Hypertension reason
Reading File
Finding Sources
Searching the Web
hypertension causes etiology pathophysiology
Searching PubMed
"hypertension"[MeSH Terms] AND "etiology"[MeSH Terms]
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Loading Image
Here is a thorough breakdown of the causes and mechanisms of hypertension, drawn from authoritative medical textbooks.
Causes of Hypertension
Hypertension (high blood pressure) is classified into two main types: primary (essential) and secondary.
1. Primary (Essential) Hypertension
This accounts for 90-95% of all adult cases. By definition, no single identifiable cause is found - it results from a combination of genetic, lifestyle, and physiological factors. - Comprehensive Clinical Nephrology, 7th Ed.
Initiating Factors and Pathogenesis
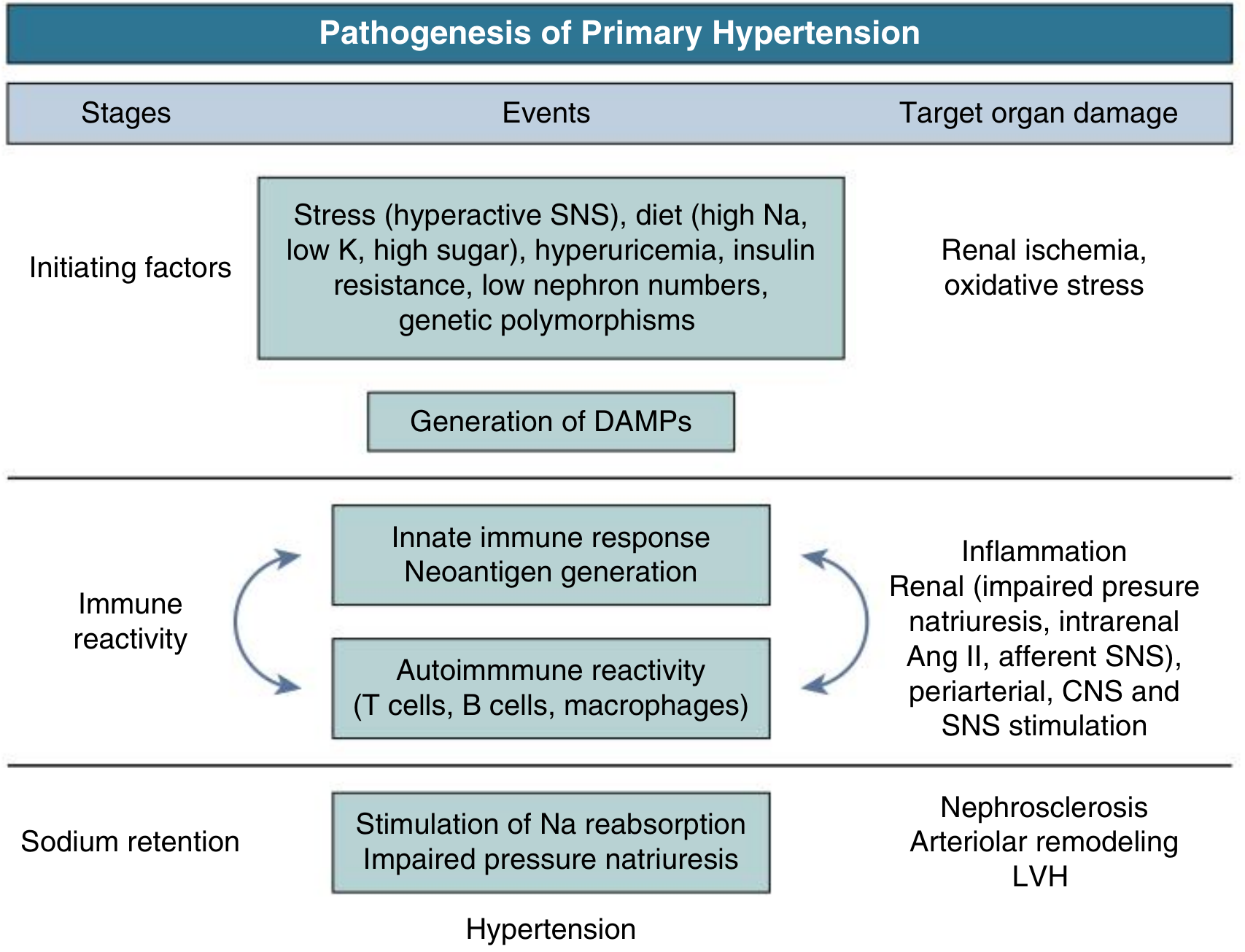
The pathogenesis involves three overlapping stages (Comprehensive Clinical Nephrology, 7th Ed.):
a) Initiating Factors
- High dietary sodium (salt), low potassium intake
- High sugar / fructose consumption
- Stress and sympathetic nervous system (SNS) overactivity
- Hyperuricemia
- Insulin resistance / obesity
- Low nephron number at birth (prematurity, low birth weight)
- Genetic polymorphisms
b) Immune Reactivity
Initiating factors cause renal ischemia and oxidative stress, generating damage-associated molecular patterns (DAMPs). This triggers an innate immune response - T cells, B cells, and macrophages create an autoimmune cycle that drives inflammation in the kidney, arteries, and CNS (stimulating SNS further).
c) Sodium Retention
The immune-driven renal inflammation leads to increased sodium reabsorption and impaired pressure-natriuresis. Sodium retention raises intravascular volume, which initially increases cardiac output. Over time, peripheral vascular resistance increases and cardiac output normalizes, but blood pressure remains elevated.
Key Contributing Mechanisms
| Mechanism | Role in Hypertension |
|---|---|
| Renin-Angiotensin-Aldosterone System (RAAS) | Angiotensin II causes vasoconstriction and stimulates aldosterone, leading to sodium/water retention and raised BP |
| Sympathetic Nervous System | Overactivity raises heart rate, cardiac output, and vascular tone |
| Salt/Sodium intake | Promotes fluid retention and raises intravascular volume |
| Obesity / Insulin resistance | Activates RAAS and SNS; promotes inflammation |
| Endothelial dysfunction | Reduced nitric oxide production impairs vasodilation |
| Genetics | Polygenic inheritance; family history significantly increases risk |
2. Secondary Hypertension
This accounts for 5-10% of cases and has a specific identifiable cause. It should be suspected when hypertension is resistant, presents at a young age, or has an abrupt onset. - Symptom to Diagnosis, 4th Ed.
Causes by System
Endocrine
- Primary hyperaldosteronism (Conn syndrome) - excess aldosterone causes sodium retention
- Pheochromocytoma - catecholamine-secreting tumor causing episodic or sustained BP elevation
- Cushing syndrome - excess cortisol promotes sodium retention and vascular effects
- Thyroid disease (hyperthyroidism raises cardiac output; hypothyroidism raises diastolic BP)
- Hyperparathyroidism - hypercalcemia affects vascular smooth muscle
Renal
- Chronic kidney disease (CKD) - impaired sodium excretion, RAAS activation
- Acute kidney injury - sudden impairment of pressure-natriuresis
Vascular
- Renovascular disease (renal artery stenosis) - activates RAAS via ischemic kidney; most common secondary cause in adults
- Coarctation of the aorta - mechanical obstruction causing upper-body hypertension
Other
- Obstructive sleep apnea - intermittent hypoxia activates SNS
- Obesity - multi-mechanistic (RAAS, SNS, insulin resistance)
- Ureteral or bladder outlet obstruction
Drug-Induced / Iatrogenic
- NSAIDs and COX-2 inhibitors
- Corticosteroids (prolonged use)
- Oral contraceptives (estrogen effect)
- Cocaine and amphetamines
- Sympathomimetics (decongestants, anorectics)
- Cyclosporine / tacrolimus
- Erythropoietin
- Alcohol
Key Risk Factors for Developing Hypertension
| Risk Factor | Notes |
|---|---|
| Family history | Strong genetic component |
| Age | Arteries stiffen with age, raising systolic BP |
| Obesity (BMI >30) | Most modifiable risk factor |
| High sodium diet | Promotes fluid retention |
| Physical inactivity | Contributes to obesity and vascular stiffness |
| Smoking | Raises BP acutely; damages arterial walls |
| Excessive alcohol | Dose-dependent BP elevation |
| Stress | Activates SNS chronically |
| African ancestry | Higher prevalence and severity |
| Prematurity / low birth weight | Fewer nephrons at birth |
In summary, hypertension is most often a multifactorial condition driven by genetics, lifestyle, RAAS activation, SNS overactivity, and renal sodium handling. Secondary causes - especially renal artery stenosis and primary hyperaldosteronism - should be ruled out in resistant or atypical cases. - Symptom to Diagnosis 4th Ed.; Comprehensive Clinical Nephrology 7th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.