Why PO2 normal in carboxyhemobloginemia
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Here is a thorough explanation, backed directly by the textbook sources:
Why PO2 is Normal in Carboxyhemoglobinemia
The Core Concept
PO2 (partial pressure of oxygen) measures only dissolved oxygen in plasma - the tiny free fraction floating unbound in the liquid phase of blood. It does NOT measure oxygen carried by hemoglobin.
In carboxyhemoglobinemia (CO poisoning), carbon monoxide binds hemoglobin (forming HbCO/COHb) but has absolutely no effect on the small amount of oxygen dissolved in plasma. Since the lungs are still ventilating normally and the patient is breathing room air (or oxygen), dissolved oxygen in plasma remains perfectly normal. The ABG machine reports PO2 from this dissolved fraction - so it comes back normal.
Mechanisms in Detail
1. What CO actually does to hemoglobin:
CO binds hemoglobin with an affinity ~200 times greater than oxygen. This causes two problems:
- The HbCO molecules are unavailable for O2 transport (functional anemia - less Hb to carry O2)
- The remaining unaffected Hb subunits bind O2 more tightly - shifting the oxyhemoglobin dissociation curve sharply to the left (see diagram below)
The net result: even though PO2 is normal, tissues are starved of oxygen because Hb cannot offload what little O2 it carries.
(Source: Miller's Anesthesia, 10e)
2. Why the ABG machine misleads you:
Standard ABG analyzers directly measure pH, PCO2, and PO2. They then calculate oxygen saturation (SaO2) using a formula that assumes:
- A normal Hb-O2 dissociation curve
- Normal 2,3-DPG
- No abnormal hemoglobins
When HbCO is present, this calculation is wildly inaccurate. The machine "calculates" a falsely normal or high SaO2 because it sees a normal PO2 and assumes all Hb is normal. (Quick Compendium of Clinical Pathology, 5e)
3. Why the pulse oximeter also lies:
The standard 2-wavelength pulse oximeter measures only oxyhemoglobin (HbO2) vs. deoxyhemoglobin absorbance. It cannot distinguish HbCO from HbO2 (both absorb similarly at 660 nm). So it reads HbCO as "saturated hemoglobin" and overestimates SpO2. (Quick Compendium of Clinical Pathology, 5e)
The Oxyhemoglobin Dissociation Curve in CO Poisoning
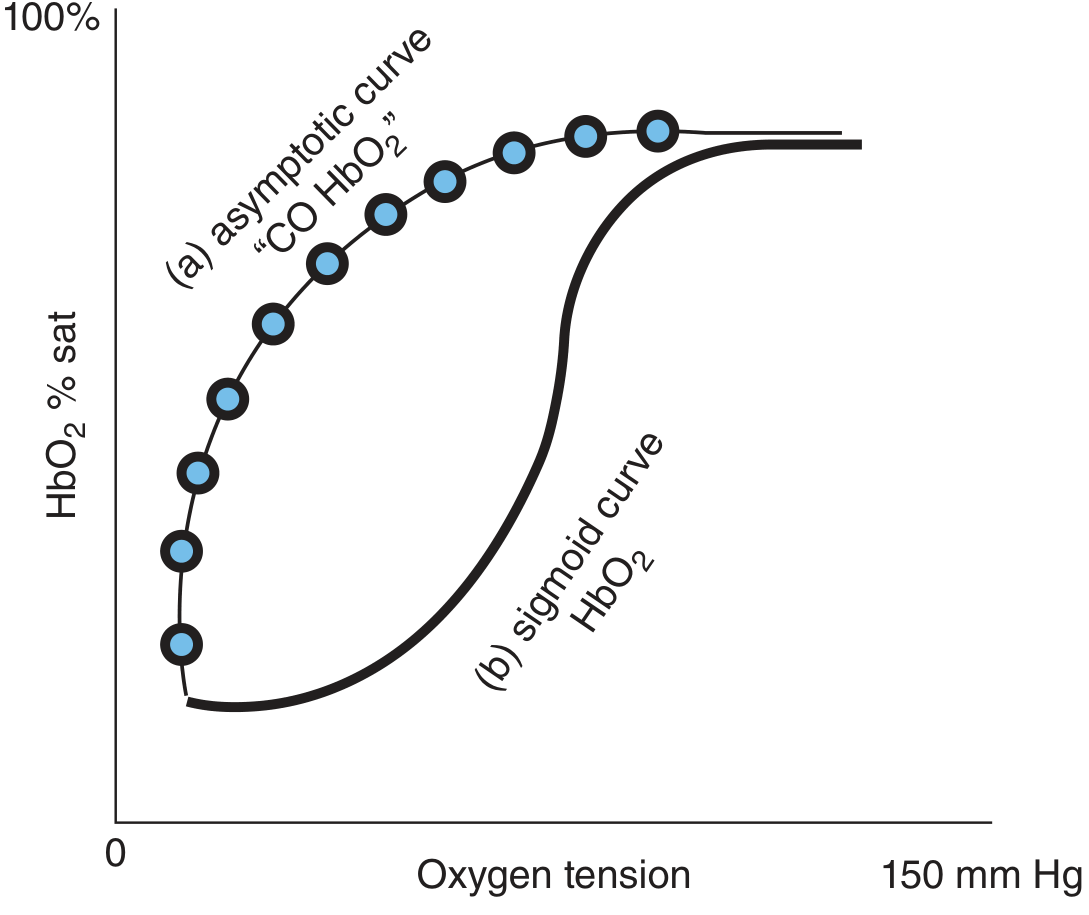
Fig: (a) CO-affected HbO2 dissociation curve - asymptotic shape; (b) normal sigmoid HbO2 curve. At a given tissue PO2, much less O2 is released from Hb in CO poisoning. - Tintinalli's Emergency Medicine
Summary Table
| Parameter | In CO Poisoning | Why |
|---|---|---|
| PaO2 | Normal | Dissolved O2 in plasma unaffected; lungs still oxygenating plasma |
| SpO2 (pulse ox) | Falsely normal/high | Cannot distinguish HbCO from HbO2 |
| Calculated SaO2 (ABG) | Falsely normal | ABG assumes no abnormal Hb |
| Measured SaO2 (co-oximetry) | LOW | Directly measures all Hb species |
| COHb level | ELEVATED | Confirms diagnosis |
| O2 content of blood | LOW | Hb occupied by CO, less O2 carried |
Clinical Pearl
The diagnosis is confirmed by finding an elevated HbCO level in arterial or venous blood. PO2 levels on blood gas may be normal even in the presence of CO poisoning - carboxyhemoglobin levels must be specifically measured.
- Pfenninger and Fowler's Procedures for Primary Care; Miller's Anesthesia, 10e
The only way to detect CO poisoning accurately is co-oximetry (a 4+ wavelength analyzer), which directly measures HbCO, methemoglobin, oxyhemoglobin, and deoxyhemoglobin separately.
DVT
Asking for Preferences
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Here is a complete overview of DVT:
Deep Vein Thrombosis (DVT)
Anatomy
DVT forms in the deep venous system of the lower extremities (most common site) but can also occur in arm veins, iliac veins, and rarely in jugular, mesenteric, portal, or cerebral veins.
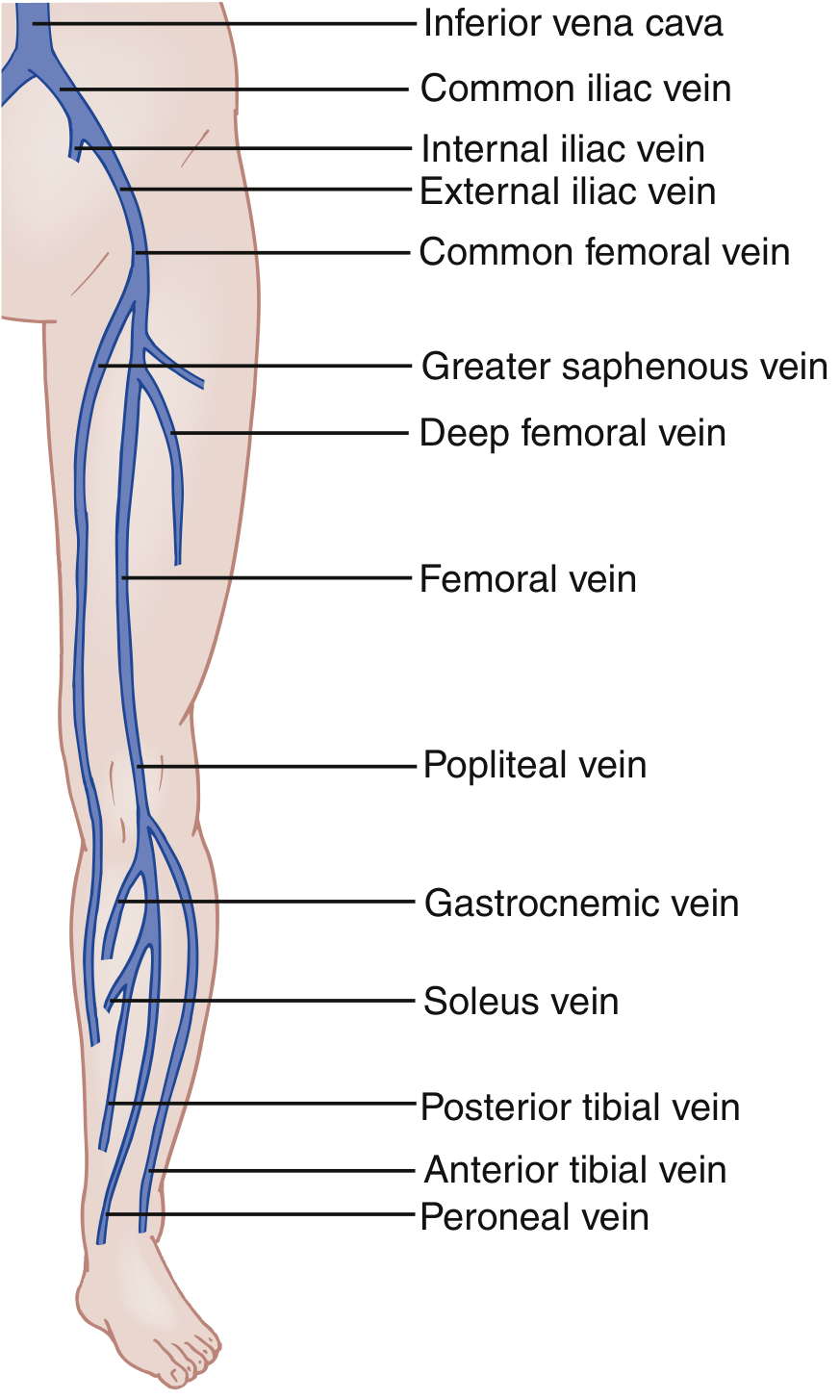
Terminology by location:
- Distal DVT - clot isolated to calf veins (ant. tibial, post. tibial, peroneal)
- Proximal DVT - popliteal vein and above (higher risk of embolization)
- Iliofemoral DVT - most proximal, highest risk
- 90% of DVT form in leg veins; 10% in upper extremities or other sites (Rosen's Emergency Medicine)
Pathophysiology - Virchow's Triad
DVT forms when the propensity of blood to coagulate overwhelms endogenous anticoagulant and fibrinolytic systems. Three interacting mechanisms drive this:
| Component | Mechanism |
|---|---|
| Venous stasis | Slow flow allows clotting factors to accumulate; seen in immobility, post-surgery, CHF |
| Endothelial injury | Exposes subendothelial tissue factor, activating coagulation; seen in trauma, surgery, inflammation |
| Hypercoagulability | Inherited (Factor V Leiden, protein C/S deficiency) or acquired (cancer, pregnancy, OCP use, antiphospholipid syndrome) |
In most cases, multiple factors act synergistically - a single factor alone rarely causes clinically significant thrombosis. (Miller's Anesthesia, 10e; Murray & Nadel's Respiratory Medicine)
Initiation of clot: Monocytes expose tissue factor on their surfaces, overwhelming natural anticoagulant mechanisms, leading to aggregation of RBCs, platelets, and fibrin in the venous sinuses and valve cusps. The resulting clot causes vascular congestion, valve incompetence, stasis, and further propagation. (Rosen's Emergency Medicine)
Risk Factors
| Risk Factor | Virchow's Mechanism | Strength |
|---|---|---|
| Surgery (within 4 weeks, under general anesthesia) | Inflammation, venous injury, stasis | ++++ |
| Prior PE or DVT | Hypercoagulability, stasis (valve damage) | ++ |
| Active cancer | Hypercoagulability | ++ |
| Inherited or acquired thrombophilia | Hypercoagulability | ++ |
| Prolonged immobility / bed rest | Stasis | ++ |
| Pregnancy | All three components (Virchow's triad) | + |
| Estrogen use (OCP, HRT) | Hypercoagulability | + |
| Older age | Multiple mechanisms | + |
| Long-haul travel | Stasis | + (weak) |
Note: ~50% of PE/DVT patients have no apparent risk factor at diagnosis. Between 4-11% are found to have a new cancer diagnosis within 1 year of an idiopathic VTE event. (Rosen's Emergency Medicine)
Clinical Features
Symptoms are often subtle and nonspecific. Many DVTs are clinically silent.
Symptoms:
- Unilateral leg pain, cramping, or "fullness" in calf
- Leg swelling (unilateral)
- Warmth and erythema of the limb
Signs:
- Pitting edema of the affected limb
- Tenderness along the deep venous system
- Dilation of superficial collateral veins
- Rarely: a palpable venous cord
- Homans' sign (calf pain on dorsiflexion) - positive in some cases, but is neither sensitive nor specific and should NOT be relied upon
Left-sided DVT is slightly more common because the left iliac vein is vulnerable to compression by the left iliac artery - this is May-Thurner syndrome.
Upper extremity DVT: >90% occur with an indwelling catheter/pacemaker wire. In young athletes without a device, Paget-Schroetter syndrome (effort-induced thoracic outlet syndrome) should be considered.
Differential Diagnosis
- Venous insufficiency / chronic venous congestion
- Cellulitis (concurrent DVT is present in only ~3% of cellulitis cases)
- Muscle/tendon injury (gastrocnemius tear, Achilles injury)
- Ruptured Baker cyst - can mimic DVT very closely
- Calf hematoma
- Asymmetrical edema (CHF, liver disease, hypoalbuminemia)
Diagnosis
Step 1: Pretest Probability (Wells DVT Score)
| Clinical Feature | Points |
|---|---|
| Active cancer | +1 |
| Paralysis, paresis, or recent leg plaster immobilisation | +1 |
| Recently bedridden >3 days OR major surgery within 12 weeks | +1 |
| Localized tenderness along deep venous system | +1 |
| Entire leg swollen | +1 |
| Calf swelling >3 cm vs contralateral | +1 |
| Pitting edema confined to symptomatic leg | +1 |
| Collateral superficial veins | +1 |
| Alternative diagnosis at least as likely | -2 |
Score interpretation:
- Low PTP: score -2 to 0
- High PTP: score ≥1 (or ≥3 for strict 3-tier)
Step 2: D-Dimer
- Measures enzymatic breakdown of cross-linked fibrin from any intravascular thrombus
- Sensitivity ~92%, specificity ~45% for excluding proximal DVT in low PTP patients
- Normal D-dimer + low PTP = DVT effectively excluded
- Age-adjusted cutoff: Age × 10 ng/mL (e.g., 800 ng/mL for an 80-year-old) - safely reduces need for ultrasound while maintaining ~95% sensitivity
- D-dimer is elevated in many non-DVT conditions: pregnancy, cancer, infection, recent surgery, trauma
Step 3: Imaging
- Venous compression ultrasound - gold standard; non-compressible vein = DVT
- 3-point US: common femoral, femoral, popliteal
- Whole-leg US adds calf veins
- MR venography - useful for pelvic vein DVT (e.g., gynecologic malignancy)
- High PTP + positive D-dimer + negative proximal US → repeat US in 1 week (to detect distal DVT that may propagate)
Key Complications
- Pulmonary Embolism (PE) - the most feared complication; clot fragments travel through right heart into pulmonary arteries
- Post-thrombotic syndrome - chronic venous insufficiency, edema, skin changes, ulceration; more common with proximal DVT
- Phlegmasia cerulea dolens - massive DVT causing near-total venous occlusion; limb-threatening ischemia
Special Populations
- Pregnancy: Wells score not validated; use LEFt score (Left leg, Edema, first Trimester). Heparin (not warfarin) is the anticoagulant of choice.
- Cancer patients: High risk; extended anticoagulation typically required; DOACs (rivaroxaban, apixaban) now preferred over LMWH in many cancers.
(Sources: Rosen's Emergency Medicine; Bailey and Love's Surgery, 28e; Murray & Nadel's Respiratory Medicine; Miller's Anesthesia, 10e)
This is a shared conversation. Sign in to Orris to start your own chat.