Varicocele
Reading File
Finding Sources
Searching PubMed
varicocele management treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Searching PubMed
varicocele infertility repair
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information from multiple authoritative sources. Here is a thorough synthesis:
Varicocele
Definition
A varicocele is an abnormal dilation and tortuosity of the veins within the pampiniform plexus of the spermatic cord — essentially varicose veins of the testis. It is the most common surgically correctable cause of male subfertility.
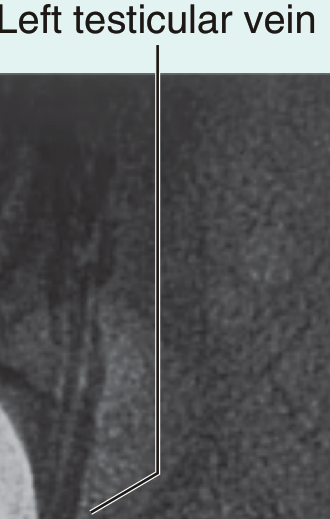
Left testicular venogram demonstrating the pampiniform plexus — Gray's Anatomy for Students
Epidemiology
| Population | Prevalence |
|---|---|
| Healthy young men (general) | ~15% |
| Subfertile men | ~40% |
| Adolescents | 8–16% |
| Bilateral (healthy men) | <10% |
| Bilateral (subfertile men) | Up to 20% |
- Varicoceles do not spontaneously regress.
- Most appear after age 10 and progress through puberty, peaking at Tanner stage 3.
- ~85% of men with varicocele in population-based studies have fathered children, so the individual impact on paternity is variable.
Anatomy & Pathogenesis
Left-sided predominance (>90% of cases)
- The left internal spermatic vein drains into the left renal vein at a right angle and is longer; the right drains obliquely into the inferior vena cava
- This geometry creates higher hydrostatic pressure on the left, predisposing to venous valve incompetence
- The "nutcracker phenomenon" (compression of the left renal vein between the aorta and superior mesenteric artery) contributes in some cases
⚠️ A solitary right-sided varicocele — especially of abrupt onset — should raise suspicion for a retroperitoneal mass (e.g., renal tumor). Evaluate with CT or abdominal ultrasound.
Mechanism of testicular damage (multifactorial):
- Elevated intratesticular temperature — disruption of countercurrent heat exchange in the pampiniform plexus (primary/most accepted theory)
- Oxidative stress — higher ROS in seminal fluid → increased sperm DNA fragmentation
- Venous stasis/hypoxia — pooling leads to toxin accumulation and hypoperfusion
- Hormonal dysfunction — pituitary-gonadal axis disruption
- Reflux of renal/adrenal metabolites via internal spermatic vein
- Elevated apoptosis-associated microRNA in seminal fluid
Clinical Features
- "Dragging feeling" or dull ache in the scrotum, typically worse at end of day or with exertion
- "Bag of worms" — classic tactile description of the dilated venous plexus
- May be asymptomatic (incidentally discovered)
- Testicular atrophy — affected testis may be smaller and softer; progressive atrophy is documented
Grading (Dubin-Amelar / Clinical System)
| Grade | Findings |
|---|---|
| 0 (Subclinical) | Not palpable; detected only on Doppler ultrasound (CDUS) |
| Grade I | Palpable only with Valsalva maneuver |
| Grade II | Easily palpable at rest; not visible |
| Grade III | Visible through scrotal skin; does not collapse supine |
Examine standing and supine. Veins should decompress in the supine position — failure to decompress (especially on the right) warrants imaging to rule out abdominal/pelvic mass.
Investigations
- Physical examination: Primary diagnostic tool
- Colour Doppler Ultrasound (CDUS): Used when examination is uncertain; detects retrograde blood flow and vein diameter; also assesses testicular volume
- Semen analysis: Abnormalities in concentration, motility (most profound), and morphology
- Venography: Gold standard for anatomical mapping but reserved for interventional planning
Effects on Fertility
- Semen parameters are poorer in men with varicocele vs. fertile population (WHO, 1992)
- Testicular atrophy progresses over time if untreated
- Sperm DNA fragmentation is elevated
- In adolescents, testicular volume discrepancy ≥20% between the two testes is a key surgical trigger
Treatment
Indications for intervention
- Adult: Palpable varicocele + abnormal semen parameters + subfertility
- Adolescent: Testicular volume discrepancy ≥20% on ultrasound; if volumes are stable and symmetric → annual surveillance ultrasound
- Symptomatic (pain/discomfort) regardless of fertility status
Surgical approaches
| Method | Details |
|---|---|
| Microsurgical subinguinal (gold standard) | Operating microscope preserves lymphatics → post-surgical hydrocele risk <1%; arteries spared |
| Inguinal (open) | Aponeurosis of external oblique divided; veins ligated |
| Laparoscopic | Less common; useful in bilateral cases |
| Percutaneous embolization | Catheter via right femoral vein → left renal vein → testicular vein; metal coils deployed; collateral drainage preserved |
Outcomes
Varicocele repair improves:
- Semen parameters (concentration, motility, morphology)
- Pregnancy rates and live birth rates
- Sperm DNA fragmentation
- Allows couples to step down to less invasive ART when indicated
Recent Evidence
Two recent systematic reviews (2024–2025) are relevant:
- [PMID 38877692] — Meta-analysis (2024): Varicocele repair improves sperm parameters, FSH, and LH in infertile males with azoospermia
- [PMID 39776560] — Systematic review (2025): Varicocele repair is supported for severe oligoasthenoteratozoospermia (OAT syndrome) across multiple published guidelines
Sources: Campbell-Walsh-Wein Urology | Smith & Tanagho's General Urology, 19e | Mulholland & Greenfield's Surgery, 7e | Gray's Anatomy for Students
Forniers gangrene
Finding Sources
Searching PubMed
Fournier gangrene necrotizing fasciitis
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Searching PubMed
Fournier gangrene mortality outcomes treatment
Loading Image
Reading File
Searching PubMed
Fournier gangrene management debridement
Comprehensive data assembled. Here is the full synthesis:
Fournier's Gangrene (FG)
Definition
Fournier's gangrene is a polymicrobial, synergistic, necrotizing fasciitis of the perineal, genital, and perianal regions — a urological and surgical emergency carrying significant mortality. Originally described by Baurienne (1764) and later by Jean-Alfred Fournier (1883) as an idiopathic fulminant scrotal gangrene in young healthy men, it is now understood to affect a broad age range and has an identifiable source in ~95% of cases.

Fournier's gangrene of the scrotum — Tintinalli's Emergency Medicine
Epidemiology
- Classically affects men ≥45 years, but women account for 10–25% of cases
- Diabetes mellitus present in 32–66% of patients
- Chronic alcohol abuse in 25–50%
- Can occur in previously healthy, immunocompetent individuals
Sources / Aetiology
Infection arises from three primary anatomic sources:
| Source | Examples |
|---|---|
| Anorectal (most common) | Perianal abscess, fistula-in-ano, colorectal surgery, IBD |
| Urogenital | Urethral stricture, urethral instrumentation, urinary extravasation, UTI, periurethral abscess |
| Cutaneous | Scrotal/perineal trauma, Bartholin abscess (in women), skin infection |
Rarely, intra-abdominal infection can track to the perineum via inguinal canals.
Microbiology
Typically polymicrobial — a synergistic mix of:
- Gram-positive aerobes: Streptococcus pyogenes, Staphylococcus aureus
- Gram-negative aerobes: Escherichia coli, Klebsiella, Pseudomonas
- Anaerobes: Bacteroides spp., Clostridia, Corynebacteria
The synergy between aerobes (consuming O₂) and anaerobes creates a highly destructive microenvironment.
Pathophysiology
- Initial focus → cellulitis at perineum/perianal region
- Bacteria cause microthrombosis of subcutaneous vessels → ischaemia
- Tissue necrosis along fascial planes (Dartos, Colles, Buck's, Scarpa's fascia)
- Crepitus — from gas-forming organisms tracking through fasciae
- Disease extent is far greater than visible skin findings suggest
- Rapid progression to bacteraemia → sepsis → multi-organ failure → death
Fascial spread patterns:
- Urogenital source: spreads posteriorly along Buck's and Dartos fascia → Colles fascia; limited at the anal margin by Colles fascia attachment to the perineal body
- Anorectal source: spreads to perianal skin; can extend anteriorly
- Both can spread to the anterior abdominal wall, potentially reaching the clavicles
The testes are usually spared — their blood supply originates intra-abdominally from the gonadal vessels, not from local fascial vessels.
Clinical Features
Early (cellulitis phase)
- Genital/perineal pain (65%) — often out of proportion to visible findings ⚠️
- Pruritus, lethargy, fever (may be afebrile on arrival)
- Swelling (65%), erythema (35%)
- Up to 40% initially have no localized symptoms — only pain
Advanced
- Crepitus of inflamed tissues (pathognomonic — gas-forming organisms)
- Purple/black bullae and necrotic patches
- Foul-smelling necrotic lesions with grey skin discolouration
- Signs of severe systemic illness out of proportion to visible local extent
- Rapid progression from genitalia → perineum → abdominal wall (can occur within hours)
Diagnosis
Primarily clinical — do not delay treatment for imaging in obvious cases.
Imaging (when diagnosis uncertain)
| Modality | Finding |
|---|---|
| Bedside US | Scrotal wall thickening; "dirty shadowing" = air in tissues |
| CT (gold standard) | Gas tracking along fascial planes, fluid collections, extent of disease |
| Plain X-ray | Soft tissue gas (less sensitive) |
LRINEC Score (Laboratory Risk Indicator for Necrotizing Infection)
Used to distinguish necrotizing fasciitis from severe cellulitis:
| Parameter | Threshold | Points |
|---|---|---|
| CRP | >150 mg/L | 4 |
| WBC | 15–25 × 10³/µL | 1; >25 → 2 |
| Haemoglobin | 11–13.5 g/dL | 1; <11 → 2 |
| Sodium | <135 mmol/L | 2 |
| Creatinine | >1.6 mg/dL | 2 |
| Glucose | >180 mg/dL | 1 |
| Score | Risk | Probability of NF |
|---|---|---|
| <5 | Low | ~50% |
| 6–7 | Moderate | 50–75% |
| ≥8 | High | >75% |
PPV 92%, NPV 96% for necrotizing infection at score ≥6.
Management
FG is a surgical emergency — triad of:
1. Resuscitation
- Aggressive IV fluid resuscitation, haemodynamic stabilisation
- ICU admission postoperatively
2. Broad-spectrum antibiotics (empiric, immediate)
Cover gram-positive, gram-negative, and anaerobic organisms:
- Piperacillin-tazobactam 3.375–4.5 g IV q6h OR imipenem 1 g IV q24h OR meropenem 500 mg–1 g IV q8h
- Plus vancomycin (MRSA coverage)
- Add clindamycin 600–900 mg IV q8h or metronidazole 500 mg IV q8h (anaerobic synergy/toxin suppression)
3. Surgical debridement (cornerstone)
- Wide aggressive debridement of all nonviable tissue to healthy, bleeding margins
- Extent of disease is invariably greater than external appearance — do not be conservative
- Average 3–4 return trips to the operating room required (second look at 24–48 hrs mandatory)
- Testicles are almost always spared (intra-abdominal blood supply)
- Urinary diversion (suprapubic catheter) or fecal diversion (colostomy/endorectal tube) as needed
- Negative pressure wound therapy (VAC) — reduces hospitalisation time, accelerates wound healing
- Split-thickness skin grafting for large tissue defects post-infection control
4. Adjunctive therapies
- Hyperbaric oxygen (HBO): pre- and post-operative; several groups report favourable results but evidence shows no improvement in overall mortality — use is controversial
- Reconstructive surgery: staged approach after infection is fully controlled
Severity Scoring Tools
| Score | Purpose |
|---|---|
| Fournier Gangrene Severity Index (FGSI) | 9 physiological variables; predicts mortality |
| Ulludag FGSI | Modified FGSI incorporating age |
| Age-Adjusted Charlson Comorbidity Index (ACCI) | Comorbidity burden |
| Surgical Apgar Score (sAPGAR) | Intraoperative risk |
All are validated for guiding therapeutic decisions in FG.
Prognosis & Mortality
- Mortality historically reported 3–67%
- Contemporary estimates: 12–30%
- Historical reports as high as 67% (Schwartz's Surgery)
- Key predictors of death: age >60 and complications during treatment
- Survivors face months–years of disability; sexual dysfunction ~65%
- Long-term multidisciplinary follow-up required
Recent Literature (2024–2026)
- [PMID 41439154] — Umbrella review (2026, Eur Urol Open Sci): Müssgens et al. define the standard of care in Fournier's gangrene
- [PMID 38879239] — Review (2024): Multidisciplinary management emphasised
- [PMID 40455358] — Review (2025, Curr Urol Rep): Modern management update
Sources: Campbell-Walsh-Wein Urology | Sabiston Textbook of Surgery | Schwartz's Principles of Surgery, 11e | Tintinalli's Emergency Medicine | Mulholland & Greenfield's Surgery, 7e
This is a shared conversation. Sign in to Orris to start your own chat.