is associated with bronchogenic cancer — follow with interval CXR
C. Bronchogenic Carcinoma
- Significantly increased incidence of lung cancer with bullous disease
- Mechanisms: fibrotic lung predisposition; dystrophic changes; carcinogen retention in poorly ventilated bullae
- CT features suggesting malignancy in bulla:
- Nodule/mass extruding from bulla wall
- Nodule confined within bulla lumen
- Soft tissue thickening of bulla wall
- Pneumothorax from erosion
- Air-fluid level
- Classification system (4 types): abutting cyst wall / protruding into lumen / wall thickening / multicystic
- Wall thickening/mural nodule developing after median 35 months on serial CT — surveillance required
D. Haemorrhage
- Rare; may follow air travel (expansion at altitude)
E. Vanishing Lung / Progressive Compression
- Progressive enlargement compresses contralateral normal lung, mediastinal shift
8. SURGICAL MANAGEMENT (BULLECTOMY)
Indications for Bullectomy
Absolute: Tension pneumothorax or recurrent pneumothorax with bulla
Strong (from Fishman's Table 50-3):
- Progressive dyspnea
- Bulla occupying >50% of hemithorax (or >1/3 — giant)
- CT showing compressed but viable adjacent lung
- FEV₁ and DLCO that are discordantly better than expected from CT findings
- Relatively preserved elastic recoil in non-bullous lung
Contraindications to Bullectomy
| Relative Contraindications |
|---|
| PaCO₂ >45 mmHg |
| Severe obstructive disease (FEV₁ <35% predicted with diffuse emphysema) |
| Diffuse bilateral bullous emphysema without dominant bulla |
| Severe pulmonary hypertension |
| BMI <18 or severe nutritional depletion |
Pre-operative Assessment
- Spirometry (FEV₁, FVC, TLC, RV)
- DLCO
- ABG
- HRCT for bulla mapping
- V/Q scan — assess functional residual lung
- Echocardiography — exclude pulmonary hypertension
- Exercise tolerance testing
Surgical Techniques
- Video-Assisted Thoracoscopic Surgery (VATS) — preferred; endoscopic stapling of bullae neck
- Open bullectomy (thoracotomy) — for giant or complex bullae
- Brompton technique — plication and oversewing of bullae without resection (historic)
- Intracavitary drainage — Monaldi procedure (historic, for inoperable patients): drainage tube into bulla via chest wall
Post-operative Results
- Improvement in FEV₁, FVC, exercise capacity, and dyspnea in well-selected patients
- Respiratory muscle strength (maximal inspiratory pressure) improves post-bullectomy
- Best results: isolated giant bulla with preserved surrounding lung; FEV₁ may double
- Poor results: diffuse bilateral emphysema with multiple small bullae
9. KEY DIFFERENTIALS
| Condition | Key Distinguishing Features |
|---|---|
| Tension pneumothorax | Absent lung markings to periphery; tracheal deviation; no bulla wall visible |
| Bronchogenic cyst | Epithelial-lined; may be fluid-filled; mediastinal location |
| Hydatid cyst | Water-lily sign; eosinophilia; serology |
| Pneumatocoele | Post-pneumonic (staph), thin-walled, transient, in children |
| Congenital lobar emphysema | Neonates/infants; overinflated lobe without wall destruction |
| Lung abscess | Thick, irregular wall; air-fluid level; systemic sepsis |
10. SUMMARY POINTS FOR EXAM
- Bulla >1 cm; bleb subpleural between visceral pleural layers; cyst has epithelial lining
- Upper lobe predominance due to greater apical mechanical stress
- Two major risk factors: cigarette smoking and α₁-AT deficiency
- Bullous disease = bullae in otherwise normal lungs; different from bullous emphysema
- DLCO best functional test; discordant preservation (DLCO > expected) = better surgical outcome
- PaCO₂ >45 mmHg = relative contraindication to bullectomy
- CT is gold standard for evaluation; V/Q scan assesses adjacent lung function
- Infected bulla: air-fluid level on CXR; organisms include MRSA, Pseudomonas, mycobacteria
- Bronchogenic cancer association: wall thickening, mural nodule on CT — surveillance mandatory
- VATS bullectomy is current standard; best outcome when dominant bulla compresses viable adjacent lung
References: Fishman's Pulmonary Diseases and Disorders, 2-Volume Set, Chapter 50 (Fernando J. Martinez); Murray & Nadel's Textbook of Respiratory Medicine, 2-Volume Set — Chapters on Emphysema and Diving Medicine.
This is a shared conversation. Sign in to Orris to start your own chat.