Mucoepidermoid carcinoma according to shafers 10th edition long answer type question for bds dental student
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive information from authoritative sources. While Shafer's 10th edition is not directly available in the library, I have equivalent or superior content from Robbins Pathologic Basis of Disease (the gold standard pathology reference) and Cummings Otolaryngology, which closely mirrors what Shafer's covers. Let me now compile the comprehensive long-answer format for BDS students.
Mucoepidermoid Carcinoma - Long Answer (BDS Examination Format)
(Based on standard oral pathology content as per Shafer's Textbook of Oral Pathology; supplemented by Robbins & Kumar Pathologic Basis of Disease and Cummings Otolaryngology Head & Neck Surgery)
Definition
Mucoepidermoid carcinoma (MEC) is the most common primary malignant tumor of the salivary glands, composed of variable mixtures of three cell types: mucous cells, squamoid (epidermoid) cells, and intermediate cells. The name is derived from its two dominant cell populations - mucous ("muco") and squamous ("epidermoid").
Incidence and Epidemiology
- Represents approximately 15% of all salivary gland tumors, making it the single most common salivary gland malignancy
- It accounts for approximately 34% of all malignant salivary gland tumors (Spiro's landmark review of 1278 cases)
- Site distribution:
- Parotid gland: 60-70% of cases (most common major salivary gland site)
- Minor salivary glands: particularly the hard palate, buccal mucosa, lip, and retromolar trigone
- Submandibular and sublingual glands: less frequent
- Central (intraosseous) MEC: arises within the mandible or maxilla from odontogenic epithelium; less aggressive behavior
- Age: Peak incidence around 45 years of age; can occur in children - in fact, MEC is the most common pediatric salivary gland carcinoma
- Sex: Slightly more common in women
Etiology and Pathogenesis
- A consistent chromosomal translocation t(11;19)(q21;p13) is found in more than 50% of MECs
- This creates a CRTC1::MAML2 fusion gene (also written as MECT1-MAML2)
- The MAML2 portion of the fusion protein cannot interact with Notch signaling components, perturbing both Notch and cAMP-dependent signaling pathways
- This translocation is associated with better prognosis and is diagnostically useful (especially in low- and intermediate-grade tumors)
- High-grade MECs are often negative for this translocation
Clinical Features
- Patients typically present with a painless, slow-growing mass
- In the parotid region, it appears as a firm or fluctuant swelling
- In the oral cavity (especially hard palate and buccal mucosa), it may appear as a bluish, fluctuant swelling that mimics a mucocele - this is due to mucin within cystic spaces imparting a blue color
- Pain, ulceration, and facial nerve involvement can occur, especially in high-grade tumors
- Intraosseous MEC may appear as a radiolucency on radiograph
Gross Pathology
- Tumors may grow up to 8 cm in diameter
- Appears circumscribed but lacks a well-defined capsule and is often infiltrative
- Cut surface is pale gray to white
- Frequently contains small, mucin-filled cysts
- Usually has both solid and cystic components
Histopathology
Three Cell Types (Classic Triad)
| Cell Type | Features |
|---|---|
| Mucous cells | Abundant light blue mucin in cytoplasm; nuclei displaced to periphery; line cystic spaces |
| Squamoid (Epidermoid) cells | Large with abundant pink cytoplasm; squamoid appearance but true keratinization is rare |
| Intermediate cells | Hybrid cells; modest pink or clear cytoplasm; usually predominate in the tumor |
- Architecture: mixture of cystic and solid elements - sheets, nests, duct-like structures, and cysts
- Mucin can be highlighted with special stains: PAS, Mucicarmine, or Alcian blue
- True keratinization is rare in MEC; its presence should raise suspicion for adenosquamous carcinoma
- Immunohistochemistry is of limited utility in diagnosis
Histological Appearances:
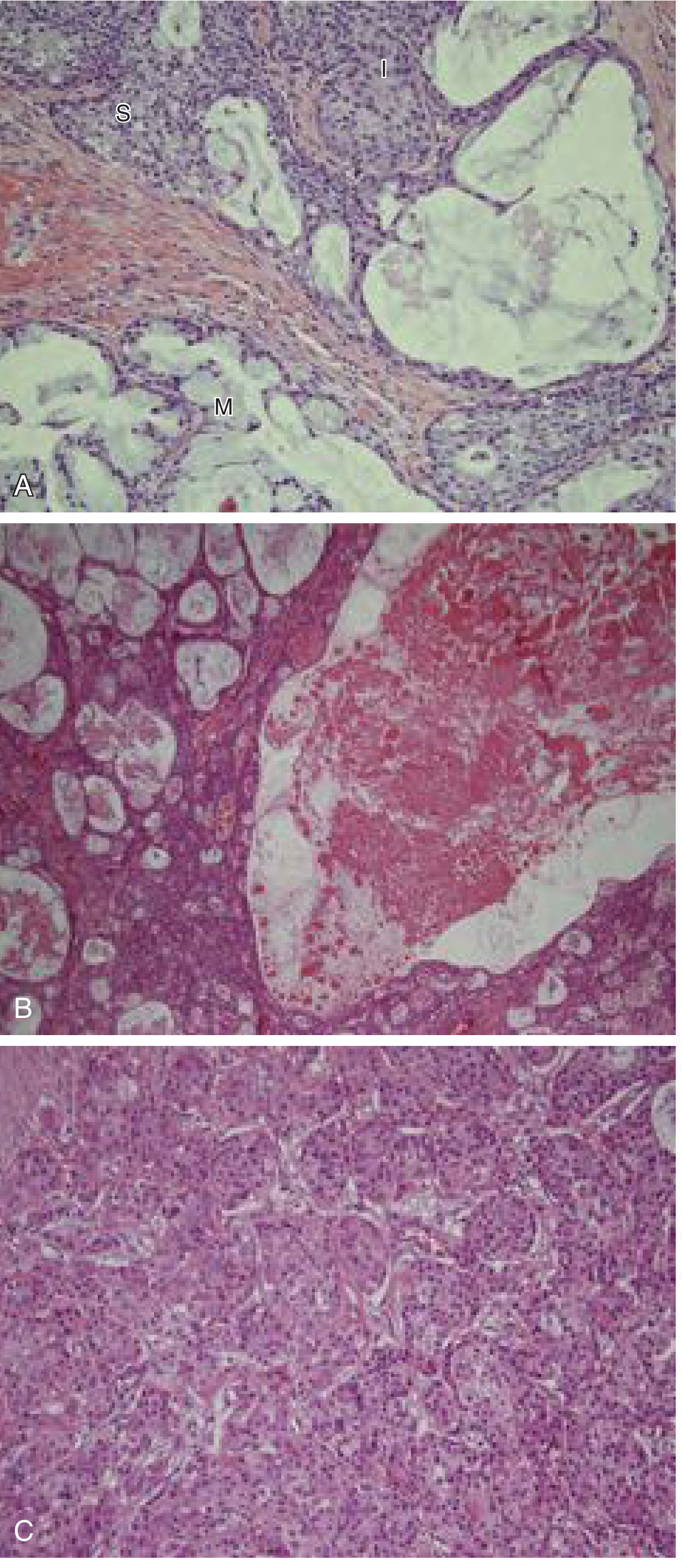
Fig: Mucoepidermoid carcinoma - (A) Three cell types: Intermediate cells (I), Mucous cells (M), and Squamoid cells (S) at x200. (B) Extensive cystic change at x100. (C) High-grade MEC: solid sheets, minimal mucous differentiation, no cystic change (Cummings Otolaryngology)
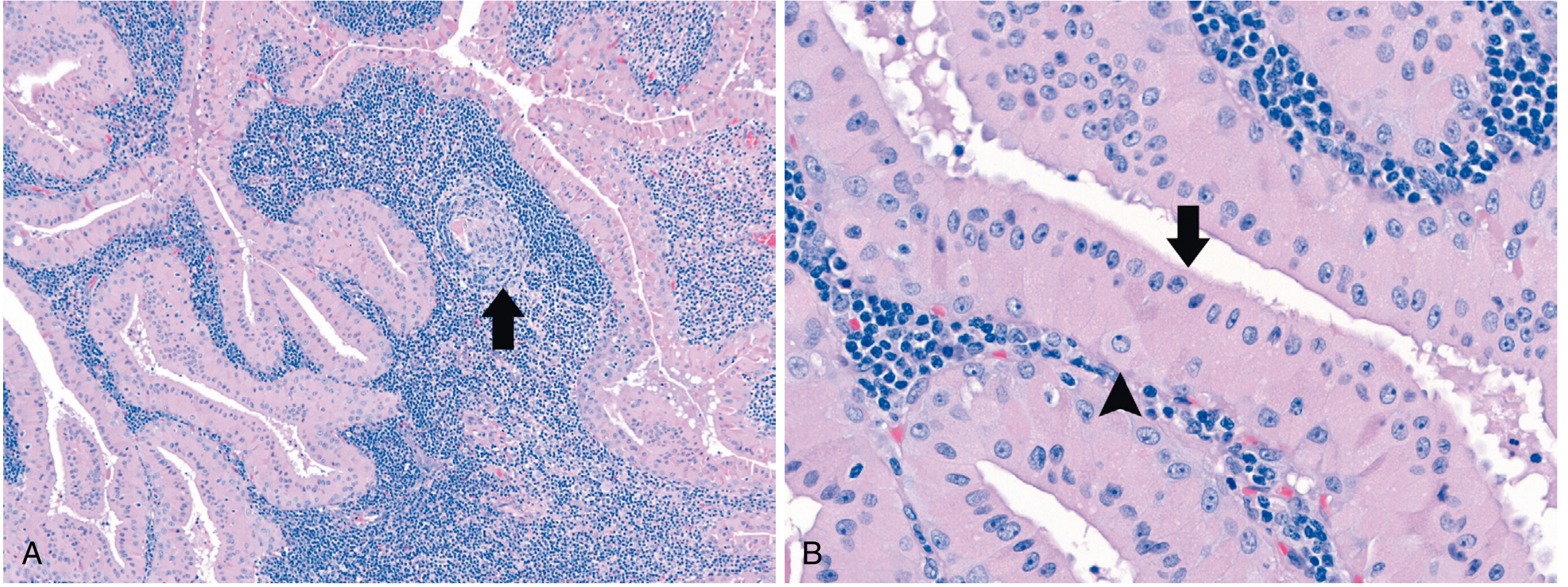
Fig: Mucoepidermoid carcinoma. (A) Low-power view: sheets and microcysts with varying cell morphologies. (B) High-power: mucinous (left), intermediate (center), and squamous (right) cells (Robbins & Kumar Pathologic Basis of Disease)
Histological Grading
Grading is crucial as it strongly correlates with clinical behavior. Two systems are widely used:
Auclair Grading System
| Parameter | Points |
|---|---|
| Cystic component <20% | +2 |
| Neural invasion | +2 |
| ≥4 mitoses/10 hpf | +3 |
| Necrosis | +3 |
| Anaplasia | +4 |
| Grade | Score |
|---|---|
| Low (Grade I) | 0-4 |
| Intermediate (Grade II) | 5-6 |
| High (Grade III) | ≥7 |
Brandwein Grading System (Modification - more stringent)
| Parameter | Points |
|---|---|
| Cystic component <25% | +2 |
| Tumor front invades in small nests/islands | +2 |
| Pronounced nuclear atypia | +2 |
| Lymphatic/vascular invasion | +3 |
| Neural invasion | +3 |
| Necrosis | +3 |
| ≥4 mitoses/10 hpf | +3 |
| Bony invasion | +3 |
| Grade | Score |
|---|---|
| Low | 0 |
| Intermediate | 2-3 |
| High | ≥4 |
(Source: Cummings Otolaryngology Head & Neck Surgery)
Low-Grade vs. High-Grade MEC - Comparative Features
| Feature | Low-Grade | High-Grade |
|---|---|---|
| Architecture | Predominantly cystic | Predominantly solid |
| Dominant cells | Mucous cells; well-differentiated | Squamoid + intermediate cells |
| Cytologic atypia | Minimal | Prominent |
| Mitoses | Low | High (≥4/10 hpf) |
| Necrosis | Absent | Present |
| Local recurrence | ~15% | 25-30% |
| Metastasis | Rare | ~30% |
| 5-year survival | >90% | ~50% |
Differential Diagnosis
- Mucocele - benign, no epithelial lining with true malignant cells; clinically mimics low-grade MEC in oral cavity
- Necrotizing sialometaplasia - non-neoplastic reactive lesion of hard palate minor salivary glands; important differential in oral cavity MECs
- Adenosquamous carcinoma - aggressive variant of SCC; has definitive squamous differentiation with keratinization (unlike MEC), surface mucosal squamous dysplasia, and more aggressive behavior
- Pleomorphic adenoma - benign; myxochondroid areas absent in MEC; no infiltrative growth
- Adenoid cystic carcinoma - basoloid cells with dark chromatin, cribriform ("Swiss cheese") pattern; perineural invasion prominent
Special Investigations
- Fine Needle Aspiration Cytology (FNAC): Yields mixture of mucinous, intermediate, and squamoid cells; both glandular and squamoid components must be present for diagnosis
- Special stains: PAS, Mucicarmine, Alcian blue - to confirm mucin in cells
- Molecular/Cytogenetics: CRTC1::MAML2 fusion gene (from t(11;19) translocation) - useful for confirmation, especially in low/intermediate-grade tumors
- Imaging (CT/MRI): For extent of disease, bone involvement, and lymph node assessment
Treatment
- Surgery is the primary treatment - wide local excision with adequate margins
- For parotid MEC: superficial or total parotidectomy depending on extent
- For submandibular gland: complete excision
- For minor salivary gland MEC: wide local excision
- Neck dissection: Indicated for clinical adenopathy or high-grade tumors
- Postoperative radiotherapy: Recommended for high-grade tumors, close/positive margins, perineural invasion, or lymph node metastasis
- Low-grade MECs of the submandibular gland recur and metastasize more frequently than parotid/minor salivary gland MECs of the same grade - warranting aggressive resection
Prognosis
| Grade | Local Recurrence | Distant Metastasis | 5-Year Survival |
|---|---|---|---|
| Low | ~15% | Rare | >90% |
| Intermediate | Variable | Variable | Intermediate |
| High | 25-30% | ~30% | ~50% |
- The CRTC1::MAML2 fusion is associated with better prognosis but this is not independent of tumor grade
- Clinical staging is equally important as histologic grade and must be considered together
Summary Points for Exam
- MEC = most common primary malignant salivary gland tumor
- Three cell types: mucous, squamoid (epidermoid), and intermediate cells
- Most common site: parotid gland (60-70%)
- Most common intraoral minor salivary gland site: hard palate
- Most common salivary gland malignancy in children
- Molecular marker: CRTC1::MAML2 fusion (t(11;19)(q21;p13))
- Grading: three grades - low, intermediate, high (Auclair or Brandwein system)
- Special stains for mucin: PAS, Mucicarmine, Alcian blue
- True keratinization is rare - if present, consider adenosquamous carcinoma
- Treatment: surgery ± postoperative radiotherapy based on grade/stage
Note: Shafer's Textbook of Oral Pathology 10th edition was not directly available in the reference library. This answer is compiled from Robbins & Kumar Pathologic Basis of Disease, Robbins Cotran & Kumar Pathologic Basis of Disease (latest edition), and Cummings Otolaryngology Head & Neck Surgery, which collectively cover all topics described in Shafer's oral pathology curriculum for MEC.
This is a shared conversation. Sign in to Orris to start your own chat.