Head and neck
Asking for Preferences
Asking for Preferences
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
I now have comprehensive content. Here is a complete, well-illustrated overview of the Skull & Scalp anatomy.
Skull & Scalp — Anatomy
Source: Gray's Anatomy for Students
The Skull
The skull has 22 bones (excluding the ossicles of the ear). With the exception of the mandible, all bones are attached to each other by sutures — immovable fibrous joints — and collectively form the cranium.
Subdivisions of the Cranium
| Part | Description | Key Bones |
|---|---|---|
| Calvaria | Upper domed cap; encloses the brain | Paired temporal & parietal bones; parts of frontal, sphenoid & occipital |
| Cranial base | Floor of the cranial cavity | Sphenoid, temporal & occipital |
| Facial skeleton (viscerocranium) | Lower anterior part | Paired nasal, palatine, lacrimal, zygomatic, maxillae & inferior nasal conchae; unpaired vomer |
| Mandible | Lower jaw; not part of cranium | Mandible only |
The skull has 3 pairs of synovial joints: the two temporomandibular joints (TMJs) and the joints between the ossicles (malleus–incus, incus–stapes on each side).
Sutures
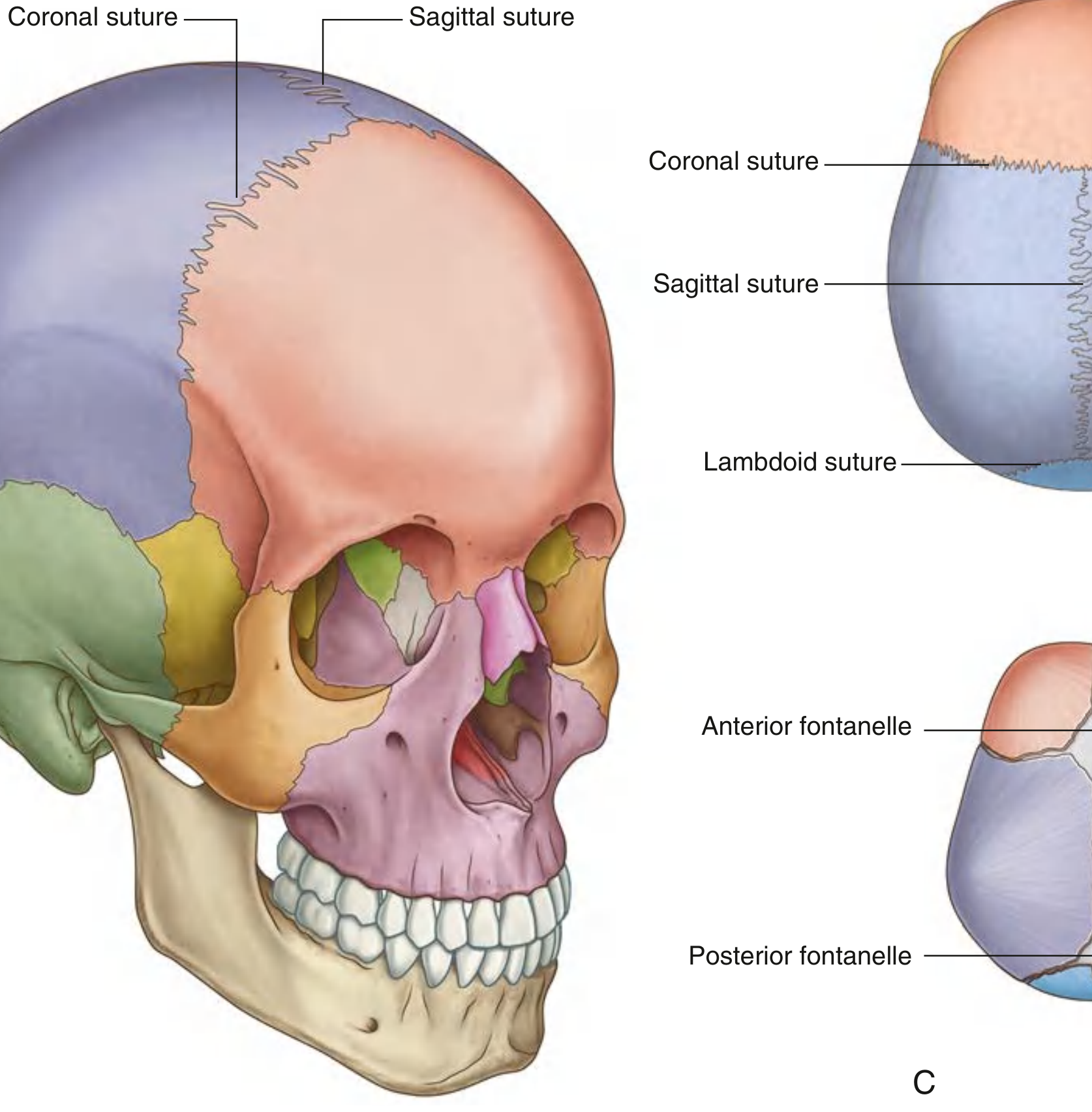
The major sutures are:
- Sagittal — between the two parietal bones (midline, superior)
- Coronal — between the frontal and parietal bones
- Lambdoid — between the parietal and occipital bones
In the fetus and newborn, gaps between these bones form fontanelles — membranous, unossified regions that allow head deformation during birth and postnatal brain growth. The anterior fontanelle (between frontal and parietal bones) closes around 18 months; the posterior fontanelle (between parietal and occipital) closes by 2–3 months.
Anterior View of the Skull
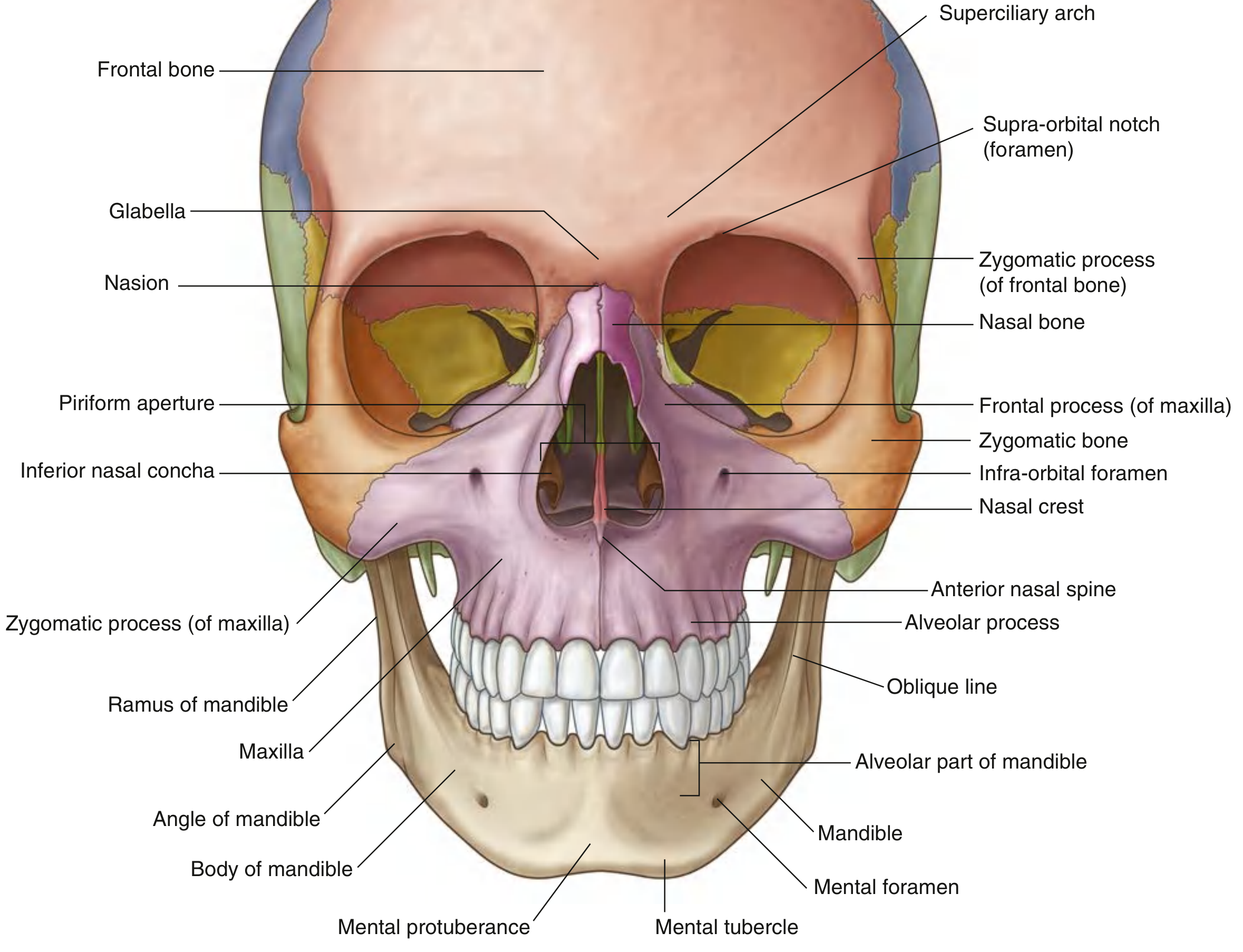
Key features from the anterior view:
| Structure | Significance |
|---|---|
| Frontal bone | Forms the forehead and superior orbital rims |
| Superciliary arches | Raised ridges above each orbit; more prominent in males |
| Glabella | Smooth midline depression between the superciliary arches |
| Supra-orbital foramen/notch | Transmits the supra-orbital nerve and vessels (CN V₁) |
| Infra-orbital foramen | Transmits the infra-orbital nerve and vessels (CN V₂) |
| Mental foramen | Transmits the mental nerve and vessels (CN V₃) |
| Nasal bones | Form the bony bridge of the nose |
| Zygomatic bone | Cheek prominence |
| Maxilla | Upper jaw, houses upper teeth |
| Mandible | Lower jaw; body, ramus, angle |
| Piriform aperture | Bony anterior nasal opening |
The Scalp
The scalp extends anteriorly from the superciliary arches, posteriorly to the external occipital protuberance and superior nuchal lines, and laterally down to the zygomatic arch.
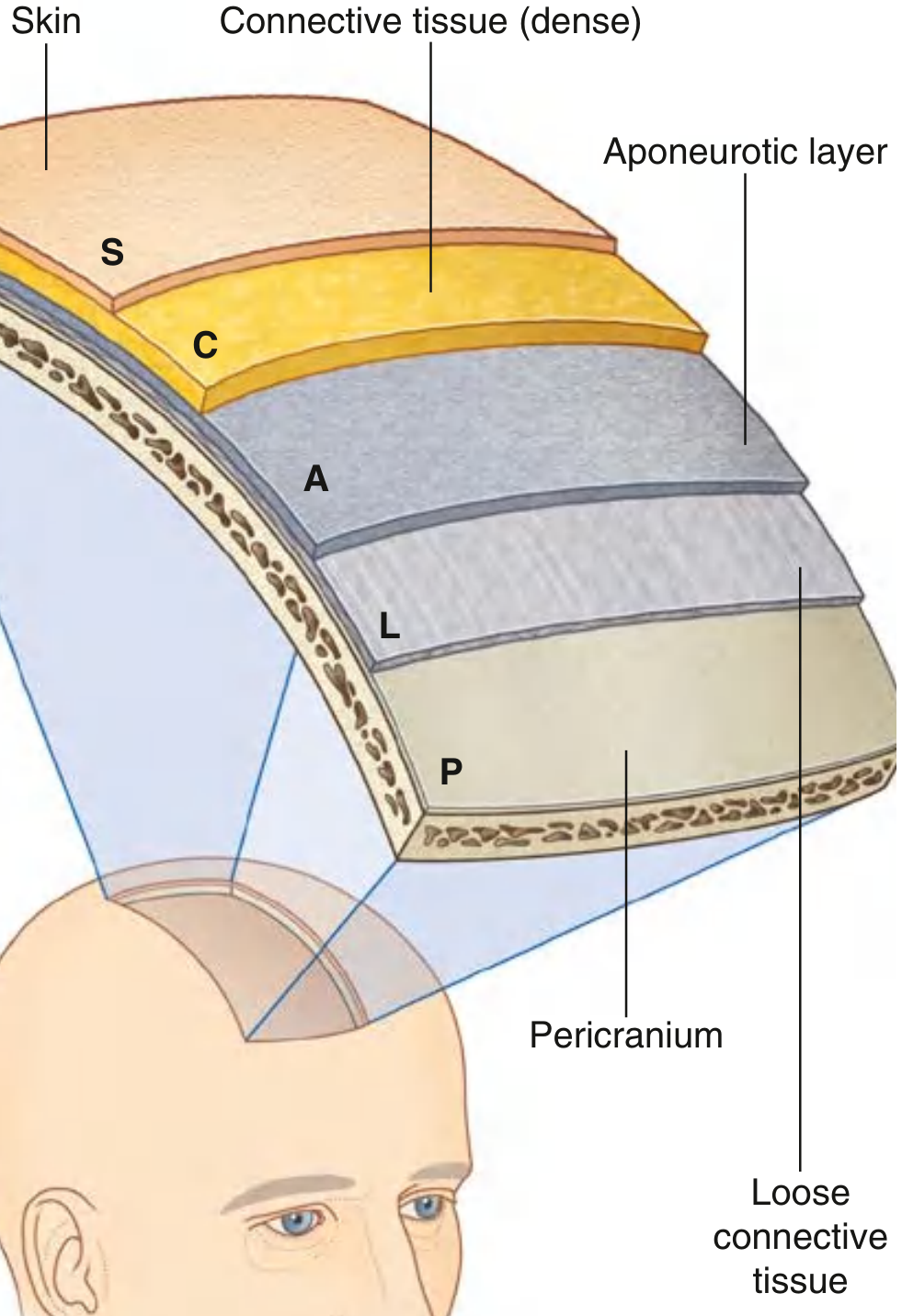
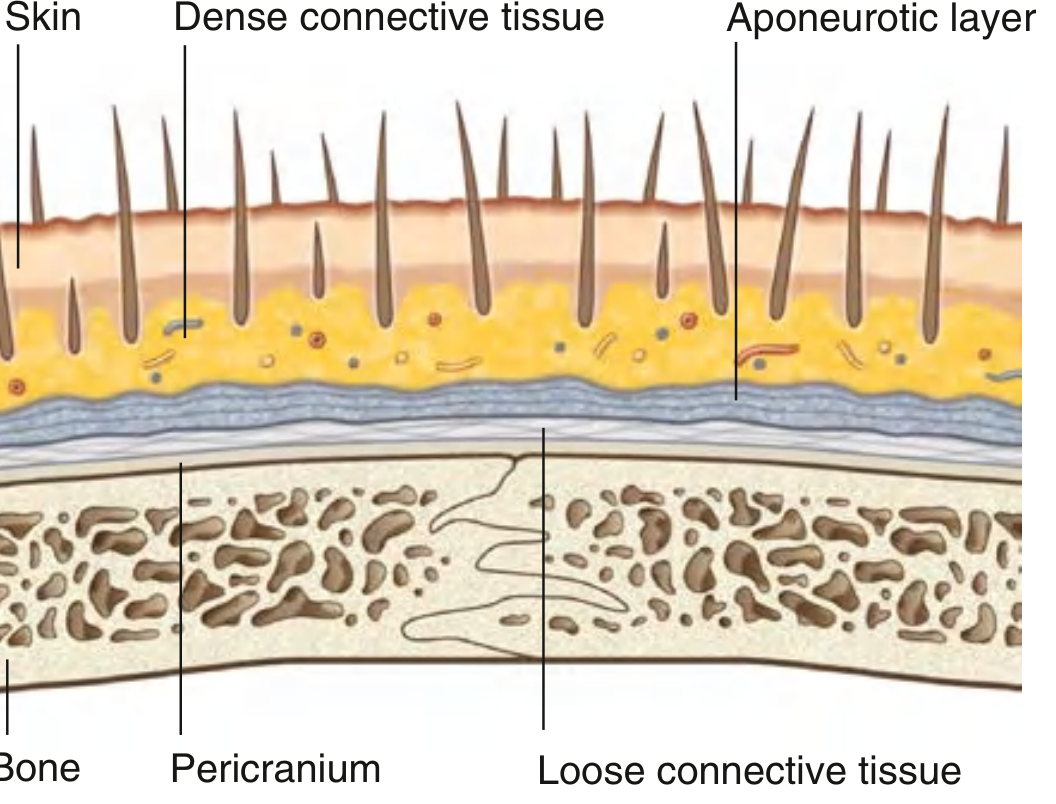
Layers — The "SCALP" Mnemonic
| Layer | Detail | Clinical note |
|---|---|---|
| S — Skin | Outer layer; contains hair follicles | Thickest skin in the body |
| C — Connective tissue (dense) | Contains arteries, veins, nerves | Dense fibrous septa hold vessels open → profuse bleeding when cut |
| A — Aponeurotic layer | Epicranial aponeurosis (galea aponeurotica); connects frontal & occipital bellies of occipitofrontalis | The first 3 layers move together as "scalp proper" — the unit avulsed in scalping injuries |
| L — Loose connective tissue | Allows free movement of scalp proper over calvaria | "Dangerous space" — infections track and spread widely here; emissary veins connect scalp to intracranial sinuses → risk of intracranial infection |
| P — Pericranium | Periosteum on outer surface of calvaria; firmly attached at sutures | Removable from bone but fixed at sutures |
The Occipitofrontalis Muscle (Aponeurotic Layer)
- Frontal belly: arises from skin of eyebrows → passes up forehead → galea aponeurotica
- Innervated by temporal branches of the facial nerve [VII]
- Action: wrinkles forehead, raises eyebrows
- Occipital belly: arises from superior nuchal line & mastoid process → galea aponeurotica
- Innervated by posterior auricular branch of CN VII
Innervation of the Scalp
Sensory supply depends on location relative to the ears and vertex:
Anterior to ears & vertex → Trigeminal nerve [CN V]:
| Nerve | Region supplied |
|---|---|
| Supratrochlear (V₁) | Medial forehead near midline |
| Supra-orbital (V₁) | Anterior scalp to vertex |
| Zygomaticotemporal (V₂) | Small anterior temple area |
| Auriculotemporal (V₃) | Temporal scalp, anterior to ear |
Posterior to ears & vertex → Cervical nerves (C2–C3):
| Nerve | Region supplied |
|---|---|
| Great auricular (C2–C3) | Small area just posterior to ear |
| Lesser occipital (C2) | Scalp posterior and superior to ear |
| Greater occipital (C2 dorsal ramus) | Large part of posterior scalp up to vertex |
| Third occipital (C3 dorsal ramus) | Lower posterior scalp |
Arterial Supply of the Scalp
Branches come from two sources:
From the ophthalmic artery (branch of internal carotid):
- Supratrochlear artery — anterior and superior scalp
- Supra-orbital artery — anterior scalp to vertex
From the external carotid artery:
- Superficial temporal artery (terminal branch) — lateral scalp
- Posterior auricular artery — scalp posterior to ear
- Occipital artery — large portion of posterior scalp
All five arteries on each side form rich anastomoses with their counterparts across the midline and with each other — this is why scalp bleeding is so profuse and why scalp flaps remain viable even after significant mobilization.
Venous Drainage
Veins mirror the arteries and drain into the external jugular, internal jugular, and (via emissary veins) into the dural venous sinuses intracranially. This direct intracranial communication means scalp infections carry a risk of cavernous sinus thrombosis or meningitis.
Key Clinical Correlates
| Condition | Anatomical basis |
|---|---|
| Profuse scalp bleeding | Dense connective tissue holds vessels open; cannot retract like skin elsewhere |
| Scalp infections → intracranial spread | Emissary veins in the loose (L) layer communicate with dural sinuses |
| Subgaleal haematoma | Blood collects in loose connective tissue layer; can spread widely across entire calvaria |
| Subaponeurotic abscess | Same loose layer allows diffuse infection spread |
| Scalp laceration repair | Must close the galea (A layer) to restore tension barrier and reduce bleeding |
— Gray's Anatomy for Students, pp. 979–992, 1062–1065
This is a shared conversation. Sign in to Orris to start your own chat.