A 45-year-old smoker develops hypertension and myocardial infarction. Discuss the 'Natural History of Disease', levels of prevention, and the web of causation. ( Community Medicine mbbs 15 marks)
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have all the material needed for a comprehensive 15-mark answer. Let me compose the full structured response.
Natural History of Disease, Levels of Prevention, and Web of Causation
Applied to a 45-Year-Old Smoker with Hypertension and Myocardial Infarction
(Source: Park's Textbook of Preventive and Social Medicine)
PART 1: NATURAL HISTORY OF DISEASE
The natural history of disease refers to the way a disease evolves over time from its earliest beginnings in the prepathogenesis phase to its final outcome - recovery, disability, or death - in the absence of any treatment or prevention (Leavell & Clark model).
The classic diagram from Park's (Fig. 8) captures this perfectly:
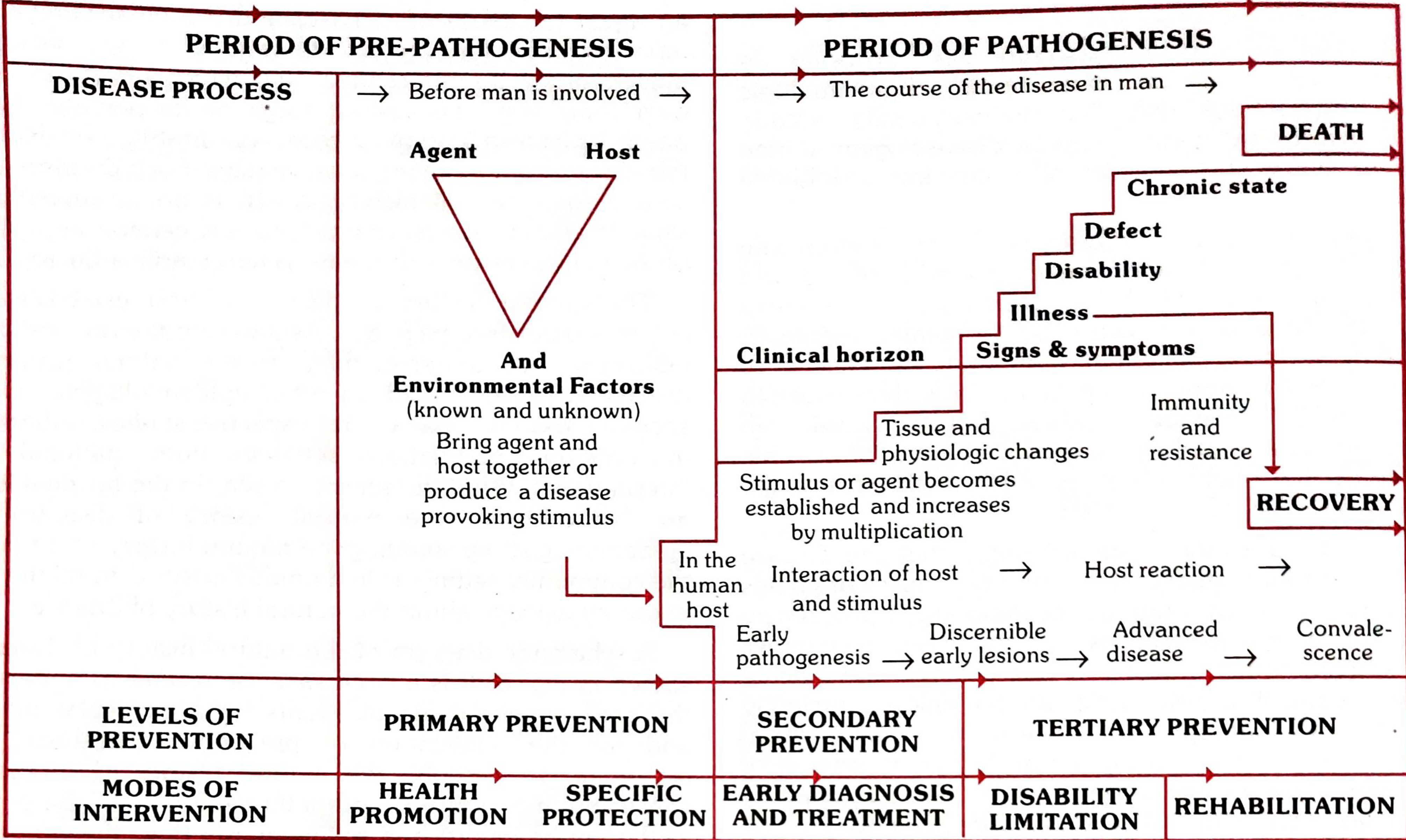
Disease results from a complex interaction between Man (Host), Agent, and Environment - the epidemiological triad.
Phase 1: Pre-Pathogenesis Phase
This is the period before disease onset in man. The causative factors have not yet entered the host, but the conditions for their interaction are already present in the environment.
In our case (45-year-old smoker):
- Host factors: Age (45 yrs, male sex), genetic predisposition to hypertension or dyslipidaemia, sedentary habits, possible obesity or stress
- Agent factors: Nicotine, carbon monoxide (from smoking), dietary saturated fats, excess sodium intake
- Environmental factors: Socioeconomic stressors, occupational pressures, sedentary lifestyle, abundance of food (high-calorie diet), lack of physical exercise
At this stage, the person is "man in the midst of disease" - exposed to risk factors but not yet clinically ill. This is the ideal time for primary prevention.
Phase 2: Pathogenesis Phase
This phase begins with the entry of the agent into the susceptible host. In chronic non-communicable diseases like MI, there is no single agent, but the disease evolves through:
| Sub-stage | What happens | In our patient |
|---|---|---|
| Early pathogenesis | Tissue changes begin; below clinical horizon | Endothelial injury, early fatty streaks in coronary arteries; asymptomatic hypertension begins |
| Discernible early lesions | Disease detectable by screening | Raised BP on measurement, early atherosclerotic plaques on imaging |
| Advanced disease / Clinical illness | Signs and symptoms appear (cross the clinical horizon) | Chest pain, angina, hypertension diagnosed clinically |
| Outcome | Recovery, disability, or death | Myocardial infarction; if untreated - heart failure, arrhythmia, sudden cardiac death |
The clinical horizon is the threshold at which the disease becomes clinically apparent. Below this horizon, disease exists but cannot be detected without screening tools.
The natural history of MI in a smoker can be summarized as:
Smoking + Risk factors → Endothelial injury → Atherosclerosis → Coronary stenosis → Plaque rupture → Coronary occlusion → Myocardial ischaemia → Myocardial Infarction → Heart failure / arrhythmia / death
PART 2: WEB OF CAUSATION
The web of causation was proposed by MacMahon and Pugh (1970) in their book "Epidemiologic Principles and Methods." This model is ideally suited to the study of chronic diseases where no single agent is responsible, but the disease results from the interaction of multiple factors.
The web considers all predisposing factors of any type and their complex interrelationship with each other. The classic example used in Park's textbook is the web for myocardial infarction:
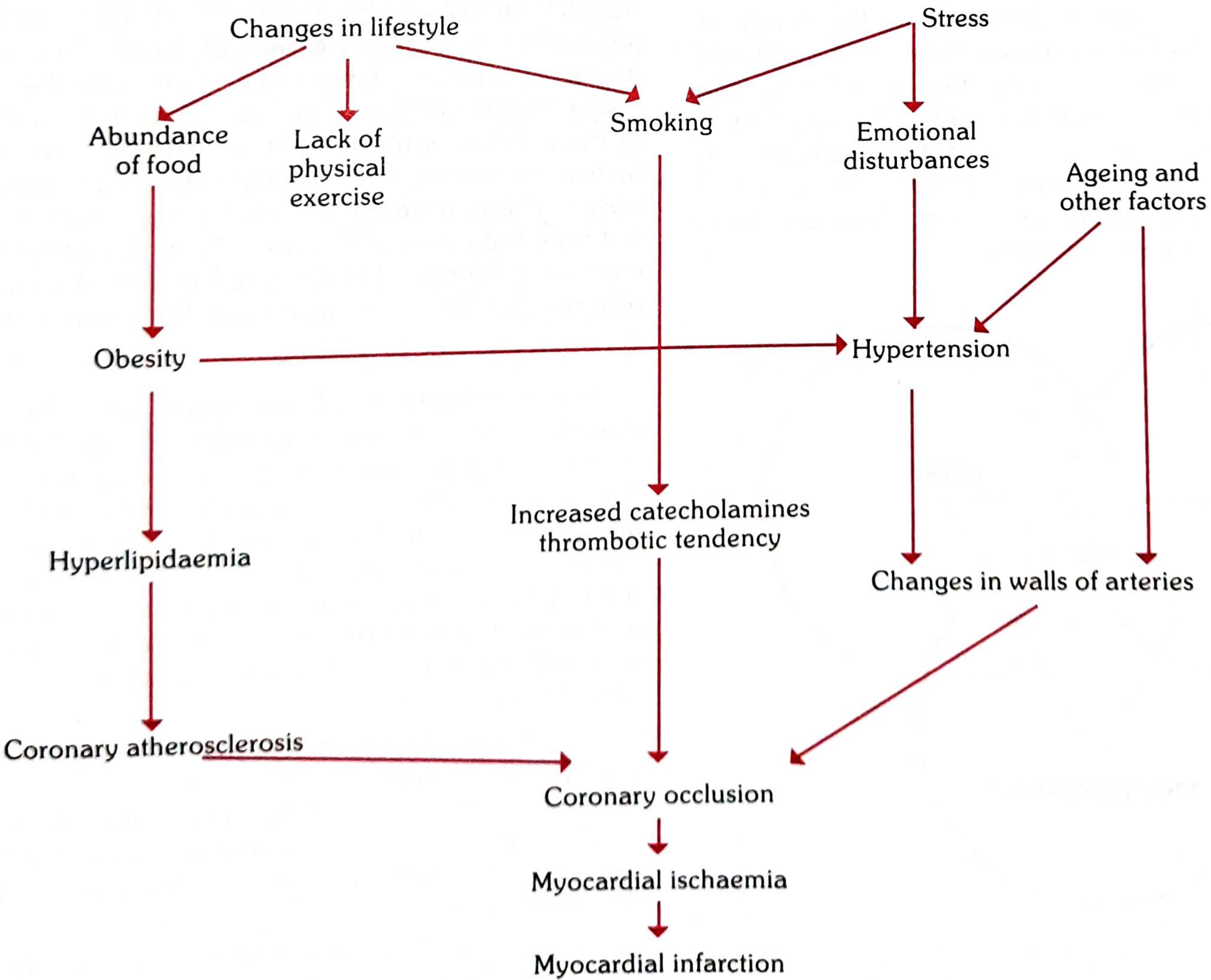
Components of the Web for This Patient
Upstream (distal) causes:
- Changes in lifestyle (modern urbanization)
- Abundance of food → Obesity
- Lack of physical exercise → Obesity
- Stress → Emotional disturbances → Hypertension
- Ageing and genetic factors → Hypertension
Intermediate links:
- Smoking (directly from lifestyle change + stress): increases catecholamines, thrombotic tendency, endothelial damage
- Obesity → Hyperlipidaemia → Coronary atherosclerosis
- Obesity → Hypertension
- Hypertension → Changes in walls of arteries
Proximal (immediate) causes converging to MI:
- Coronary atherosclerosis
- Increased catecholamines and thrombotic tendency (from smoking)
- Changes in arterial walls (from hypertension)
- These three paths all converge on → Coronary occlusion → Myocardial ischaemia → Myocardial Infarction
Key Principle of the Web
The web of causation does not imply that all causal links must be removed to control disease. Sometimes the removal of even one important link can break the chain and prevent the final outcome. For example:
- Stopping smoking alone can significantly reduce risk of MI (reduces catecholamines, thrombosis risk, and reverses some endothelial changes)
- Treating hypertension alone substantially reduces arterial wall damage
- The relative importance of individual factors is expressed as relative risk
PART 3: LEVELS OF PREVENTION
In modern preventive medicine, four levels of prevention are recognized, all mapped to the natural history of disease (Park's Textbook, Table 10):
Level 0: Primordial Prevention
Definition: Prevention of the emergence or development of risk factors in populations where they have not yet appeared.
Applied to our case (ideally, during childhood/adolescence):
- Discouraging the patient from ever starting smoking
- Promoting healthy diet and physical activity from childhood
- Preventing obesity and sedentary lifestyle through school-level health education
- Main intervention: Individual and mass education (policy-level changes - no-smoking zones, taxes on tobacco, food labeling laws)
Level 1: Primary Prevention
Definition: "Action taken prior to the onset of disease which removes the possibility that a disease will ever occur." - Acts in the pre-pathogenesis phase.
Two approaches (WHO):
a. Population (Mass) Strategy:
Directed at the whole population regardless of individual risk. Even a small reduction in average blood pressure or serum cholesterol across a population produces a large reduction in cardiovascular disease incidence.
- Salt reduction in food supply
- Anti-tobacco campaigns
- Promoting physical activity at community level
b. High-Risk Strategy:
Targeted at individuals already identified as at high risk (like our 45-year-old smoker with hypertension):
- Aggressive smoking cessation counselling
- Antihypertensive therapy before MI occurs
- Lipid-lowering therapy (statins)
- Anti-platelet agents (aspirin in high-risk individuals)
- Dietary modification, weight reduction, regular aerobic exercise
Modes of intervention at this level:
- Health promotion - balanced diet, regular exercise, stress management, healthy lifestyle counselling
- Specific protection - smoking cessation, blood pressure control, lipid management, vaccination against influenza (reduces cardiac events), aspirin prophylaxis
Level 2: Secondary Prevention
Definition: "Action which halts the progress of disease at its incipient stage and prevents complications." - Acts at the early pathogenesis phase (around the clinical horizon).
Specific interventions:
- Early diagnosis through screening: BP measurement, ECG screening, lipid profile, blood glucose, coronary CT angiography
- Case-finding programmes: Opportunistic BP checks in smokers
- Adequate treatment once disease detected:
- Antihypertensives (ACE inhibitors, beta-blockers, CCBs)
- Statins for dyslipidaemia
- Aspirin and antiplatelet therapy
- Management of acute MI: thrombolytics, primary PCI (percutaneous coronary intervention)
- Beta-blockers, ACE inhibitors post-MI
Secondary prevention is largely the domain of clinical medicine. It attempts to arrest the disease process and restore health before irreversible pathological changes occur.
Mode of intervention: Early diagnosis and treatment
Level 3: Tertiary Prevention
Definition: "All measures available to reduce or limit impairments and disabilities, minimize suffering caused by existing departures from good health, and to promote the patient's adjustment to irremediable conditions."
Applied after established MI (late pathogenesis phase):
- Disability limitation:
- Cardiac rehabilitation (graded exercise, dietary counselling post-MI)
- Prevention of recurrent MI (dual antiplatelet, long-term statins, ACE inhibitors, beta-blockers)
- Management of heart failure, arrhythmias, and other complications
- Strict smoking cessation and lifestyle modification post-MI
- Rehabilitation:
- Physical rehabilitation (cardiac rehab program)
- Psychological support (depression is common post-MI)
- Vocational rehabilitation (return to appropriate work)
- Social support and education about self-management
Mode of intervention: Disability limitation + Rehabilitation
SUMMARY TABLE: Levels of Prevention Applied to this Case
| Level | Phase | Goal | Example in this Patient |
|---|---|---|---|
| Primordial | Before risk factors emerge | Prevent risk factor development | Never start smoking; healthy childhood diet |
| Primary | Pre-pathogenesis | Prevent disease onset | Smoking cessation, BP control, statins, exercise |
| Secondary | Early pathogenesis | Halt disease, prevent complications | BP screening, lipid testing, early antihypertensive Rx, acute MI management (PCI) |
| Tertiary | Late pathogenesis | Reduce disability, rehabilitation | Cardiac rehab, secondary prevention drugs, vocational rehab |
CONNECTING ALL THREE CONCEPTS
The natural history of disease provides the framework on which the levels of prevention are applied. The web of causation for MI shows that multiple interacting factors (smoking, obesity, hypertension, hyperlipidaemia, stress, aging) together produce the disease, and that intervention at any one node of the web can reduce the probability of the final outcome. This is why preventive strategies are most effective when applied upstream (primordial/primary levels) before irreversible pathological changes have occurred.
"What the physician sees in the hospital is just an 'episode' in the natural history of disease. The epidemiologist, by studying the natural history of disease in the community setting, is in a unique position to fill the gaps." - Park's Textbook of Preventive and Social Medicine
Source: Park's Textbook of Preventive and Social Medicine (Park, 2013) - the authoritative reference for Community Medicine in Indian MBBS curriculum.
This is a shared conversation. Sign in to Orris to start your own chat.