Interstitial brachytherapy in detail according to standard books
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive content from multiple authoritative textbooks. Let me compile the detailed response.
Interstitial Brachytherapy - Detailed Overview
(Sourced from Campbell-Walsh-Wein Urology, Smith & Tanagho's General Urology, Berek & Novak's Gynecology, and Grainger & Allison's Diagnostic Radiology)
1. Definition and Basic Principle
Brachytherapy refers to a treatment technique that places radioactive sources in close proximity to or directly into the tumor (from the Greek brachy = short distance). Interstitial brachytherapy specifically involves the placement of radioactive needles, afterloaded needles or catheters, or radioactive seeds directly into the tissue - as opposed to intracavitary brachytherapy, which places sources inside a body lumen or orifice.
A fundamental physical advantage is that radiation dose falls off rapidly according to the inverse square law - irradiation affects only a highly localized area around the source, meaning very high doses can be delivered to the target while healthy tissue further away receives minimal exposure.
- Smith & Tanagho's General Urology, p. 436
- Grainger & Allison's Diagnostic Radiology, p. 1726
2. Classification
Brachytherapy is classified along two axes:
| Axis | Categories |
|---|---|
| By placement | Interstitial vs. Intracavitary |
| By dose rate | Permanent/LDR vs. Temporary/HDR (vs. PDR) |
By Placement
- Interstitial: Radioactive needles, afterloaded catheters, or seeds placed directly into tissue (prostate, bladder, penis, periurethral soft tissues, gynecologic tumors)
- Intracavitary: Placement of sources into a lumen or orifice (uterine canal, vagina, urethra)
- Combined intracavitary/interstitial: Newer applicators that incorporate interstitial needles into standard intracavitary tandem-and-ring geometry
By Dose Rate
-
Low-dose rate (LDR): Continuous radiation over weeks-months via permanent seeds; dose rate <0.4 Gy/hour (technically, isotopes like Cs-137 fall here in traditional use)
-
High-dose rate (HDR): Short but high-dose radiation using temporary catheters; >12 Gy/hour with Ir-192 remote afterloading
-
Pulsed-dose rate (PDR): Uses an Ir-192 HDR source with a pulsed regimen designed to mimic the radiobiologic effects of LDR treatment; mostly seen at specialized academic centers
-
Smith & Tanagho's General Urology, p. 436
-
Berek & Novak's Gynecology, p. 2253
3. Isotopes Used
For Permanent (LDR) Interstitial Implants
| Isotope | Energy | Half-life | 90% dose delivered in | Monotherapy dose |
|---|---|---|---|---|
| ¹²⁵Iodine | 27 keV x-rays | 59.6 days | 204 days | 140-160 Gy |
| ¹⁰³Palladium | 21 keV x-rays | 17 days | 58 days | 110-125 Gy |
| ¹³¹Cesium (since 2004) | 30 keV x-rays | 9.7 days | 33 days | 100-115 Gy |
- ¹²⁵I is considered more "forgiving" dosimetrically due to slightly higher energy offering better prostatic coverage
- A randomized trial comparing ¹²⁵I vs. ¹⁰³Pd in low-risk disease found no difference in biochemical control; urinary symptoms were worse at 1 month with ¹⁰³Pd but resolved more rapidly
For Temporary (HDR) Interstitial Implants
-
Iridium-192 (¹⁹²Ir): 400 keV gamma radiation; used via remote afterloading systems; single source migrated along catheter length at variable positions and dwell times
-
Campbell-Walsh-Wein Urology, p. 4700-4701
4. Technique: LDR Permanent Seed Implant (Prostate Prototype)
Pre-procedure Planning
- Volume study using transrectal ultrasound (TRUS)
- Preoperative dosimetric planning determines number of seeds, seed activity, and needle/seed positions
- Seeds are peripherally loaded to minimize dose to the central urethra
Procedure
- Patient under spinal or general anesthesia
- TRUS probe placed transrectally for real-time imaging
- A perineal template grid is used to guide transperineal needle insertion
- Seeds are deposited at calculated positions as needles are withdrawn
- Typically 60-120 seeds placed using 15-25 needles
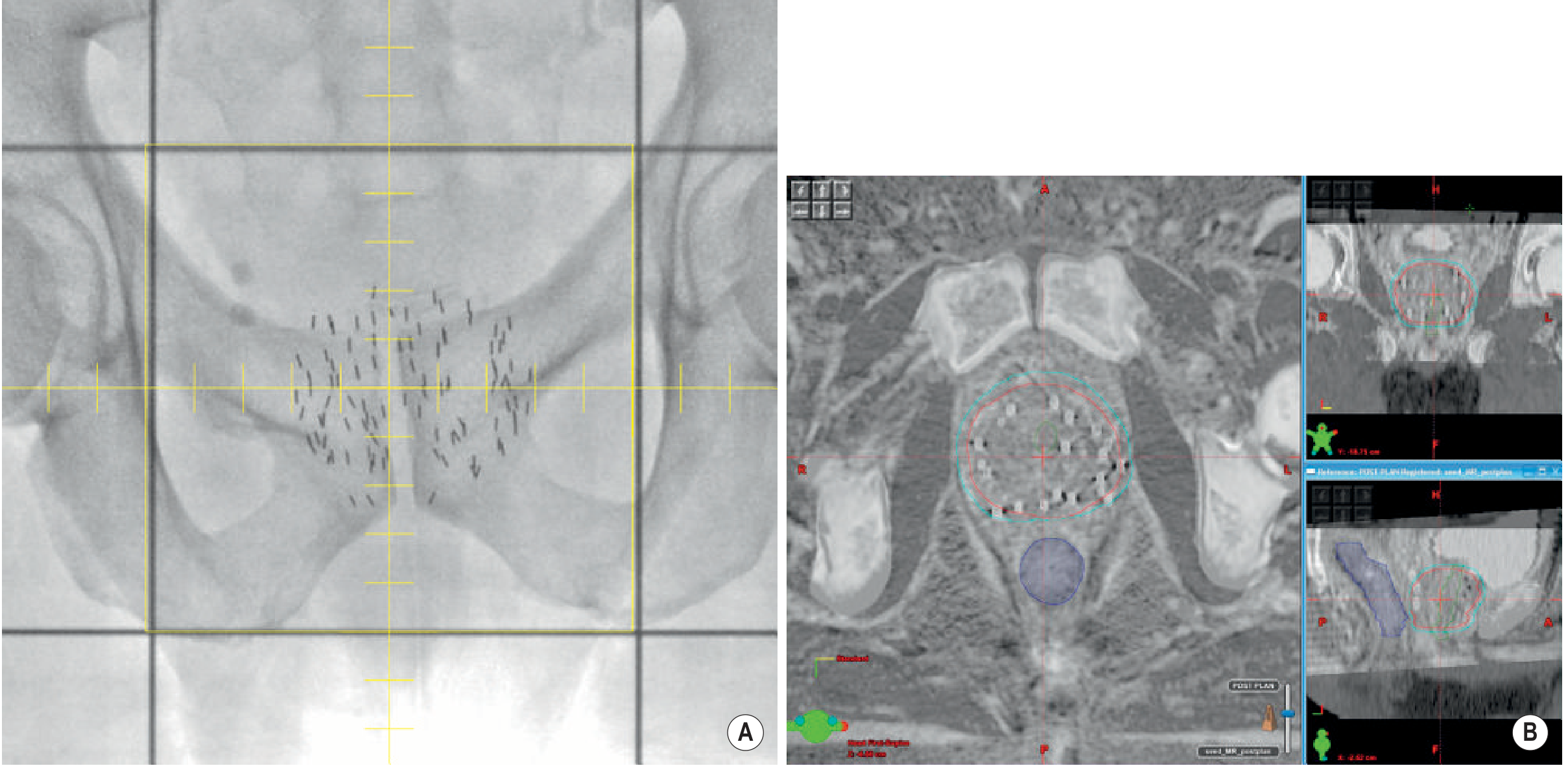
LDR brachytherapy for prostate cancer - plain radiograph and fused CT/MRI post-implant (Grainger & Allison)
Post-implant Dosimetry
-
CT with or without MRI fusion performed 4-6 weeks post-implant (not immediately) because seed migration occurs due to bleeding and swelling from the trauma of implantation
-
Key dosimetric parameters: D90 (dose covering 90% of prostate) and V100 (% of prostate volume receiving 100% prescribed dose)
-
MRI offers superior prostate delineation; CT better identifies metallic seed positions - fused images combine both advantages
-
Campbell-Walsh-Wein Urology, p. 4701-4702
-
Grainger & Allison's Diagnostic Radiology, p. 1729
5. Technique: HDR Interstitial Brachytherapy
Mechanism
- Hollow catheters are placed transperineally into the prostate (or through templates into other tissue targets) using the same grid-and-TRUS technique as LDR
- A single ¹⁹²Ir source is robotically driven ("afterloaded") along the length of each catheter
- The source dwells for seconds to minutes at 5 mm intervals - dwell times are modulated to optimize dose distribution
- All radioactive material is removed at the end of treatment - no sources remain in the patient
- Treatment is delivered in a shielded room via remote activation
Fractionation (Prostate HDR as Boost)
Common EBRT schedules combined with HDR boost include:
- 45 Gy in 25 fractions (5 weeks) + HDR
- 46 Gy in 23 fractions (4.5 weeks) + HDR
- 35.7 Gy in 13 fractions (2.5 weeks) + HDR
HDR monotherapy (without EBRT) is increasingly used for low-to-intermediate risk prostate cancer.
- Campbell-Walsh-Wein Urology, p. 4702-4703
6. Advantages and Disadvantages: HDR vs. LDR
Advantages of HDR over LDR
| Advantage | Explanation |
|---|---|
| Greater target flexibility | Catheter-based placement allows easier inclusion of extracapsular disease and seminal vesicles |
| Dose optimization | Modifying dwell times and positions allows real-time dose sculpting |
| Biological dose advantage | High dose per fraction exploits low alpha/beta ratio of prostate cancer |
| Radiation safety | No personnel handling of radioactive source; no sources left in patient |
| Cost-effectiveness | Single multipurpose ¹⁹²Ir source used for all patients |
| No post-implant dosimetry needed | Sources removed after treatment |
Disadvantages of HDR over LDR
| Disadvantage | Explanation |
|---|---|
| Treatment inaccuracies | Catheter/organ movement between imaging and source insertion; interobserver contouring variability |
| Patient convenience | Multiple fractions require repeated catheter placements or maintained catheter access |
| Shielded room required | High activity ¹⁹²Ir source requires dedicated infrastructure |
| Less pathologic response | Available post-treatment biopsy studies favor LDR |
| Limited phase III data | No comparable randomized data for HDR in high-risk prostate cancer |
- Campbell-Walsh-Wein Urology, p. 4703
7. Gynecologic Applications (Cervix Cancer)
Combined Intracavitary/Interstitial Brachytherapy
- Newer applicators incorporate interstitial needles into the standard tandem-and-ring or tandem-and-ovoids geometry (e.g., the Vienna applicator)
- Interstitial needles extend reach beyond what standard intracavitary geometry can dose
- Especially useful for bulky or irregularly shaped tumors that extend beyond the standard applicator coverage
- In the retroEMBRACE study: combined intracavitary/interstitial BT vs. intracavitary alone showed a 10% improvement in local control for larger tumors (cervix + tumor volume >30 cm³)
- Can often eliminate the need for more morbid techniques such as the Syed template or MUPIT template needle implants
2D vs. 3D Image-Guided Brachytherapy (IGA-BT)
- Classical 2D: Dose prescribed to "Point A" (2 cm superior to the cervical os, 2 cm lateral to the intrauterine canal); typical dose 7,000-8,000 cGy to Point A, limiting bladder/rectum to <6,000 cGy
- Modern 3D IGA-BT: MRI/CT-based volumetric planning; dose prescribed to the high-risk CTV D90 (8,500-9,500 cGy cumulative)
- The French STIC multicenter trial (705 patients) prospectively demonstrated 3D brachytherapy gave improved local control with half the toxicity of 2D brachytherapy
- Dose constraints (GEC-ESTRO): bladder D2cc <90 Gy EQD2; rectum D2cc <75 Gy EQD2; sigmoid D2cc <75 Gy EQD2
LDR vs. HDR for Cervix Cancer
-
LDR (Cs-137): Manual placement, requires inpatient admission 1-3 days, patient immobilization, DVT prophylaxis, radiation precautions for staff
-
HDR (Ir-192): Ambulatory, shorter total treatment time, remote afterloading eliminates staff exposure
-
A Cochrane review found no significant differences in OS, disease-specific survival, local control, or complications between LDR and HDR for locally advanced cervix cancer (based on 4 qualifying trials)
-
Berek & Novak's Gynecology, pp. 2253-2255
8. Other Interstitial Brachytherapy Applications
| Site | Details |
|---|---|
| Prostate cancer | LDR seed implant (low-risk) or HDR boost/monotherapy (intermediate/high-risk) |
| Penile/urethral cancer | Both EBRT and interstitial BT may be used; circumcision required prior to BT to expose the lesion and prevent inflammation-related swelling |
| Head and neck cancers | Interstitial implants for base of tongue, lip, floor of mouth; IMRT with or without BT boost |
| Breast cancer | Interstitial multi-catheter implant as partial breast irradiation (APBI) |
| Endobronchial tumors | Catheter-based bronchoscopic placement for airway tumors |
| Bladder cancer | Interstitial BT for selected Ta/T1 and T2 tumors; not yet standard of care |
| Gynecologic (vaginal/cervical) | Combined intracavitary/interstitial for bulky disease |
| Liver metastases | Interstitial BT as one of multiple local ablative options |
9. Dosimetry Principles
-
Dose from each source position is additive; superposition of contributions from all dwell positions defines the overall dose distribution
-
Inverse square law governs rapid dose fall-off away from each source
-
Imaging is mandatory: CT identifies applicator/seed positions precisely; MRI provides superior soft tissue definition (especially prostate and cervix)
-
For LDR prostate: post-implant CT/MRI fusion at 4-6 weeks - D90 and V100 are key quality indicators
-
For HDR: real-time or near-real-time planning at each fraction based on CT/MRI with applicators in situ
-
Grainger & Allison's Diagnostic Radiology, pp. 1726-1729
10. Comparison With External Beam Radiotherapy
| Feature | Interstitial BT | EBRT |
|---|---|---|
| Dose fall-off | Rapid (inverse square law) - spares adjacent normal tissue | Gradual; requires margins around target |
| Patient setup variation | Minimal - sources move with tumor | Significant daily repositioning needed |
| Tumor motion | Not a concern - sources within tumor | Major challenge (breathing, organ filling) |
| Dose per fraction | Can exploit high doses per fraction biologically | Typically 1.8-2 Gy fractions |
| Access | Invasive procedure required | Non-invasive |
| Suitable volumes | Small to medium tumors; precise geometry | Any volume; irregular shapes |
Sources:
- Campbell-Walsh-Wein Urology, 3-Volume Set - Chapters 157 & 158 (LDR/HDR Prostate Brachytherapy)
- Smith & Tanagho's General Urology, 19th Ed. - Chapter 26 (Brachytherapy classification and technique)
- Berek & Novak's Gynecology - Chapter on Primary Radiation Therapy (Cervix cancer brachytherapy)
- Grainger & Allison's Diagnostic Radiology - Chapter 67 (Principles of radiotherapy including brachytherapy)
Application in ent and head and neck surgery only
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
I now have comprehensive content from multiple ENT/H&N textbooks. Let me compile the full detailed answer.
Interstitial Brachytherapy in ENT and Head & Neck Surgery
(Sourced from Cummings Otolaryngology, Scott-Brown's Otorhinolaryngology Head & Neck Surgery, KJ Lee's Essential Otolaryngology, and Grainger & Allison's Diagnostic Radiology)
1. Historical Background and Basic Principles in H&N
Brachytherapy in head and neck cancer has deep roots - the first documented successful treatment was reported in 1899, when Thor Stenberg treated a nasal basal cell carcinoma with radium over 9 months, with the patient alive 30 years later. In 1901, Dr. Frand Williams in Boston reported successful treatment of a lip cancer. Radium was initially applied only to superficial sites because of severe toxicities; physicians later began inserting it directly into deep-seated tumors, founding the field of brachytherapy.
Core principle: Radiation dose from an implanted source obeys the inverse square law - it falls off rapidly with distance, allowing very high doses to be concentrated at the target (tumor) while sparing surrounding healthy tissues (including bone, nerve, major vessels).
Key advantage in H&N: Better dose localization → less radiation damage to surrounding healthy tissue, and prolonged time over which radiation is delivered.
Key disadvantage in H&N: Does not address subclinical nodal disease; requires general anesthesia in many cases; close proximity of mandible creates risk of osteoradionecrosis.
- Cummings Otolaryngology, p. 1343, 1361
2. Radioactive Sources Used in H&N Brachytherapy
| Source | Type | Notes |
|---|---|---|
| Iridium-192 (¹⁹²Ir) | LDR afterloading or HDR | Most widely used; dose rate 0.4-0.8 Gy/hour (LDR); or >12 Gy/hour (HDR remote afterloading) |
| Cesium-137 (¹³⁷Cs) | LDR needles | Traditional use; being replaced by ¹⁹²Ir |
| Radium-226 (²²⁶Ra) | Historical | Needles for implants; now largely obsolete |
| Gold-198 (¹⁹⁸Au) | Permanent grains | Used for nasopharyngeal recurrences (grain implantation) |
| Iodine-125 (¹²⁵I) | Permanent seeds | Low energy; used in selected cases |
A typical ¹⁹²Ir LDR implant delivers approximately 0.4-0.8 Gy/hour. HDR remote afterloading devices drive a single high-activity ¹⁹²Ir source through a set of interstitial catheters under computer control; typically 3.0-3.5 Gy is delivered to ~1 cm from the catheter periphery per treatment, with up to two daily treatments ~6 hours apart, each lasting 15-30 minutes depending on source strength and implant complexity.
- Cummings Otolaryngology, p. 1361
3. Site-by-Site Applications
A. Oral Tongue (Mobile Tongue)
Radiotherapy (brachytherapy preferred over EBRT) has been advocated as a primary treatment modality because it conserves tongue volume and morphology - an enormous functional advantage.
Indications:
- T1-T2 tumors of mobile tongue not suitable for surgery, or where organ preservation is prioritized
- Brachytherapy alone or as a boost after EBRT
Technique: ¹⁹²Ir interstitial implant through the tongue tissue, using afterloading catheters placed to encompass the tumor with adequate margins.
Outcomes: Brachytherapy is considered preferable to EBRT for tongue primaries in terms of dose localization and functional preservation.
Key limitation - Osteoradionecrosis (ORN): The mandible lies in close proximity to the tongue. Up to 9% of patients develop some form of osseous complication following tongue brachytherapy. This is a recognized and major concern that has led some centers to prefer surgery as primary treatment, keeping radiotherapy in reserve for:
- Poor pathologic prognostic indicators post-resection
- Recurrence
- Second primaries
An important additional consideration is that when surgery is not used as the primary modality, valuable histopathological prognostic information is lost - making decisions about elective neck dissection (END) more difficult.
Some authorities suggest surgery is superior to brachytherapy for Stage I/II tongue cancer for this reason (retaining radiotherapy as a reserve modality).
- Scott-Brown's Otorhinolaryngology, p. 6861
B. Floor of Mouth
Indications:
- T1/T2 floor-of-mouth carcinomas - brachytherapy (or EBRT) has been shown to give results comparable to surgery
Key limitation - ORN risk is particularly high here:
-
The floor of mouth lies in direct proximity to the mandible
-
Up to 8.5% of patients treated with brachytherapy for floor-of-mouth cancer require segmental mandibulectomy for osteoradionecrosis within 10 years (Gustave-Roussy Institute series; Pernot et al., Marsiglia et al.)
-
Several major units have changed practice from brachytherapy to surgery as the primary treatment modality for floor-of-mouth cancer, specifically because of this complication risk
-
T3/T4 lesions are best treated with surgery + post-operative radiotherapy (PORT)
-
Scott-Brown's Otorhinolaryngology, p. 6641-6652
C. Base of Tongue (Oropharynx)
Role of brachytherapy: RT for base of tongue is often performed as a combination of EBRT + interstitial ¹⁹²Ir implant.
Outcomes data (Cummings Otolaryngology):
| Treatment | T1 Local Control | T2 Local Control |
|---|---|---|
| EBRT alone (primary) | 78-96% | 47-88% |
| EBRT + brachytherapy implant | 71-100% | 71-100% |
| EBRT alone vs. combined | EBRT alone = unacceptably high failure rate (2× other groups) |
Houssef et al. compared surgery + adjuvant RT vs. EBRT + ¹⁹²Ir implant vs. EBRT alone for T1/T2 base-of-tongue cancers and found:
- Surgery + adjuvant RT ≈ EBRT + implant (comparable results)
- EBRT alone showed unacceptable failure rate - twice as high as the other two groups
For salvage/recurrent disease, afterloading techniques with ¹⁹²Ir have achieved local control of 59% and actuarial survival of 48%, though residual/recurrent tongue base disease remains a demanding problem.
- Cummings Otolaryngology, p. 1793
D. Tonsillar Region / Oropharynx
Salvage surgery after primary RT in the tonsillar region carries high mortality and low 5-year survival (Gehanno et al.: 5-year survival 24%, mortality as high as 8% in 120 patients).
Two investigations support brachytherapy salvage in the tonsillar region:
-
5-year survival rate: 64% (one series)
-
2-year survival rate: 42% (another series)
-
Cummings Otolaryngology, p. 1792
E. Nasopharynx (Recurrent/Salvage Setting)
Brachytherapy for nasopharyngeal carcinoma (NPC) is used specifically in the salvage setting for local failure following primary chemoradiation, as an alternative to re-irradiation with EBRT (which has poor outcomes due to proximity of brainstem, optic chiasm, and temporal lobe to the treatment field).
Rationale: Traditional 2D re-irradiation for NPC local failure has a 5-year survival of only 7.6% due to dose constraints protecting vital organs. Brachytherapy delivers a high dose with limited penetration - ideal for small recurrences without deep invasion.
Radioactive sources:
- Iridium-192 (¹⁹²Ir): The source is loaded into a tailor-made plastic mould fitted into the nasopharynx. The mould is placed transorally (via the oral cavity) under local anaesthesia.
- Gold-198 (¹⁹⁸Au) grains: Implanted directly into the nasopharynx after the soft palate is split open under general anaesthesia.
Patient selection: Both techniques are only suitable for small tumors <2 cm in maximal dimension (no deep invasion).
Outcomes:
- 5-year survival: 50-60% for salvage brachytherapy of NPC local recurrence
As an alternative to brachytherapy, stereotactic RT (3D/IMRT-based) for NPC local salvage has shown 5-year overall survival 40% and local control 57% (series of 30 patients) - brachytherapy outcomes are superior but patient selection is stricter (smaller tumors only).
Brachytherapy also has a potential role in nodal failure in NPC, used in conjunction with surgical resection of nodal metastasis (the limited penetration of brachytherapy makes it suitable as an adjunct after debulking surgery).
- Scott-Brown's Otorhinolaryngology, p. 8504-8520
F. Orbit and Paranasal Sinuses (Intracavitary, H&N)
The orbit and nasopharynx are the most common intracavitary head and neck brachytherapy sites. Custom PMMA (acrylic) stents are constructed around catheters into which radioisotopic seeds are inserted:
-
The radiation oncologist/physicist prescribes catheter positions in consultation with the maxillofacial prosthodontic team, after generating a master cast from an impression of the site
-
Stents are retained in position by anatomic soft tissue undercuts or alveolar structures
-
After maxillectomy, intracavitary void-filling with tissue-equivalent material improves dose distribution (preventing uneven dosing of peripheral tissues around the surgical defect)
-
Cummings Otolaryngology, p. 1702
G. Lip Cancer
One of the original sites treated with brachytherapy historically (1901 - Dr. Williams, Boston). Lip carcinoma remains amenable to interstitial brachytherapy, particularly for:
-
Small T1-T2 squamous cell carcinomas of the lip
-
As an organ-preserving alternative to surgery for cosmetically sensitive sites
-
Cummings Otolaryngology, p. 1343
4. Technique Summary for H&N Interstitial BT
LDR ¹⁹²Ir Interstitial Implant (Standard Technique)
- Planning phase: CT/MRI-based volumetric planning; catheter positions determined to achieve adequate dose to tumor with acceptable dose to adjacent mandible, vessels, nerves
- Implant procedure: Under general anaesthesia (most cases); hollow plastic catheters or metal needles inserted through the tumor-bearing tissue
- Afterloading: ¹⁹²Ir sources loaded into catheters; patient cared for in a shielded room during treatment
- Dose delivery: 0.4-0.8 Gy/hour continuously over 2-6 days
- Source removal: All sources and catheters removed at end of treatment
HDR Remote Afterloading (Modern Approach)
- Computer-controlled robotic ¹⁹²Ir source driven through catheters
- Dwells at 5 mm intervals; dwell times modulated to optimize dose distribution
- Each fraction: 3.0-3.5 Gy to ~1 cm from catheter periphery
- Up to 2 fractions per day (at least 6 hours apart)
- Each treatment: 15-30 minutes
- Advantages: Eliminates radiation exposure to nursing/medical staff; outpatient delivery possible
5. Combinations with EBRT
In head and neck cancer, interstitial brachytherapy is frequently used as a boost following a course of EBRT:
- EBRT addresses the primary tumor plus regional lymphatics (elective or therapeutic nodal irradiation)
- Brachytherapy delivers an additional dose increment to the primary tumor bed, achieving higher total doses than either modality alone
- This combination is the standard approach for base-of-tongue carcinoma and is used in other oral cavity sites
6. Complications Specific to H&N Brachytherapy
| Complication | Details |
|---|---|
| Osteoradionecrosis (ORN) of mandible | Most feared; up to 9% for tongue BT, up to 8.5% requiring segmental mandibulectomy for floor-of-mouth BT; high local doses from BT increase incidence; risk further raised by microvascular disease (atherosclerosis, diabetes) and post-RT dental extractions |
| Soft tissue necrosis | Histologically: epithelial hyperplasia → dermal fibrosis → necrosis; Marx characterized tissue as "hypoxic, hypocellular, hypovascular" |
| Mucositis | Acute; self-limiting; universal to varying degree with all H&N RT |
| Xerostomia | From inclusion of salivary glands in the radiation field |
| Trismus | Radiation fibrosis of masticator muscles |
| Radiation-related fistulae | In high-dose zones near mucosa |
| Radioprotection requirements | LDR implants require patient isolation in shielded room; HDR remote afterloading eliminates this (no radiation exposure to staff during treatment) |
ORN pathophysiology (Scott-Brown's Vol. 2):
- Impaired tissue repair capacity
- Vasculitis → obliteration of blood vessels → avascular necrosis
- Marx triad: hypoxic + hypocellular + hypovascular tissue
- Macroscopically: loss of skin/soft tissue exposing bone, bony sequestration, secondary infection
Note on temporal bone: The compact (non-cancellous) nature of the petrous temporal bone and poor blood supply of the tympanic ring make this region particularly susceptible to ORN from brachytherapy of adjacent tumors.
- Scott-Brown's Vol. 2, p. 1011
- Cummings Otolaryngology (Key Points, p. 1702)
7. Contraindications and Patient Selection
| Factor | Implication |
|---|---|
| Tumor > 2 cm in nasopharynx | Contraindication to NPC salvage BT |
| Deep invasion of tumor | Contraindication to BT (limited penetration cannot cover deep extension) |
| Prior high-dose RT to site | Increased ORN risk; careful re-treatment planning needed |
| Poor dental hygiene | Must optimize dental care pre-BT to reduce ORN risk |
| Diabetes / atherosclerosis | Increased ORN risk; relative contraindication to BT near mandible |
| Need for nodal treatment | BT alone insufficient; must add EBRT or neck dissection |
8. Summary Table: BT Applications by H&N Site
| Site | Role | Source/Technique | Key Outcome Data | Main Risk |
|---|---|---|---|---|
| Oral tongue (T1-T2) | Primary or EBRT boost; organ preservation | ¹⁹²Ir LDR/HDR interstitial | Comparable to surgery for T1/T2 | ORN 9% |
| Floor of mouth (T1-T2) | Primary (results = surgery); T3/T4 → surgery + PORT | ¹⁹²Ir LDR interstitial | ~= surgery; many units switching to surgery | ORN up to 8.5% → mandibulectomy |
| Base of tongue | EBRT + BT boost (standard); salvage afterloading | ¹⁹²Ir LDR/HDR interstitial | T1: 71-100%; T2: 71-100% (EBRT + BT) | Functional swallowing |
| Tonsillar region | Salvage after RT failure | ¹⁹²Ir afterloading | 5-yr survival 64%; 2-yr survival 42% | High operative mortality if surgical salvage used |
| Nasopharynx (recurrent) | Salvage for small (<2 cm) recurrences | ¹⁹²Ir mould or ¹⁹⁸Au grains | 5-yr survival 50-60% | Limited to tumors without deep invasion |
| Orbit/sinus (intracavitary) | Post-maxillectomy/targeted | PMMA stent with ¹²⁵I seeds | Site-specific | Dosimetric consistency |
| Lip (T1-T2) | Primary; cosmetic preservation | Interstitial needles | Historically effective (first H&N site treated, 1901) | ORN (low risk, away from mandible) |
Sources:
- Cummings Otolaryngology Head and Neck Surgery - Chapter 75 (Radiation Therapy Principles) & Chapter 96 (Oropharyngeal Cancers)
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery - Oral tongue, floor of mouth, and nasopharynx chapters
- Scott-Brown's Vol. 2 - Osteoradionecrosis chapter
- KJ Lee's Essential Otolaryngology - Oral tongue cancer chapter
- Grainger & Allison's Diagnostic Radiology - Brachytherapy principles chapter
This is a shared conversation. Sign in to Orris to start your own chat.