Bowel anastomosis techniques
Reading File
Finding Sources
Finding Sources
Searching PubMed
"bowel anastomosis" AND techniques
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Here is a comprehensive overview of bowel anastomosis techniques drawn from authoritative surgical references.
Bowel Anastomosis Techniques
An intestinal anastomosis joins two segments of bowel after resection. The three pillars of successful anastomotic healing are: meticulous technique, adequate blood supply, and no tension at the suture line. The submucosa is the load-bearing layer and must always be included in any repair.
1. Anastomotic Configuration
The geometry chosen depends on the caliber discrepancy between the two bowel ends and the anatomical location.
| Configuration | When Used | Notes |
|---|---|---|
| End-to-End | Segments of similar caliber; rectal resections, colocolostomy, small bowel | Most anatomically "natural"; used for most colorectal anastomoses |
| End-to-Side | Proximal limb smaller than distal (e.g., chronic obstruction) | Closes the end of the larger segment; allows size mismatch |
| Side-to-End | Proximal bowel of smaller caliber (e.g., ileorectal anastomosis) | May have better blood supply than end-to-end |
| Side-to-Side | Ileocolic or small bowel anastomoses; size discrepancy | Large, well-vascularized connection on the antimesenteric side |
Functional end-to-end (created with a linear stapler in side-to-side fashion, then closing the common entry) is the most common configuration for ileocolic anastomoses.
2. Hand-Sewn Techniques
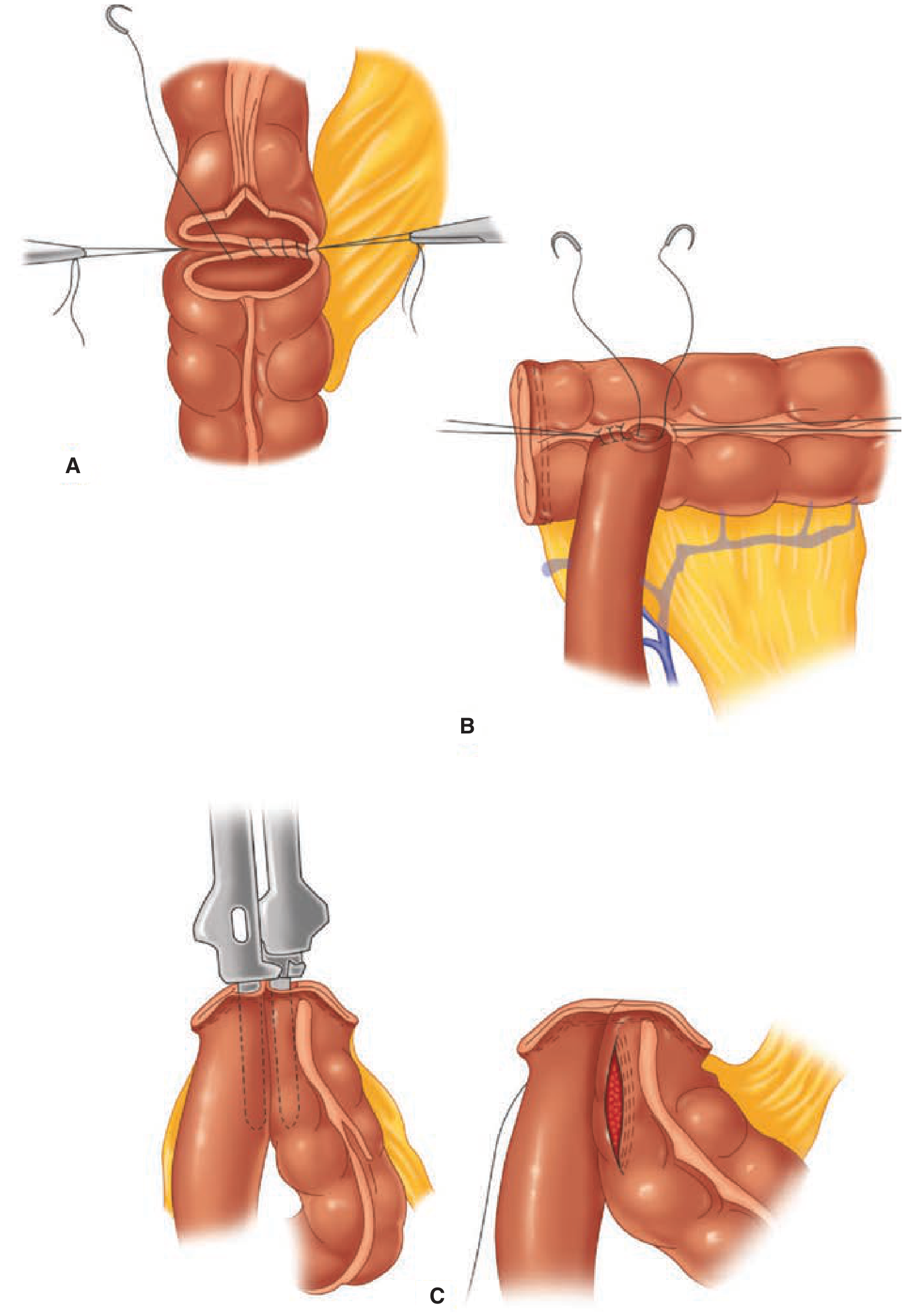
Figure: A. Sutured end-to-end colocolic anastomosis. B. Sutured end-to-side ileocolic anastomosis. C. Stapled side-to-side (functional end-to-end) ileocolic anastomosis.
All four geometric configurations above can be created with hand-sewn technique.
Single-Layer
- Running or interrupted absorbable sutures through all layers (full-thickness) or the submucosa/muscularis
- Faster to construct than two-layer
- Less tissue inversion; lower theoretical risk of lumen narrowing
Double-Layer
- Inner layer: continuous (often absorable), incorporating the mucosa and submucosa
- Outer layer: interrupted seromuscular (Lembert) stitches, inverting the suture line
- Traditional "gold standard" but more time-consuming
- Suture material may be permanent (polypropylene) or absorbable (polyglycolic acid, chromic)
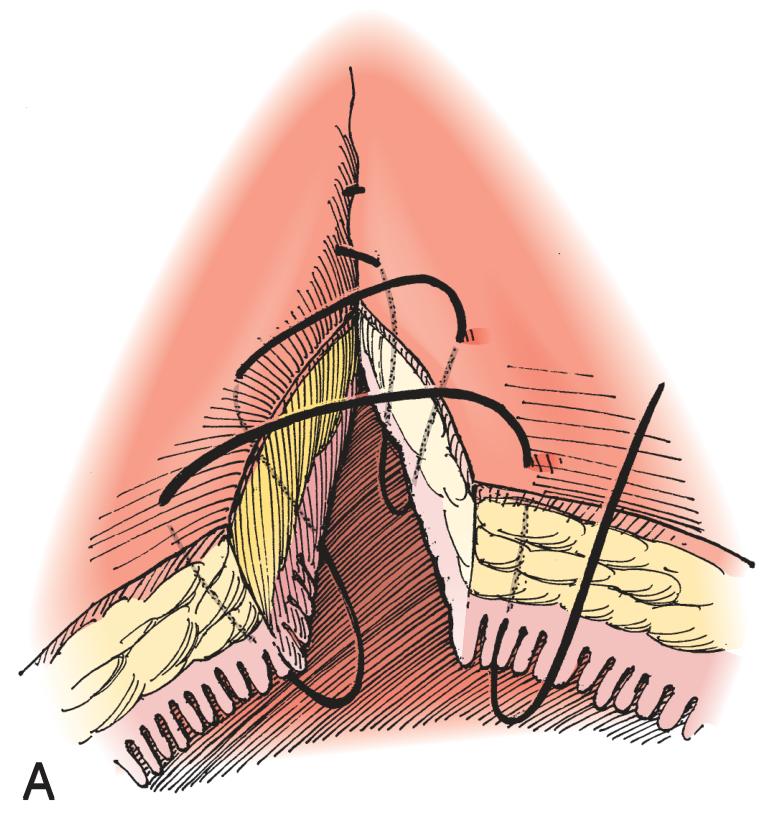
Special: Hand-Sewn Coloanal / Transanal
- After low rectal or anal canal resection where the anatomy makes stapling impossible
- Performed transanally, optionally with anal canal mucosectomy to place the anastomosis at the dentate line
-
- Schwartz's Principles of Surgery, 11e, p. 1302
3. Stapled Techniques
Stapled anastomoses have complication rates equivalent to hand-sewn; they may be slightly faster, particularly when multiple anastomoses are needed. Hand-sewn is preferred with significant bowel edema, size mismatch, or friable tissue.
Linear Cutting/Stapling Device (GIA)
- Used to divide bowel and create side-to-side (functional end-to-end) anastomoses
- Two limbs of bowel are placed side-by-side; the stapler fires two staggered rows of staples and cuts between them
- The common enterotomy/colotomy is then closed with a linear stapler or hand-sewn
- Can be reinforced with interrupted sutures if desired
Circular Cutting/Stapling Device (EEA/CDH)
- Creates end-to-end, end-to-side, or side-to-end anastomoses
- Particularly valuable for low rectal and anal canal anastomoses where the confined pelvis makes hand-sewing extremely difficult
- Two techniques for rectal stump purse-string:
- Open purse-string technique: the distal rectal stump purse-string is placed by hand; the assembled stapler is inserted transanally and guided to the rectal stump
- Double-staple technique (now preferred): the rectal stump is divided with a linear stapler across the rectal stump; the circular stapler's trocar is deployed through the linear staple line and mated with the anvil in the proximal colon; the instrument is closed and fired
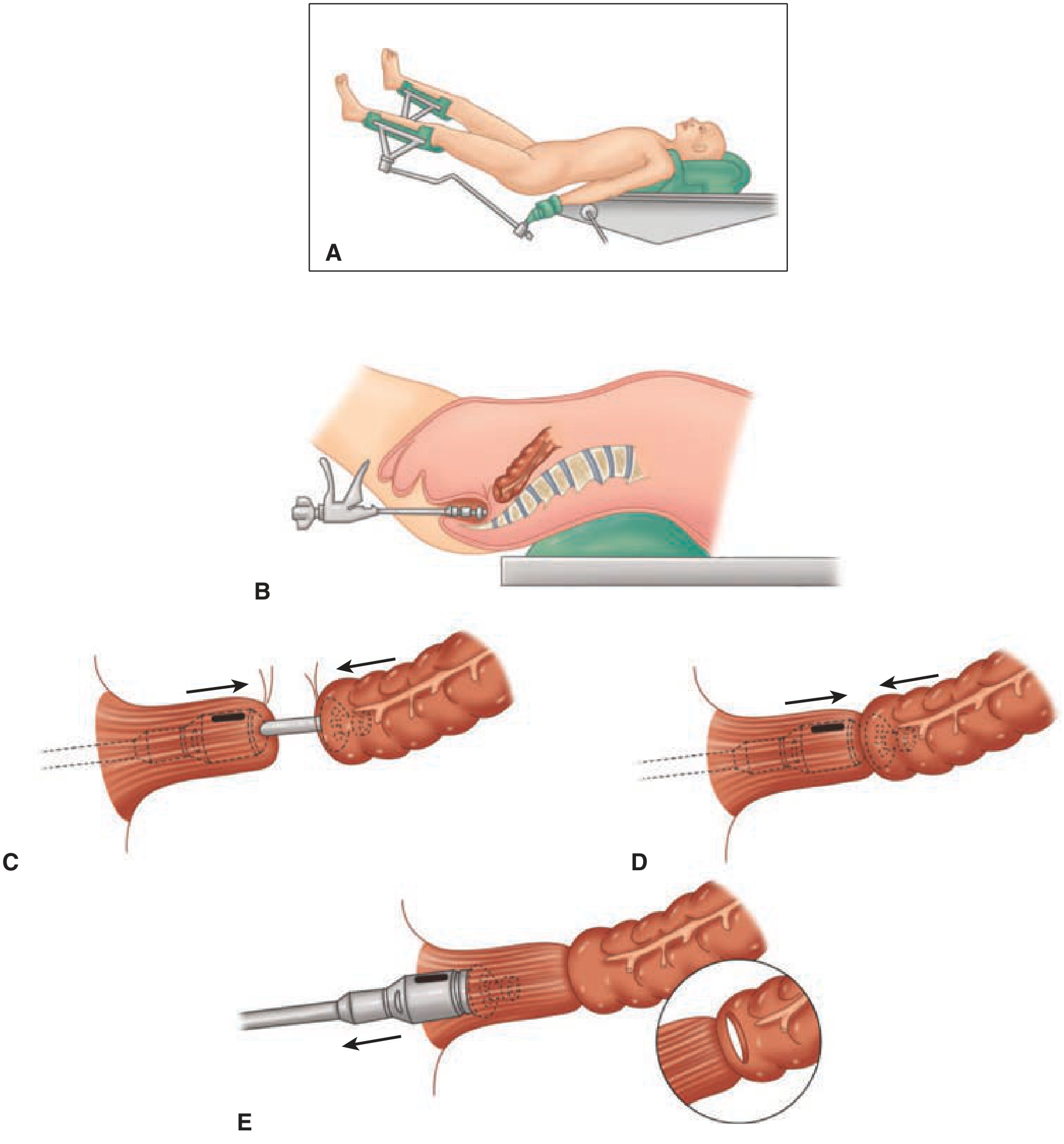
Figure: End-to-end colorectal anastomosis using a circular stapler. The stapler is inserted transanally, the bowel ends are secured with purse-string sutures to the anvil and rod, the device is closed and fired, leaving a circular double-stapled anastomosis.
-
- Schwartz's Principles of Surgery, 11e, p. 1302
4. Factors Affecting Anastomotic Healing
From Sabiston Textbook of Surgery and Schwartz's Principles of Surgery:
Definitive risk factors for anastomotic leak:
| Factor | Detail |
|---|---|
| Technical failure | Gaps in suture line, stapler misfiring, misplaced sutures, enterotomy near suture line |
| Poor blood supply | Most common cause of failure |
| Tension | Inadequate bowel mobilization |
| Location | Distal rectal/anal canal > intraperitoneal colorectal > small bowel |
| Local sepsis | Peritoneal soilage, fluid collection, irradiated bowel |
| Bowel disease | Crohn disease, radiation injury, obstruction |
Implicated (modifiable) factors: malnutrition, smoking, steroids, obesity, neoadjuvant therapy, emergency surgery, coagulopathy, zinc/vitamin C/vitamin A deficiency.
5. Specific Situations
| Clinical Setting | Preferred Approach |
|---|---|
| Edematous bowel, bowel trauma | Hand-sewn (stapler misfire risk) |
| Low rectal resection (LAR) | Circular stapler - double-staple technique |
| Ileoanal pouch (IPAA) | Stapled (now preferred over mucosectomy + hand-sewn) |
| Significant size mismatch | End-to-side or side-to-side; or antimesenteric corner incision to enlarge the smaller end |
| Irradiated/diseased bowel | Avoid anastomosis if possible; consider diverting stoma |
| Damage control (edematous at re-look) | Hand-sewn preferred |
6. Intraoperative Testing
After completion, the anastomosis is routinely tested for integrity:
- Air leak test: submerge in saline, insufflate air transanally - bubbles indicate a defect
- Dye test: transanal instillation of methylene blue or dilute betadine
- Palpation: assess for gaps and tissue vascularity
Summary
Neither hand-sewn nor stapled technique has been proven uniformly superior; the choice is guided by location, tissue quality, size match, and surgeon experience. The non-negotiable requirements for any anastomosis are: tension-free approximation, well-vascularized ends, and meticulous incorporation of the submucosa. High-risk anastomoses (low rectal, irradiated bowel, contaminated field, malnourished patient) warrant consideration of a proximal diverting stoma to protect the join while healing occurs.
- Schwartz's Principles of Surgery, 11e, p. 1348-1302
- Sabiston Textbook of Surgery, p. 454
- Current Surgical Therapy, 14e
- Maingot's Abdominal Operations
Named suture technique
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Loading Image
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Loading Image
I now have comprehensive material from authoritative surgical atlases. Here is the complete overview.
Named Suture Techniques in Surgery (Especially Bowel Anastomosis)
1. Lembert Suture
Introduced by: Antoine Lembert (1826) - the first technique that made satisfactory intestinal anastomosis possible.
Type: Interrupted or continuous; inverting seromuscular suture
Layers included: Serosa + muscularis + upper submucosa (does NOT penetrate mucosa)
Action: Inverts the bowel wall, producing serosal apposition between the two limbs - serosal contact is what promotes healing.
Technique:
- Insert the needle at ~4-5 mm from the cut edge, passing through serosa and muscularis into (but not through) the submucosal layer
- Exit on the same side symmetrically, then repeat on the opposing bowel segment
- Tying inverts the tissue so serosa faces serosa
Uses:
- Outer (second) layer of a two-layer anastomosis
- Closure of the end of the bowel (over a clamp)
- One-layer interrupted anastomosis (inverting)
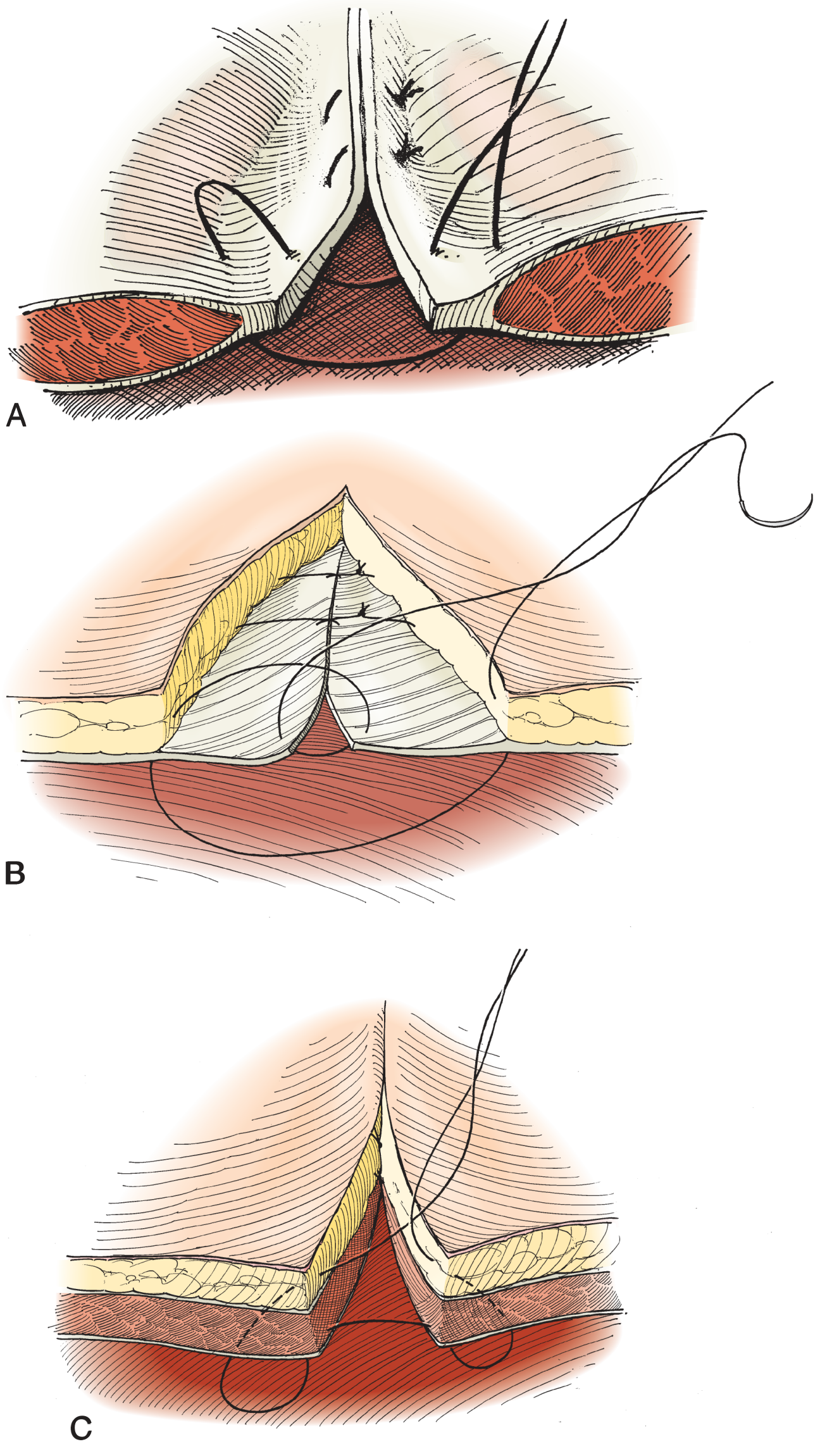
Figure: A. Interrupted Lembert suture placement. B. Continuous Lembert suture. C. Closing bowel end over clamp with interrupted Lembert sutures.
- Hinman's Atlas of Urologic Surgery, p. 36
2. Connell Suture
Type: Continuous running; inverting full-thickness suture (also called the "U-stitch" or loop-on-mucosa stitch)
Layers included: All layers (full-thickness)
Action: Each bite enters from outside, passes through all layers, comes back out through the mucosa on the same side (forming a loop on the mucosal surface), crosses to the other limb and repeats - the tissue inverts as the suture is tightened.
Technique:
- Enter from outside → full thickness → exit through mucosa (inside)
- Cross to other side of the anastomosis → enter through mucosa → exit full thickness
- The suture runs along the mucosal surface as a "loop" between bites
- Produces a smooth mucosal-to-mucosal inversion
Uses:
- Inner (first) layer of a classic two-layer bowel anastomosis, particularly the anterior wall
- Commonly used after a Cushing stitch finishes the posterior wall
- Transition suture at the corners of an anastomosis (the "angle stitch")
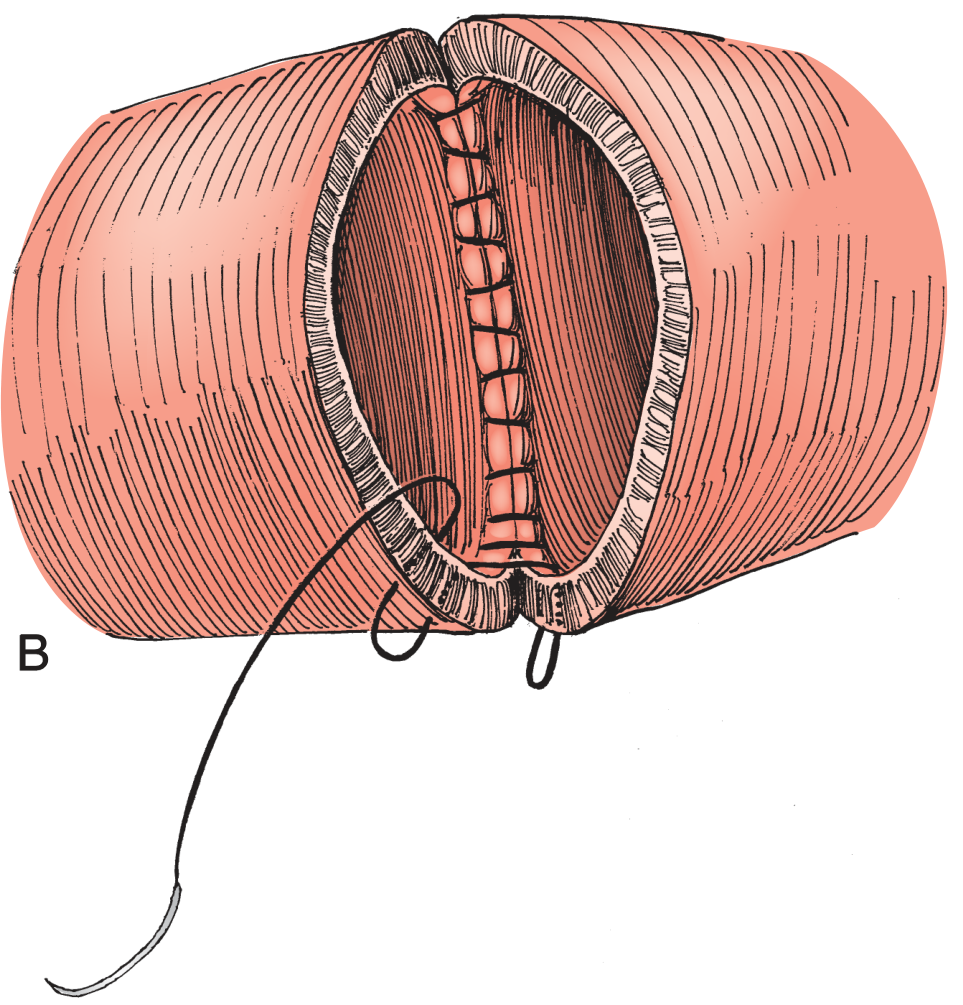
Figure: Connell suture forming the inner mucosal inverting layer of a bowel anastomosis.
- Campbell-Walsh-Wein Urology, p. (anastomosis chapter)
3. Cushing Suture
Type: Continuous running; inverting seromuscular suture (like a running Lembert)
Layers included: Serosa + muscularis (does not enter the lumen)
Action: A running version of the Lembert - inverts the serosa without entering the mucosa.
Technique:
- Run continuous bites through serosa and muscularis only, parallel to the cut edge
- Each bite is placed on the same side and the suture advances along the wall
Uses:
- Outer layer of a two-layer anastomosis (running alternative to interrupted Lembert)
- Posterior outer layer of anastomosis before the Connell anterior layer
Relationship to Connell: Together they form the classic two-layer anastomosis:
- Posterior outer: Cushing (or interrupted Lembert)
- Posterior inner: Connell (inverting, full thickness)
- Anterior inner: Connell continued
- Anterior outer: Cushing (or interrupted Lembert)
4. Halsted Suture
Type: Interrupted; inverting seromuscular (mattress variant)
Layers included: Serosa + muscularis
Action: A horizontal mattress variation of the Lembert - provides greater inversion and serosa-to-serosa contact.
Technique:
- Pass suture through the seromuscular layer parallel to the cut edge on one side
- Cross to the opposing bowel and pass through the seromuscular layer parallel to the edge
- Tie to produce horizontal mattress inversion
Uses:
-
Outer layer reinforcement stitch
-
Closing small bowel enterotomies
-
Inverting the skin edge (dermal version)
-
Hinman's Atlas of Urologic Surgery (described as "inverts the edge")
5. Gambee Suture
Type: Interrupted; single-layer; approximating (neither purely inverting nor everting)
Layers included: Full thickness - but with a specific mucosal loop
Action: Achieves a two-layer closure effect with a single pass, preventing mucosal eversion while maintaining mucosal apposition.
Technique:
- Enter through full thickness of bowel A (outside → in)
- Come back out through only the mucosa/submucosa of bowel A (inside → mucosa, not exiting the serosa)
- Cross to bowel B and enter through the mucosa/submucosa (mirror image)
- Exit through the full thickness of bowel B (inside → outside)
- Tie - the knot sits on the serosa; the mucosal loop inverts gently without mucosa prolapse
Advantage: Prevents mucosal eversion (which can cause anastomotic problems), achieves submucosa-to-submucosa contact in one layer, and reduces lumen narrowing compared to inverting techniques.
Uses:
- Single-layer enteroenterostomy (especially where lumen size is limited)
- Pyloroplasty reconstruction
- Preferred by many urologists for intestinal anastomosis in urinary diversion
"Some prefer to use a Gambee stitch at this point, which involves placing the suture through the full thickness of the bowel followed by traversing a small segment of mucosa of each segment of bowel before exiting through the full thickness of the bowel of the other segment." - Campbell-Walsh-Wein Urology
6. Purse-String Suture
Type: Continuous circumferential suture around a defect
Action: When tied, closes a circular opening by drawing the edges inward (like a drawstring bag).
Uses:
- Inversion of the appendix stump
- Securing bowel ends to a circular stapler (EEA) anvil and rod during colorectal anastomosis
- Closing a hernia sac
- Securing drainage tubes (e.g., T-tube, cecostomy)
7. Lock-Stitch (Over-and-Over Locked)
Type: Continuous running suture with periodic locking
Action: Every 3rd-4th bite, the suture passes under the previous loop, "locking" it in place - prevents puckering and distributes tension evenly.
Uses:
- Mucosal edge closure
- When running sutures tend to bunch or pucker
- Hemostatic inner layer
8. Figure-Eight Bowel Suture
Type: Interrupted; approximating
Layers included: Full thickness on the outside bites; mucosa/submucosa on the inside bites
Action: Approximates mucosa independently from the muscularis/serosa in a single stitch (similar principle to Gambee but with a different needle path).
Technique:
- Pass suture through all layers on one side
- On the same side, pass back through mucosa and submucosa only
- Cross to the other side and pass through mucosa and submucosa
- Exit through all layers on the other side
- The stitch forms a figure-eight pattern
Summary Table
| Suture | Type | Layers | Action | Primary Use |
|---|---|---|---|---|
| Lembert | Interrupted or continuous | Serosa + muscularis + upper submucosa | Inverting | Outer layer of anastomosis; gold standard seromuscular stitch |
| Connell | Continuous running | Full thickness | Inverting (mucosal loop) | Inner layer (anterior wall) of 2-layer anastomosis |
| Cushing | Continuous running | Serosa + muscularis only | Inverting | Outer layer, running alternative to Lembert |
| Halsted | Interrupted mattress | Serosa + muscularis | Inverting (horizontal mattress) | Outer layer reinforcement, enterotomy closure |
| Gambee | Interrupted | Full thickness + mucosal loop | Approximating (prevents eversion) | Single-layer anastomosis, pyloroplasty |
| Purse-string | Continuous circumferential | Variable | Inverting/closing | Appendix stump, EEA stapler, hernia sac |
| Lock-stitch | Continuous locked | Mucosal layer | Approximating | Mucosal edge closure, hemostasis |
| Figure-eight | Interrupted | Full thickness + submucosal loop | Approximating | Bowel approximation (rarely used now) |
The Classic Two-Layer Bowel Anastomosis
The traditional approach uses four named stitches in sequence:
- Posterior outer layer - interrupted Lembert sutures (or running Cushing)
- Posterior inner layer - continuous Connell suture (full-thickness inverting)
- Anterior inner layer - Connell continued (the running suture turns the corner)
- Anterior outer layer - interrupted Lembert (or running Cushing)
The mesenteric corner is the most critical area - most leaks occur here due to difficult suture placement through the mesenteric border.
- Hinman's Atlas of Urologic Surgery
- Campbell-Walsh-Wein Urology
- Maingot's Abdominal Operations
- Fischer's Mastery of Surgery, 8e
This is a shared conversation. Sign in to Orris to start your own chat.