Traumatic Cardiac Arrest
Reading File
Finding Sources
Finding Sources
Searching PubMed
"traumatic cardiac arrest" management resuscitation
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Here is a comprehensive review of Traumatic Cardiac Arrest (TCA):
Traumatic Cardiac Arrest
Definition and Epidemiology
Traumatic cardiac arrest (TCA) is cardiac arrest occurring as a direct result of physical injury. It is fundamentally different from medical cardiac arrest in mechanism, management priorities, and approach to resuscitation. TCA carries a historically poor prognosis - overall survival rates are low, but outcomes are highly variable based on mechanism, injury location, and time to intervention. Penetrating trauma has substantially better outcomes than blunt trauma when managed aggressively.
Penetrating cardiac injuries are among the leading causes of death in urban violence settings. Improvements in EMS and emphasis on rapid transport have increased the number of cardiac injury patients arriving in extremis or full arrest at trauma centers.
Etiology and Pathophysiology
TCA results from several distinct, often co-existing, mechanisms. Identifying and reversing these is the core of TCA management:
| Cause | Mechanism |
|---|---|
| Exsanguination / Hemorrhage | Most common cause overall; massive blood loss depletes preload |
| Cardiac tamponade | Blood accumulation in pericardial sac compresses the heart; even 65-100 mL can cause acute rise in intrapericardial pressure |
| Tension pneumothorax | Mediastinal shift compresses the heart and great vessels; complete hemodynamic collapse if untreated |
| Massive hemothorax | Compressive physiology + hypovolemia |
| Direct myocardial injury | Contusion, rupture, or laceration from blunt or penetrating trauma |
| Hypoxia | Airway or pulmonary injury causing severe hypoxemia |
| Open pneumothorax | Disrupted chest wall mechanics prevent ventilation |
Cardiac Tamponade in Detail
Intrapericardial blood accumulation progressively increases intrapericardial pressure, decreasing right and left ventricular filling. Catecholamine release causes compensatory tachycardia and elevated right-sided filling pressures. Once the pericardium's distensibility limit is reached, the septum shifts toward the left ventricle, further reducing cardiac output. This downward spiral produces irreversible shock and death.
Key points:
- Beck's Triad (muffled heart sounds, hypotension, JVD) is present in fewer than 10% of cases - do not rely on it.
- Sinus tachycardia may be the only finding initially.
- Narrowing of pulse pressure with elevated CVP is tamponade until proven otherwise.
- Gunshot wounds are less likely than stab wounds to cause tamponade because the pericardial defect is larger and harder to seal.
- Up to 80% of myocardial stab wounds may develop tamponade.
The "Cardiac Box" - Anatomic Risk Zone
Penetrating injuries within the "cardiac box" carry the highest risk for cardiac injury:
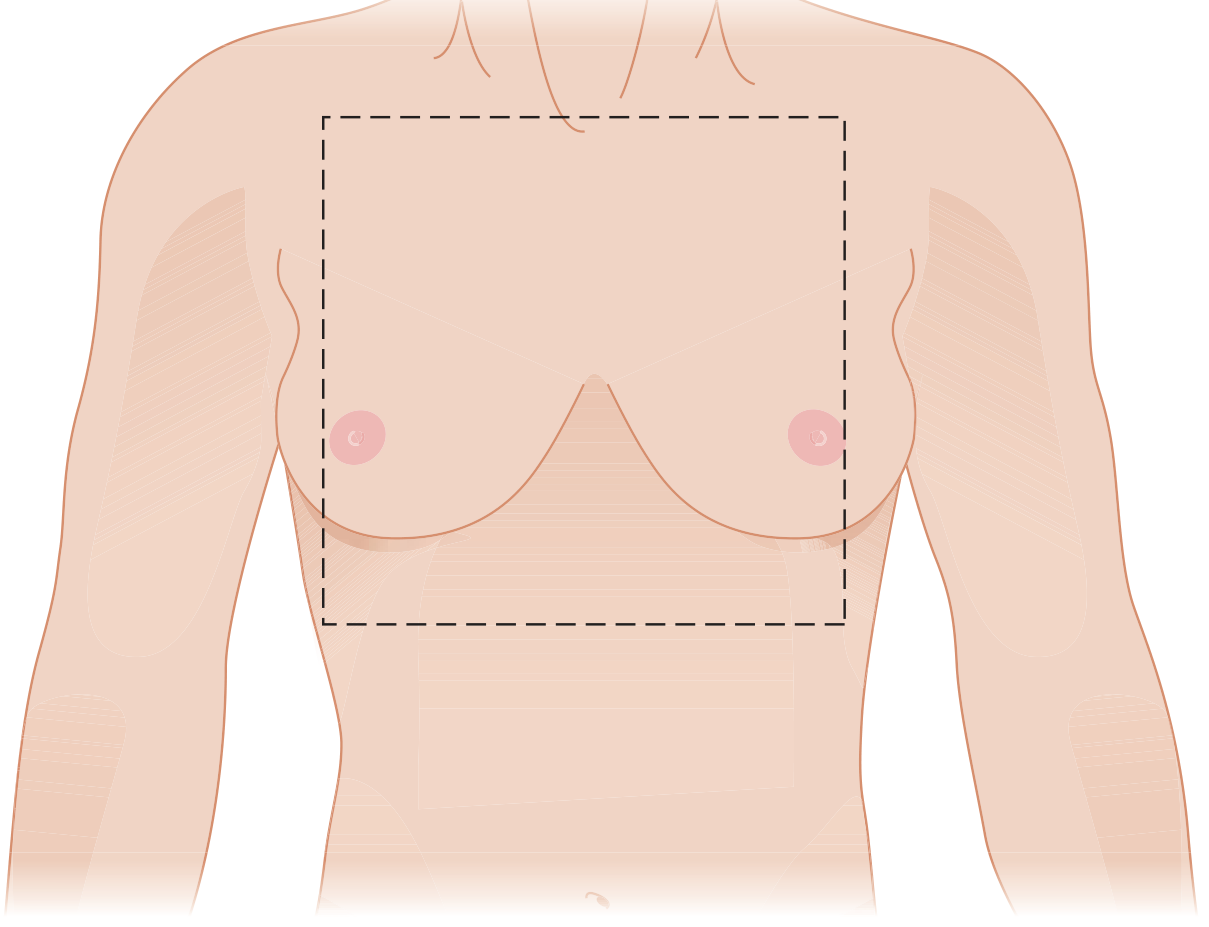
The cardiac box: sternal notch (superior), xiphoid (inferior), nipples (lateral). The right ventricle is most commonly injured due to its large anterior exposure.
Note: Gunshot wounds may enter far outside this region (transmediastinal, back, thoracoabdominal), so any such trajectory puts the heart at risk.
Blunt vs. Penetrating TCA
| Feature | Penetrating TCA | Blunt TCA |
|---|---|---|
| Common injuries | Stab wounds, GSW to cardiac box | MVA, falls, crush; right heart injury predominates |
| Tamponade | Very common (up to 80% of stab wounds) | Rare, but occurs |
| Mechanism | Direct cardiac injury or exsanguination | Myocardial contusion, rupture, aortic disruption |
| Survival with EDT | Up to ~35% (stab, cardiac box, witnessed) | ~1.4% overall; 0.7-2.4% neurologically intact |
| EDT indication | Strong - if witnessed, signs of life, penetrating chest | Narrow - only if loss of vital signs in the trauma bay |
In blunt trauma, over 90% of patients with aortic injury die at the scene. Of those who survive, 50% die within 24 hours and 90% within 4 months if untreated. Mortality for untreated aortic injury is approximately 1% per hour for the initial 48 hours.
Prehospital Considerations
The standard BLS algorithm is modified in trauma: C-A-B-C-D, where the first "C" is critical hemorrhage control (rather than leading with airway), then airway, breathing, circulation, defibrillation/disability.
CPR in TCA: Standard CPR is unlikely to benefit and may actually detract from more useful lifesaving interventions in primary TCA (e.g., hemorrhage control, decompression). The decision to withhold CPR should be made only by ALS-level or higher personnel.
Prehospital management priorities:
- Rapid transport to a trauma center (the primary intervention for abdominal trauma)
- Tourniquet and external hemorrhage control
- Needle decompression for suspected tension pneumothorax
- Advanced prehospital systems with physician-paramedic crews may perform prehospital thoracostomy, blood transfusion, or even resuscitative thoracotomy
Emergency Department Management
Initial Approach - Search for Reversible Causes (FAST + Primary Survey)
Upon arrival of a TCA patient, a critical decision must be made regarding escalation vs. termination of resuscitation. Any decision should be based on an immediate search for readily reversible causes. Point-of-care ultrasound (POCUS/FAST) is the primary tool and can identify:
- Cardiac tamponade (pericardial fluid)
- Pneumothorax
- Massive hemoperitoneum
- Presence or absence of ongoing cardiac activity
Immediately Reversible Causes to Address Simultaneously:
- Tension pneumothorax - immediate bilateral tube thoracostomy (do not await CXR); needle thoracostomy if tubes unavailable
- Cardiac tamponade - pericardiocentesis as bridge to thoracotomy, or emergency thoracotomy/pericardiotomy
- Massive hemorrhage - control external bleeding; operative intervention for internal sources
- Airway/hypoxia - definitive airway management
Emergency Department (Resuscitative) Thoracotomy
What It Achieves
- Release of cardiac tamponade and pericardiotomy
- Direct cardiac repair (finger, Foley balloon tamponade, suture)
- Open cardiac massage (internal)
- Control of thoracic hemorrhage
- Thoracic aortic cross-clamping to redirect blood to brain and coronaries, and control intra-abdominal hemorrhage
- Internal defibrillation
Technique
Left anterolateral thoracotomy through the 4th or 5th intercostal space with the patient supine. Can be extended across the sternum (clamshell incision) for access to the mediastinum and right chest.
For cardiac rupture control:
- Atrial hemorrhage: finger occlusion or vascular clamp; Foley catheter balloon through the defect
- Ventricular rupture: direct digital pressure or non-absorbable vascular sutures
- Cardiopulmonary bypass is only required in ~10% of successful myocardial rupture repairs
Indications and Contraindications
Strong indications (best outcomes):
- Penetrating chest trauma (especially stab wound to cardiac box) with witnessed loss of vital signs in the ED or within 15 minutes of arrival, with residual cardiac electrical activity
- Cardiac tamponade on bedside US with witnessed arrest: survival approaches ~35%
Relative indications (provider discretion, survival up to ~15%):
- Penetrating abdominal, pelvic, or extremity arrest with witnessed loss of vital signs in the field (with signs of life) or in-ED arrest
- Blunt thoracoabdominal trauma with arrest in the trauma bay
Contraindications / Not indicated:
- Blunt trauma with no pulse/respiration in the field (no survivors in key studies; EDT not recommended even with myocardial electrical activity)
- Unwitnessed loss of vital signs in the prehospital setting following blunt trauma
- Prolonged pulselessness (>15 minutes for penetrating; >10 minutes for blunt)
- Massive non-survivable injuries
- Absence of cardiac activity on bedside US
Survival Data Summary
| Scenario | Survival |
|---|---|
| Penetrating thoracic trauma (any) | Up to 24% |
| Stab wound to chest, breathing/pulse in field | ~23% |
| Stab wound to chest, moribund but signs of life on arrival | ~38% |
| Penetrating trauma, arrives pulseless (<15 min arrest) | ~4% |
| Blunt trauma (overall) | ~1.4% |
| Blunt trauma, loss of vital signs before ED arrival | ~0.2% |
| Neurologically intact survival, blunt trauma | 0.7-2.4% |
Sources: Mulholland & Greenfield's Surgery 7e, Current Surgical Therapy 14e, Tintinalli's Emergency Medicine
REBOA (Resuscitative Endovascular Balloon Occlusion of the Aorta)
REBOA is increasingly being used as an adjunct or alternative to open aortic cross-clamping in TCA from non-compressible torso hemorrhage (NCTH). The balloon is inserted percutaneously through a femoral artery sheath and inflated in the descending thoracic aorta (Zone 1 for abdominal hemorrhage, Zone 3 for pelvic hemorrhage).
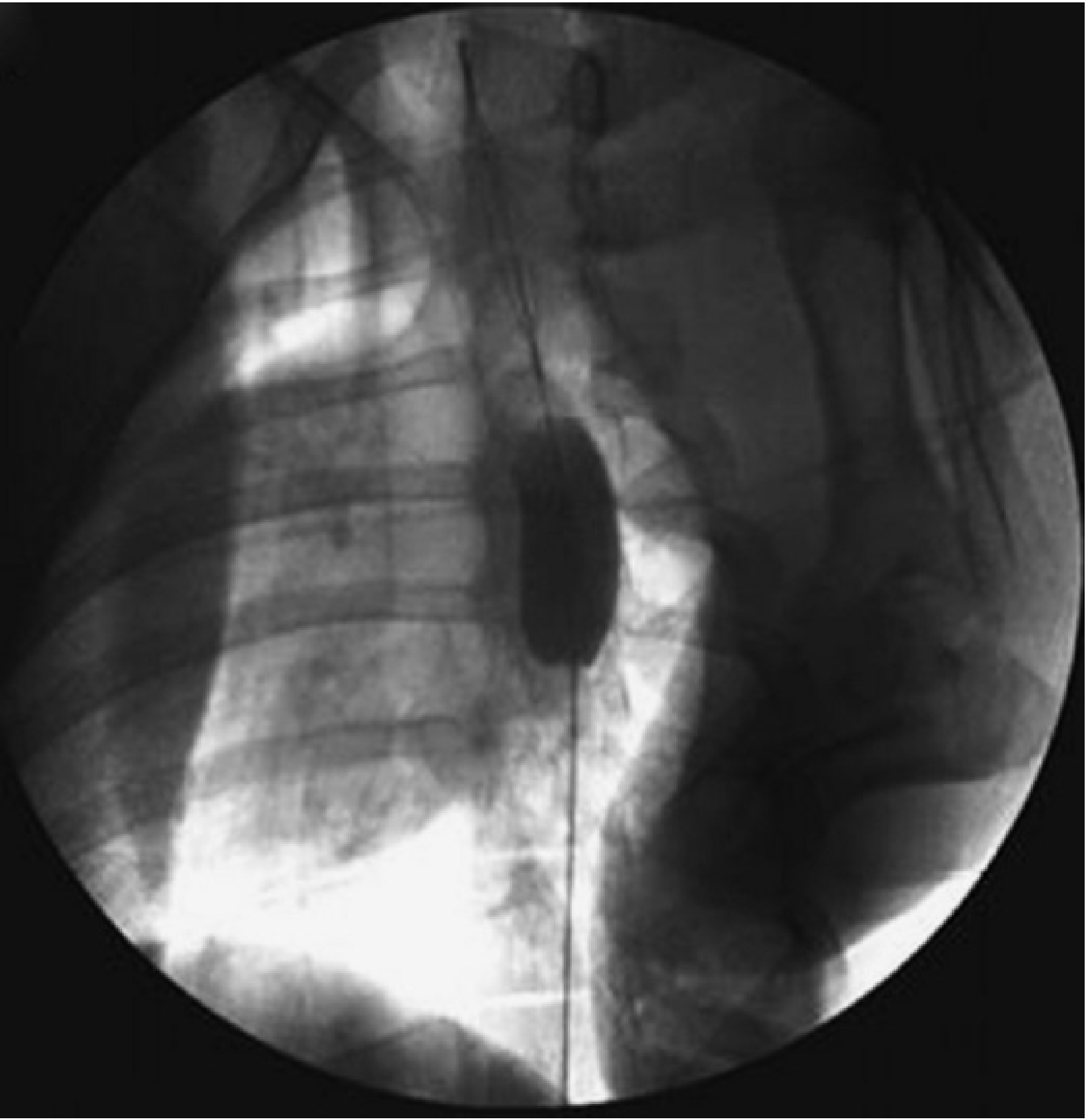
REBOA: percutaneous balloon occlusion through the femoral artery - an alternative to open resuscitative thoracotomy with aortic clamping in selected cases.
Its role in the prehospital and ED setting remains controversial, and it does not address tamponade or thoracic hemorrhage - open thoracotomy remains necessary for those.
Termination of Resuscitation
Evidence-based criteria to not initiate or to terminate resuscitation in TCA:
- No pulse or respiration in the field after blunt trauma
- Prolonged pulselessness before arrival (>15 min penetrating; >10 min blunt)
- No cardiac activity on bedside ultrasound with no tamponade
- Massive, non-survivable injuries (severe head injury, torso evisceration, decapitation)
- An organized algorithm incorporating FAST, mechanism, field vital signs, and cardiac electrical activity should guide decision-making
Key Clinical Pearls
- TCA is not medical cardiac arrest - epinephrine and standard ACLS are not the priority; reversing the mechanical cause is.
- FAST is your most powerful diagnostic tool - tamponade, pneumothorax, and cardiac activity can be assessed in <60 seconds.
- Bilateral thoracostomies should be performed early in all TCA patients to rule out/treat tension pneumothorax.
- Penetrating > Blunt for resuscitative thoracotomy - blunt TCA with prehospital arrest has essentially zero survival from EDT.
- Stab wound to the cardiac box with witnessed arrest is the highest-yield scenario for EDT.
- Pacing is not a standard TCA intervention but may be considered in selected patients with non-penetrating cardiac trauma and conduction disturbances.
- REBOA is replacing open aortic cross-clamping in many centers for NCTH, but expertise and appropriate patient selection are required.
Sources: Tintinalli's Emergency Medicine (9e), Rosen's Emergency Medicine (9e), Mulholland & Greenfield's Surgery (7e), Current Surgical Therapy (14e), Miller's Anesthesia (10e), Roberts & Hedges' Clinical Procedures in Emergency Medicine, Fischer's Mastery of Surgery (8e)
This is a shared conversation. Sign in to Orris to start your own chat.