Management Of Heart Failure
Reading File
Finding Sources
Finding Sources
Searching PubMed
"heart failure" AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Searching Images
heart failure management algorithm treatment guidelines
Reading File
Finding Sources
Reading File
I now have comprehensive, authoritative information from multiple textbooks. Let me compile a complete, structured response.
Management of Heart Failure
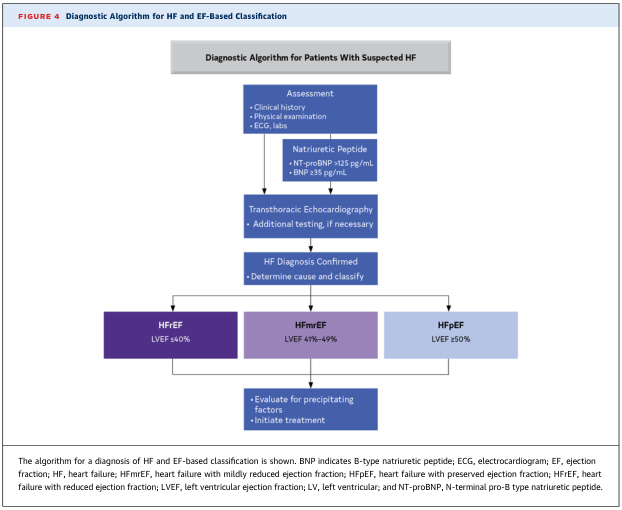
Classification & Diagnosis Framework
Heart failure (HF) is a clinical syndrome in which the heart cannot pump blood at a rate commensurate with tissue requirements, or can do so only at elevated filling pressures. Before initiating treatment, patients are classified by ejection fraction and ACC/AHA stage:
| EF Category | LVEF | Formerly |
|---|---|---|
| HFrEF (reduced) | ≤ 40% | Systolic HF |
| HFmrEF (mildly reduced) | 41–49% | — |
| HFpEF (preserved) | ≥ 50% | Diastolic HF |
ACC/AHA Stages (A → D, progressive):
- Stage A: High risk, no structural disease (HTN, DM, CAD)
- Stage B: Structural disease, no symptoms
- Stage C: Structural disease with current/prior symptoms → active GDMT
- Stage D: Refractory to GDMT → advanced therapies (LVAD, transplant)
General Non-Pharmacological Measures
- Sodium restriction and daily fluid monitoring
- Weight reduction, regular physical activity as tolerated
- Abstinence from alcohol, tobacco, and illicit drugs
- Optimise comorbidities: HTN, diabetes, dyslipidaemia, AF
- Vaccination (influenza, pneumococcal)
- Patient education and adherence counselling
"Before patients with chronic heart failure are referred for heart transplantation or MCS therapies, they are treated medically with a combination of lifestyle modification and GDMT." — Sabiston Textbook of Surgery
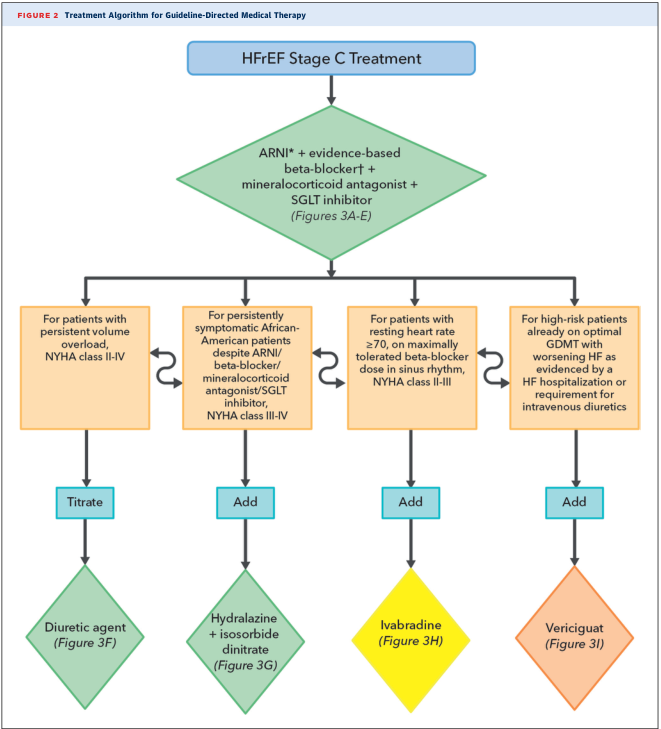
HFrEF (LVEF ≤ 40%) — Pharmacological Management
Foundational Quadruple Therapy (GDMT)
The 2022 AHA/ACC/HFSA guidelines, reflected in all major textbooks, endorse four pillars of therapy that each independently reduce mortality:
| Pillar | Drug Class | Examples | Key Benefit |
|---|---|---|---|
| 1 | RAAS inhibitor / ARNI | Sacubitril/valsartan (ARNI preferred); or ACEi/ARB if ARNI not tolerated | Reduces mortality; reverses remodelling |
| 2 | β-blocker (evidence-based) | Carvedilol, metoprolol succinate, bisoprolol | Reduces mortality; slows progression |
| 3 | MRA (mineralocorticoid receptor antagonist) | Spironolactone, eplerenone | Reduces morbidity and mortality |
| 4 | SGLT2 inhibitor | Dapagliflozin, empagliflozin | Reduces HF hospitalisations and CV death |
"Four evidence-based therapies have been shown to improve outcomes in patients with reduced EF heart failure: renin-angiotensin-aldosterone inhibitors with or without a neprilysin inhibitor, β-adrenergic receptor blockers, mineralocorticoid-receptor antagonists, and an SGLT2 inhibitor." — Sabiston Textbook of Surgery
ARNI vs ACEi:
Sacubitril/valsartan (ARNI) is preferred over ACEi in eligible patients. ACEi/ARB are alternatives when ARNI is not tolerated or available. Never combine ARNI with ACEi (risk of angioedema); a 36-hour washout is required when switching from ACEi.
Sacubitril/valsartan (ARNI) is preferred over ACEi in eligible patients. ACEi/ARB are alternatives when ARNI is not tolerated or available. Never combine ARNI with ACEi (risk of angioedema); a 36-hour washout is required when switching from ACEi.
Volume Management: Diuretics
- Loop diuretics (furosemide, torsemide, bumetanide): first-line for congestion/oedema; required in most Stage C patients
- Thiazides (hydrochlorothiazide): mild cases only; synergistic with loop diuretics for diuretic resistance
- Diuretics reduce symptoms but have not been shown to reduce mortality independently
- Monitor for hypokalaemia — supplement potassium or add ACEi/MRA
Add-On Therapies in Selected Patients
| Drug | Indication | Notes |
|---|---|---|
| Hydralazine + Isosorbide dinitrate | Self-identified African-American patients NYHA III–IV despite quadruple therapy; also if RAAS inhibitors not tolerated | Shown to reduce mortality in ISDN/Hyd combination |
| Ivabradine | Sinus rhythm, resting HR ≥ 70 bpm, on max tolerated β-blocker dose, NYHA II–III | Reduces HF hospitalisations |
| Vericiguat | High-risk patients (recent HF hospitalisation or IV diuretic use) on optimal GDMT | sGC stimulator; reduces HF events |
| Digoxin | Persistent symptomatic HF or AF with rapid ventricular rate | Reduces symptoms and rehospitalisation; does not reduce mortality |
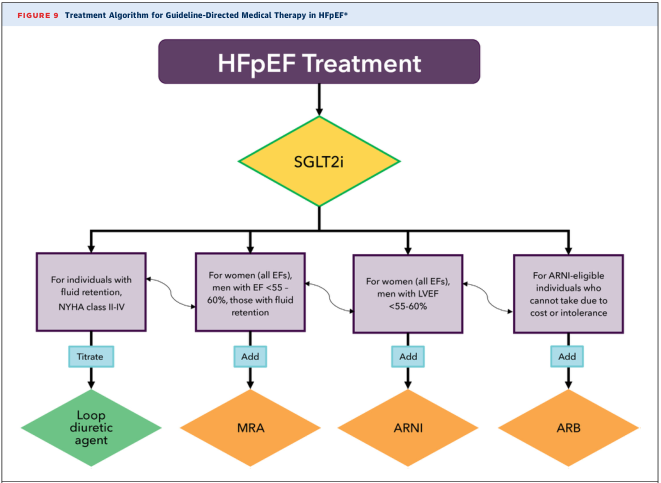
HFpEF (LVEF ≥ 50%) — Management
HFpEF management remains less well-defined, but recent guidelines now recommend a treatment hierarchy:
- SGLT2 inhibitors — now considered first-line for all HFpEF patients (empagliflozin, dapagliflozin; reduce HF hospitalisations)
- Loop diuretics — titrated for fluid retention and symptom relief (NYHA II–IV)
- MRA (spironolactone) — added for women (all EFs) and men with EF < 55–60%
- ARNI (sacubitril/valsartan) — added for those eligible; reduces symptoms and NT-proBNP
- ARB — for those unable to tolerate ARNI (cost or intolerance)
- Treat underlying causes: control HTN aggressively, treat dyslipidaemia, consider revascularisation for CAD, rate control of AF
"SGLT2 inhibitors are now considered first-line therapy for HFpEF." — Katzung's Basic and Clinical Pharmacology
Key differences from HFrEF:
- Non-dihydropyridine CCBs and β-blockers useful for HR and BP control
- Nitrates require caution (may cause excessive preload reduction)
- Positive inotropes are not recommended
Acute Decompensated Heart Failure (ADHF)
Common triggers: excess salt/fluid intake, non-adherence to medications, infections, arrhythmia (especially new AF), acute MI, anaemia, NSAIDs.
Management Priorities (IV therapy is the rule)
| Agent | Role |
|---|---|
| IV furosemide (high-dose) | First-line for acute decongestion; acetazolamide add-on improves diuresis |
| IV nitroprusside / nitroglycerin / nesiritide | Vasodilators — reduce preload and afterload; useful when BP is preserved |
| IV dobutamine / dopamine | Positive inotropes for low output / hypotension; prompt onset, short duration |
| Levosimendan | Calcium sensitiser; non-inferior to dobutamine (approved in Europe) |
| Vasopressin antagonists (tolvaptan, conivaptan) | Dilutional hyponatraemia in ADHF; aquaretic effect without worsening renal function |
"Among diuretics, furosemide is most commonly used, usually at high dosage. A recent study suggests that addition of acetazolamide to standard high-dose furosemide has an important additive benefit." — Katzung's Basic and Clinical Pharmacology
For ADHF precipitated by acute MI: emergency revascularisation (PCI with stent or thrombolysis) is the priority.
Device Therapy
| Device | Indication |
|---|---|
| ICD (implantable cardioverter-defibrillator) | HFrEF LVEF ≤ 35%, NYHA II–III, expected survival > 1 year; sudden death prevention |
| CRT (cardiac resynchronisation therapy) | Sinus rhythm, QRS ≥ 120–150 ms (LBBB morphology preferred), NYHA II–IV on GDMT; biventricular pacing improves synchrony, CO, and mortality |
| CRT-D | CRT + ICD combined; most patients with CRT indication |
| Transcatheter TEER (MitraClip) | Secondary/functional MR in patients with advanced HFrEF remaining symptomatic on GDMT |
"Patients with a wide QRS interval (> 120 ms) have impaired synchronization of ventricular contraction… Resynchronization with biventricular pacing has been shown to reduce mortality in patients with chronic heart failure already receiving optimal medical therapy." — Katzung's Basic and Clinical Pharmacology
Advanced / End-Stage HF (Stage D)
For patients refractory to GDMT and device therapy:
Left Ventricular Assist Device (LVAD)
- Bridge to transplantation or destination therapy
- Durable LVADs achieve average survival > 6 years
- Indications include inotrope dependence or inability to wean from temporary MCS
Heart Transplantation
- Definitive therapy for Stage D HF
- Indications: Stage D HF, MCS dependence, inotrope dependence, peak VO₂ ≤ 14 mL/kg/min (off β-blocker) or ≤ 12 mL/kg/min (on β-blocker)
- Absolute contraindication: PVR > 6 Wood units (consider heart-lung transplant)
- Relative contraindication: PVR 4–6 Wood units, age > 70, active malignancy
Summary Drug Table
| Drug Class | Representative Drugs | Mortality Benefit | Use |
|---|---|---|---|
| Loop diuretics | Furosemide, torsemide | ✗ | Symptoms/congestion |
| SGLT2 inhibitors | Dapagliflozin, empagliflozin | ✓ (HFrEF + HFpEF) | Both HF types |
| ACEi | Enalapril, lisinopril | ✓ (HFrEF) | First-line RAAS |
| ARB | Losartan, valsartan | ✓ (HFrEF) | ACEi intolerance |
| ARNI | Sacubitril/valsartan | ✓ (HFrEF + HFpEF) | Preferred over ACEi |
| β-blockers | Carvedilol, metoprolol succinate | ✓ (HFrEF) | All stable HFrEF |
| MRA | Spironolactone, eplerenone | ✓ (HFrEF) | NYHA II–IV |
| Hydralazine + ISDN | — | ✓ (select) | African-American; RAAS intolerance |
| Ivabradine | — | ✗ (↓ hospitalisation) | HR ≥ 70, sinus rhythm |
| Digoxin | — | ✗ (↓ rehospitalisation) | Symptomatic HFrEF, AF |
| Dobutamine/dopamine | — | ✗ | Acute decompensation |
| Levosimendan | — | ✗ | Acute decompensation (Europe) |
Recent Evidence (PubMed, 2024–2025)
A recent RCT + meta-analysis (DAPA ACT HF-TIMI 68, Circulation 2025, PMID 40884036) confirmed that dapagliflozin initiated during hospitalisation for HF is safe and beneficial — supporting early in-hospital initiation of SGLT2 inhibitors rather than waiting for outpatient stabilisation. This aligns with the guideline shift toward initiating all four pillars of GDMT as early as possible.
Sources:
- Katzung's Basic and Clinical Pharmacology, 16th Edition
- Sabiston Textbook of Surgery, Biological Basis of Modern Surgical Practice
- Goodman & Gilman's The Pharmacological Basis of Therapeutics
- Braunwald's Heart Disease, 2-Vol Set
- PMID 40884036 — Dapagliflozin in Hospitalised HF (Circulation, 2025)
This is a shared conversation. Sign in to Orris to start your own chat.