Colorectal carcinoma
Reading File
Finding Sources
Finding Sources
Searching PubMed
"colorectal cancer"[MeSH Terms] AND ("diagnosis" OR "treatment")
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have rich, comprehensive content from multiple authoritative textbooks. Let me compile the full, detailed response.
Colorectal Carcinoma
Epidemiology
Colorectal cancer (CRC) is the second most common cause of cancer death in the UK, with approximately 42,000 new diagnoses annually. About one-third arise in the rectum and two-thirds in the colon. It occurs more frequently in resource-rich countries, and men are more affected than women (56% vs. 44%). - Bailey and Love's Short Practice of Surgery, 28th Ed.
Distribution by Site
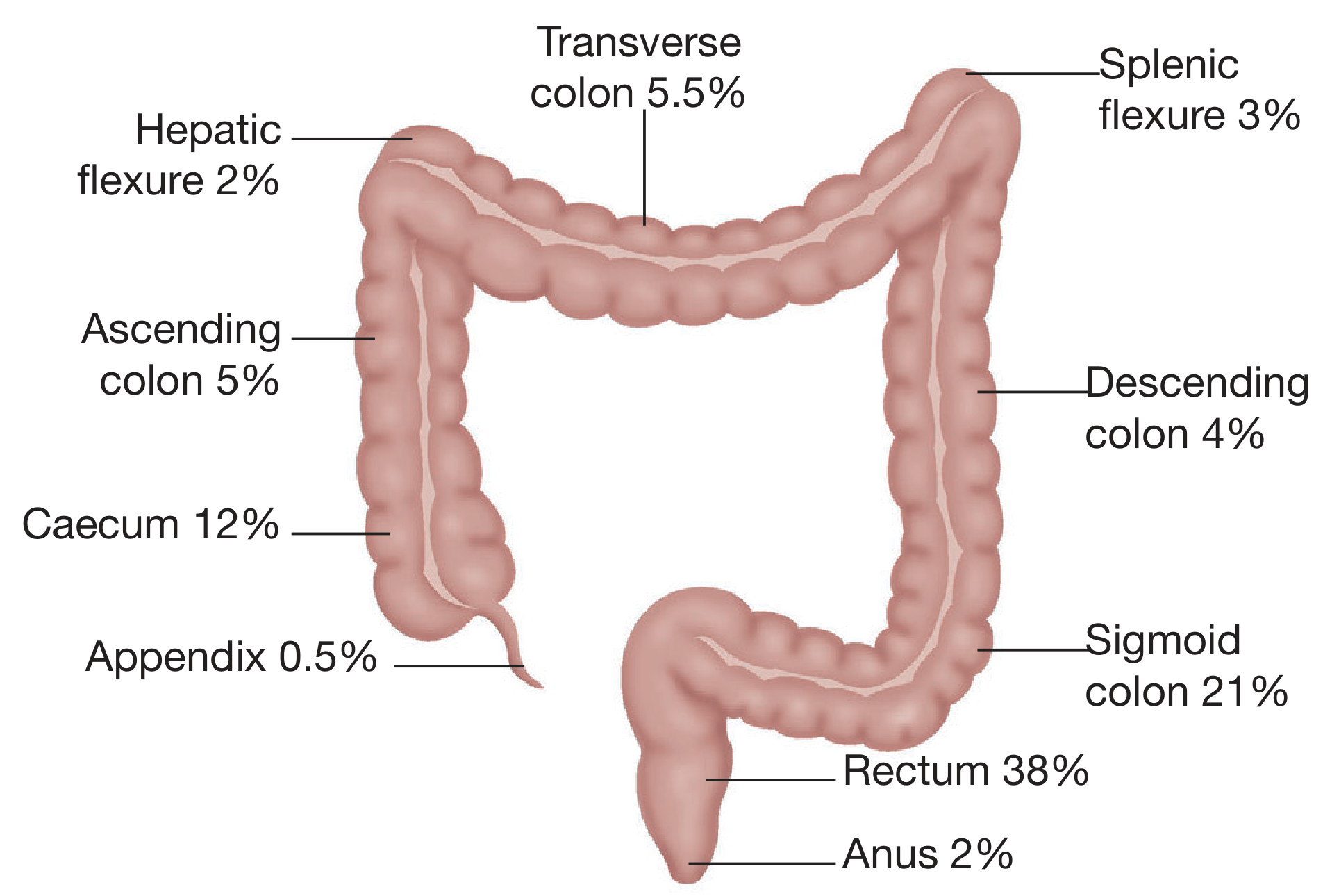
| Site | Frequency |
|---|---|
| Rectum | 38% |
| Sigmoid colon | 21% |
| Caecum | 12% |
| Ascending colon | 5% |
| Transverse colon | 5.5% |
| Descending colon | 4% |
| Splenic/Hepatic flexures | 2-3% |
| Appendix | 0.5% |
- Bailey and Love's Short Practice of Surgery, 28th Ed.
Aetiology and Risk Factors
Adenoma-Carcinoma Sequence
The vast majority of CRCs develop from adenomatous polyps through a sequence of genetic mutations influenced by environmental factors. Key evidence:
- Distribution of adenomas mirrors that of cancers (70% left-sided)
- Larger adenomas are more likely to be dysplastic
- Most early cancers have adjacent adenomatous tissue
- Adenomas are found in one-third of CRC resection specimens
- Incidence drops within colonoscopy-based screening programmes
Mutations in APC occur in ~two-thirds of colonic adenomas (early event), K-ras mutations are more common in larger lesions (intermediate event), and p53 mutation is a marker of invasion (late event). - Bailey and Love's
Three Major Molecular Pathways
| Pathway | Early Event | Progressive Events | Associated Syndrome |
|---|---|---|---|
| APC (Chromosomal Instability / LOH) | APC mutation (somatic or inherited) | KRAS, P53, DCC mutations | Conventional adenoma-to-carcinoma; sporadic + FAP |
| MMR (Microsatellite Instability) | MMR gene mutation (inherited) | KRAS, PIK3CA mutations | HNPCC (Lynch syndrome) |
| Methylator (CIMP) | Somatic BRAF mutation + MMR promoter methylation | Epigenetic silencing of TSGs | Serrated adenoma-associated carcinoma |
- Quick Compendium of Clinical Pathology, 5th Ed.
Consensus Molecular Subtypes (CMS)
A recent international consortium identified four CMS of CRC:
- CMS1: MSI-high, immune activation (right-sided, sporadic MSI)
- CMS2: WNT and MYC signalling activation
- CMS3: Metabolic dysregulation
- CMS4: TGF-beta activation - Bailey and Love's
Environmental/Lifestyle Risk Factors
- Red and processed meat (haem iron, N-nitroso compounds) - strong association worldwide
- Dietary fibre - protective (reduced colonic transit time, altered microbiota)
- Obesity, alcohol, smoking - increased risk
- Inflammatory bowel disease (IBD) - significant risk factor
- High calcium and magnesium intake - potentially protective
- Aspirin/NSAIDs (COX-2 inhibitors) - strong epidemiological evidence for protection
- Cholecystectomy may marginally increase right-sided colon cancer risk
Hereditary Syndromes
Familial Adenomatous Polyposis (FAP)
- Autosomal dominant; APC gene mutation on chromosome 5q (identified in 75% of FAP cases)
- Accounts for ~1% of all CRC
- Hundreds to thousands of polyps develop after puberty
- Lifetime risk approaches 100% by age 50 without intervention
- Extraintestinal: congenital hypertrophy of retinal pigmented epithelium, desmoid tumors, epidermoid cysts, mandibular osteomas (Gardner's syndrome), CNS tumors (Turcot's syndrome)
- Screening: Flexible sigmoidoscopy or APC gene testing from age 10-15 years
- Treatment: Surgical (total proctocolectomy + IPAA preferred; total abdominal colectomy + ileorectal anastomosis as alternative); COX-2 inhibitors (celecoxib, sulindac) may slow polyp development
HNPCC / Lynch Syndrome
- Autosomal dominant; mutations in mismatch repair (MMR) genes (MLH1, MSH2, MSH6, PMS2)
- Accounts for ~3% of CRC; lifetime CRC risk up to 80%
- Right-sided predominance; tends to be poorly differentiated but better prognosis than stage-matched sporadic CRC
- Associated with endometrial, ovarian, gastric, small bowel, urological tumors
- Diagnosed using Amsterdam criteria or Bethesda guidelines; confirmed by germline testing
Familial (Non-Syndromic)
- Accounts for 10-15% of CRC
- Average lifetime risk 6% (no family history) rises to 12% (one first-degree relative), 35% (two first-degree relatives)
- Diagnosis before age 50 in a relative significantly increases risk
- Schwartz's Principles of Surgery, 11th Ed.
Pathology
Macroscopic forms:
- Annular/constricting - obstructive symptoms predominant
- Ulcerating - bleeding predominant
- Polypoid/fungating - especially right colon
- Diffusely infiltrating
Microscopic: Predominantly columnar cell adenocarcinoma. Rarer types include mucinous adenocarcinoma, signet-ring cell carcinoma, squamous cell carcinoma, and undifferentiated carcinoma. - Bailey and Love's
Spread
- Direct/local: Longitudinal or radial extension into adjacent structures (ureter, duodenum, posterior abdominal wall, anterior abdominal wall)
- Lymphatic: Progressive from pericolic to intermediate to central nodes; orderly but not always predictable
- Haematogenous: Via the portal vein to the liver (most common; one-third of patients have liver metastases at diagnosis; 50% will eventually develop them). Lung is the next most common site. Ovaries, brain, kidney, bone less common
- Transcoelomic (peritoneal): To peritoneum, ovary (Krukenberg tumour), omentum
- Bailey and Love's
Staging
Dukes' Classification (Historical, Still Used)
| Stage | Definition |
|---|---|
| A | Tumour confined to bowel wall (not penetrating muscularis propria) |
| B | Tumour penetrates muscularis propria; no nodal involvement |
| C1 | Nodal metastases; apical node negative |
| C2 | Apical node positive |
| D | Distant metastases |
TNM Staging (International Standard)
T - Primary Tumour:
| Stage | Definition |
|---|---|
| Tis | Carcinoma in situ (intramucosal) |
| T1 | Invades submucosa |
| T2 | Invades muscularis propria |
| T3 | Through muscularis propria into pericolorectal tissues |
| T4a | Through visceral peritoneum |
| T4b | Invades/adheres to adjacent organs or structures |
N - Nodes:
| Stage | Definition |
|---|---|
| N0 | No regional node metastasis |
| N1 | 1-3 positive nodes |
| N1a/b/c | 1 node / 2-3 nodes / tumor deposits with negative nodes |
| N2a | 4-6 positive nodes |
| N2b | 7 or more positive nodes |
M - Metastasis:
| Stage | Definition |
|---|---|
| M0 | No distant metastasis |
| M1a | Metastasis to 1 distant site/organ |
| M1b | Metastasis to 2+ sites/organs |
| M1c | Peritoneal metastasis |
- Schwartz's Principles of Surgery, 11th Ed.
Clinical Presentation
Symptoms depend on tumour location:
Right colon (caecum/ascending):
- Occult blood loss → iron-deficiency anaemia
- Vague abdominal discomfort
- Palpable mass (tumours can grow large before obstruction)
Left colon (descending/sigmoid) and rectum:
- Change in bowel habit (alternating constipation and diarrhoea)
- Rectal bleeding (bright red or dark)
- Tenesmus (especially rectal)
- Colicky abdominal pain
- Obstruction (more common than right-sided due to narrower lumen)
General/systemic features: weight loss, anorexia, fatigue (anaemia), perforation (rare, peritonitis)
Investigations
Tumour Markers
- CEA (Carcinoembryonic Antigen): Not useful for diagnosis but important for monitoring after treatment and detecting recurrence. CEA >5 ng/mL post-resection suggests residual disease or recurrence. - Quick Compendium of Clinical Pathology
Endoscopy
- Colonoscopy is the investigation of choice: secures histological diagnosis, detects synchronous polyps or carcinomas (present in 3-5% of cases). Small risk of perforation (1:1000). - Bailey and Love's
Radiology
- CT colonography (virtual colonoscopy): Highly sensitive for polyps ≥6mm; less invasive but cannot biopsy
- CT chest/abdomen/pelvis: Standard for staging CRC
- MRI pelvis: Mandatory for rectal cancer local staging (assessing circumferential resection margin, mesorectal fascia involvement)
Molecular Testing
- MSI/MMR status: Predicts Lynch syndrome; also predicts response to immune checkpoint inhibitor (ICI) therapy; MSI-H tumours respond well to pembrolizumab
- KRAS/NRAS mutation testing: Predicts resistance to EGFR inhibitors (cetuximab, panitumumab) - wild-type RAS required for benefit
- BRAF V600E mutation: Poor prognosis in metastatic CRC; predictive of response to specific therapies
- Tumour Mutation Burden (TMB): High TMB predicts ICI response
- NTRK fusion: Rare (<1% CRC), usually MSI-H; specific tyrosine kinase inhibitor therapy available
- Bailey and Love's; Quick Compendium of Clinical Pathology
Screening
For average-risk adults (age ≥50), accepted strategies include:
- Annual FOBT/FIT (reduces CRC mortality by 33%, metastatic disease by 50%; specificity low - 90% of positives are false positives; must be followed by colonoscopy if positive)
- Stool DNA (e.g., Cologuard: 92% sensitive for CRC, 74% specific; every 1-3 years)
- Flexible sigmoidoscopy every 5 years (60-70% reduction in mortality)
- CT colonography every 5 years
- Colonoscopy every 10 years (gold standard) - Schwartz's
High-risk groups (FAP, Lynch, IBD, family history) require earlier and more frequent surveillance.
Surgical Treatment
Colon Cancer
- Right hemicolectomy: Caecum, ascending colon, hepatic flexure tumours (with ileocolic, right colic, right branch of middle colic vessels)
- Extended right hemicolectomy: Transverse/hepatic flexure cancers
- Left hemicolectomy: Descending colon
- Sigmoid colectomy / high anterior resection: Sigmoid and upper rectum
- Minimum of 12 lymph nodes required in resection specimen for adequate staging
- Laparoscopic approach is oncologically equivalent to open surgery with faster recovery
Preoperative Preparation
- Mechanical bowel preparation combined with oral antibiotics reduces surgical site infections, anastomotic leak, ileus, reoperation, and mortality (used with ERAS protocols). - Bailey and Love's
Rectal Cancer
- Anterior resection: Upper rectum (above peritoneal reflection)
- Low anterior resection (LAR): Mid/lower rectum with total mesorectal excision (TME)
- Abdominoperineal resection (APR): Very low rectal cancers where sphincter preservation is not possible (permanent colostomy)
- TME is the standard for rectal cancer surgery - reduces local recurrence from ~30% to <10%
- Neoadjuvant (chemo)radiotherapy: For T3/T4 or node-positive rectal cancer prior to surgery
Systemic Treatment
Adjuvant Chemotherapy
- Stage III (node-positive) CRC: FOLFOX (5-FU/leucovorin + oxaliplatin) or CAPOX (capecitabine + oxaliplatin) - standard of care
- Stage II: Adjuvant chemotherapy reserved for high-risk features (T4, obstruction, perforation, inadequate node sampling, poor differentiation)
- FOLFIRI (5-FU + irinotecan): Alternative regimen for metastatic disease
Targeted Therapy in Metastatic CRC
| Agent | Target | Requirement |
|---|---|---|
| Cetuximab / Panitumumab | Anti-EGFR monoclonal antibody | Wild-type KRAS AND NRAS (mutations confer resistance) |
| Bevacizumab | Anti-VEGF | No specific biomarker required |
| Pembrolizumab | PD-1 checkpoint inhibitor | MSI-H or dMMR tumours |
| Encorafenib + cetuximab | BRAF + EGFR inhibition | BRAF V600E mutation |
| Larotrectinib / Entrectinib | TRK inhibitor | NTRK gene fusion |
- Bailey and Love's; Quick Compendium of Clinical Pathology
Note: Small molecule EGFR TKIs (gefitinib, erlotinib) have not shown benefit in CRC (unlike in lung cancer). Anti-EGFR monoclonal antibodies are the agents of choice. EGFR expression testing itself is not required - RAS testing is what matters.
Prognosis
5-year survival by stage:
| Dukes Stage | 5-Year Survival |
|---|---|
| A | ~90% |
| B | ~65-75% |
| C | ~30-40% |
| D | <10% |
Factors worsening prognosis: lymphovascular invasion, perineural invasion, poor differentiation, T4 stage, peritoneal involvement, emergency presentation (obstruction/perforation), BRAF V600E mutation in metastatic disease.
MSI-H tumours have better prognosis in early-stage disease but may have different behavior in metastatic setting.
Post-Treatment Surveillance
Following curative resection:
- CEA every 3 months for 2 years, then every 6 months to 5 years
- Colonoscopy at 1 year post-resection; if normal, every 3-5 years
- CT chest/abdomen/pelvis annually for 3-5 years (for high-risk stage II and stage III)
- Clinical assessment at each visit
Sources:
- Bailey and Love's Short Practice of Surgery, 28th Ed.
- Schwartz's Principles of Surgery, 11th Ed.
- Quick Compendium of Clinical Pathology, 5th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.