Cardiomegaly
Reading File
Finding Sources
Finding Sources
Searching PubMed
cardiomegaly causes diagnosis management
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
I now have comprehensive material from multiple authoritative textbooks. Here is the full answer:
Cardiomegaly
Definition
Cardiomegaly refers to an enlarged heart, most commonly identified on chest radiography (CXR) as an increased cardiac silhouette. In adults, cardiomegaly is defined by a cardiothoracic (CT) ratio ≥ 0.5, measured by dividing the maximum transverse cardiac diameter by the maximum internal thoracic diameter on a PA CXR. A CT ratio > 0.6 generally indicates significant enlargement and carries prognostic weight (e.g., in Ebstein anomaly, CTR > 0.6 correlates with worse outcomes and higher risk of reoperation).
Important caveat: An enlarged cardiac silhouette on CXR does not always equal true cardiomegaly - pericardial effusion can mimic it and must be excluded.
- Frameworks for Internal Medicine
Pathophysiology: How the Heart Enlarges
The heart enlarges through two main mechanisms:
1. Eccentric Hypertrophy (Volume Overload)
- Chamber dilation with relative thinning of the ventricular wall
- Results in an increased chamber size - the "big and floppy" heart
- Seen in dilated cardiomyopathy, chronic volume overload (AR, MR), heart failure with reduced ejection fraction
- This is the pattern that produces cardiomegaly visible on CXR
2. Concentric Hypertrophy (Pressure Overload)
-
Wall thickens disproportionately, chamber size decreases
-
Typical of hypertension, aortic stenosis
-
May NOT cause cardiomegaly on CXR despite significant hypertrophy
-
Frameworks for Internal Medicine
Causes of Cardiomegaly
| Category | Examples |
|---|---|
| Myocardial | Dilated cardiomyopathy (ischemic, non-ischemic), previous MI with LV remodeling |
| Ischemic | Post-MI LV dilation, chronic ischemic heart disease |
| Hypertensive | Long-standing hypertension causing LV dilation |
| Valvular | Aortic regurgitation (chronic - gross cardiomegaly), mitral regurgitation, aortic stenosis (later stages) |
| Pericardial | Pericardial effusion (can mimic cardiomegaly) |
| High-output states | Hyperthyroidism, severe anemia, beriberi, arteriovenous shunts |
| Congenital | Ebstein anomaly (massive cardiomegaly), ASD (with right heart enlargement), coarctation of the aorta |
| Toxic/Metabolic | Alcoholic cardiomyopathy (~20-30% of nonischemic dilated CMP), tachycardia-mediated CMP |
| Rheumatologic | Myocarditis (in SLE, rheumatoid, other connective tissue disease) |
- Goldman-Cecil Medicine, Katzung Pharmacology, Fuster & Hurst's The Heart, Braunwald's Heart Disease
Radiographic Appearances
Acute vs. Chronic Heart Failure
-
Acute left-sided HF: Normal heart size + alveolar pulmonary edema (butterfly pattern). Cardiomegaly is typically absent because there is no time for cardiac remodeling.
-
Chronic left-sided HF: Gross cardiomegaly + striking cephalization of pulmonary vasculature + Kerley B lines + interstitial pulmonary edema or fibrosis.
-
Chronic right-sided HF: Cardiomegaly with right-sided chamber enlargement; pulmonary vascular changes depend on etiology.
-
Fuster & Hurst's The Heart, 15th Edition
Disease-Specific Patterns (from CXR)
| Condition | CXR Findings |
|---|---|
| Aortic stenosis | Mild cardiomegaly or LV prominence; aortic calcification |
| Aortic regurgitation (chronic) | Gross cardiomegaly; pulmonary edema, widened mediastinum |
| Ebstein anomaly | Massive globular cardiomegaly (CTR often >0.6); "box-shaped" heart; bulging right heart border |
| ASD | Cardiomegaly + increased vascular markings (right heart enlargement) |
| Coarctation of aorta | Cardiomegaly + pulmonary edema (neonates); rib notching (older children/adults) |
- Washington Manual of Medical Therapeutics, Fuster & Hurst's The Heart, Tintinalli's Emergency Medicine
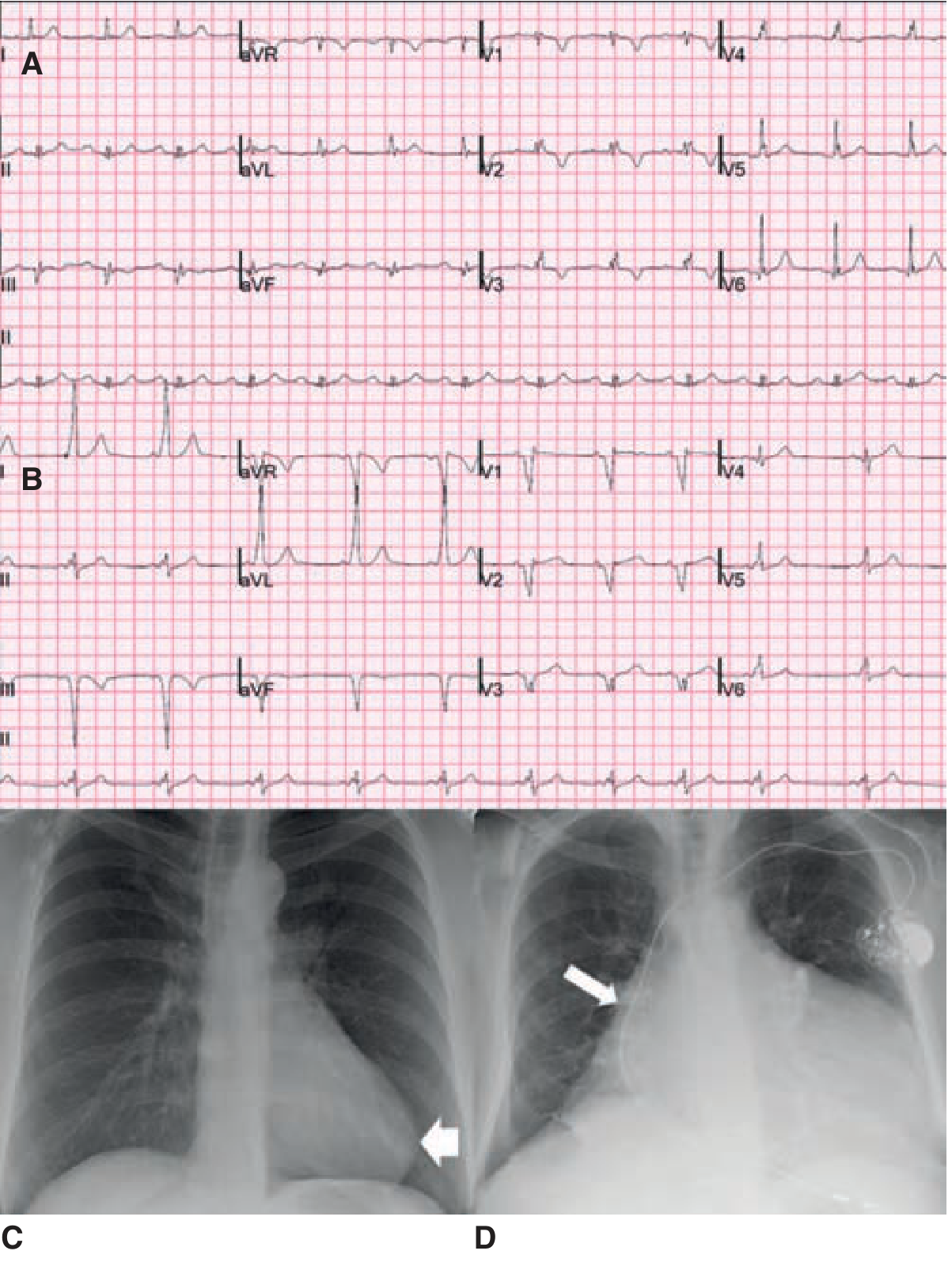
Below: ECGs and CXRs in Ebstein anomaly showing the spectrum from mild (C, CTR 0.49) to massive cardiomegaly (D, CTR 0.78):
Signs and Symptoms
Cardiomegaly itself is a radiographic/imaging finding, not a symptom, but the underlying cause typically produces:
- Symptoms: Dyspnea (exertional, then at rest), orthopnea, PND, fatigue, decreased exercise tolerance, peripheral edema
- Signs: Tachycardia, displaced apex beat (toward the axilla), S3 gallop (specific for systolic dysfunction), S4, murmurs of valvular disease, raised JVP, hepatomegaly, peripheral edema
- ECG changes: LVH, LAE, LBBB, ST-T changes depending on the cause
Primary signs and symptoms of heart failure include tachycardia, decreased exercise tolerance, shortness of breath, and cardiomegaly. - Katzung's Basic and Clinical Pharmacology, 16th Edition
Diagnostic Workup
- Chest X-ray - initial identification; CT ratio ≥ 0.5 = cardiomegaly
- ECG - LVH, conduction defects, arrhythmias, prior MI evidence
- Echocardiography - gold standard for assessing chamber size, wall motion, EF, valvular disease, pericardial effusion; differentiates dilated vs. hypertrophic vs. restrictive patterns
- BNP / NT-proBNP - elevated in heart failure, guides severity assessment
- Troponin - rules out acute ischemic cause
- Thyroid function, CBC, iron studies - screen for reversible/high-output causes
- Cardiac MRI - tissue characterization (fibrosis, infiltration, myocarditis), laminopathy evaluation
- Coronary angiography - if ischemic etiology suspected
- Tintinalli's Emergency Medicine, Goldman-Cecil Medicine
Management Principles
Management targets the underlying cause:
| Cause | Treatment |
|---|---|
| Systolic HF (HFrEF) | ACE inhibitors/ARBs, beta-blockers, MRAs, SGLT2 inhibitors, diuretics |
| Hypertension | Antihypertensive therapy |
| Valvular disease | Surgical/transcatheter repair or replacement |
| Alcoholic CMP | Abstinence (may be partially reversible) |
| Thyroid disease | Treat hyperthyroidism |
| Severe anemia | Treat underlying cause, transfusion if needed |
| Pericardial effusion | Pericardiocentesis |
| Congenital defects | Surgical/catheter-based repair |
"High-output" heart failure (hyperthyroidism, beriberi, AV shunts, severe anemia) responds poorly to conventional heart failure drugs and must be treated by correcting the underlying cause. - Katzung's Basic and Clinical Pharmacology, 16th Edition
Key Differentials for an Enlarged Cardiac Silhouette on CXR
- True cardiomegaly (from any cause above)
- Pericardial effusion - globular "water bottle" heart; no pulmonary vascular changes
- Pericardial fat pad - pseudo-enlargement
- AP film artifact - portable AP CXRs magnify the cardiac shadow; always compare with PA erect films
- Ebstein anomaly - massive RA/RV enlargement mimicking pericardial effusion globular shape
Summary
Cardiomegaly is a final common radiographic manifestation of many cardiac conditions. The most common causes are dilated cardiomyopathy (ischemic or non-ischemic), chronic valvular disease, and long-standing hypertension. Echocardiography is the key next step after CXR to define the structural cause. Management is directed at the specific etiology, with heart failure therapies forming the backbone when systolic dysfunction is present.
Congestive heart' failure
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching PubMed
"heart failure" management guidelines
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Reading File
Loading Image
I now have comprehensive, authoritative content from Robbins Pathology, Katzung Pharmacology, Goldman-Cecil Medicine, and Braunwald's Heart Disease. Here is the full, synthesized answer:
Congestive Heart Failure (CHF)
Definition
Heart failure occurs when the heart is unable to provide adequate perfusion to meet the metabolic requirements of peripheral tissues. Inadequate cardiac output is usually accompanied by increased congestion of the venous circulation - hence the term "congestive" heart failure. Normal cardiac output is approximately 5 L/min/70 kg body weight.
- Robbins, Cotran & Kumar Pathologic Basis of Disease; Katzung's Basic and Clinical Pharmacology, 16th Edition
Etiology and Causes
| Category | Examples |
|---|---|
| Ischemic heart disease | MI (most common cause globally), chronic ischemic CMP |
| Hypertension | Long-standing systemic hypertension (pressure overload) |
| Valvular disease | Aortic stenosis/regurgitation, mitral regurgitation/stenosis |
| Primary myocardial disease | Dilated cardiomyopathy (idiopathic, alcoholic, viral, familial) |
| Tachyarrhythmia | Atrial fibrillation with rapid rate (tachycardia-mediated CMP) |
| High-output states | Hyperthyroidism, severe anemia, beriberi, AV shunts |
| Infiltrative | Amyloidosis, sarcoidosis, hemochromatosis |
| Toxic | Alcohol, anthracyclines, cobalt, cocaine |
| Congenital | Large shunts (ASD, VSD), Ebstein anomaly |
| Pericardial disease | Constrictive pericarditis (mimics CHF) |
Pathophysiology
The Core Problem
Increased mechanical work on either ventricle (from pressure or volume overload) triggers a cascade:
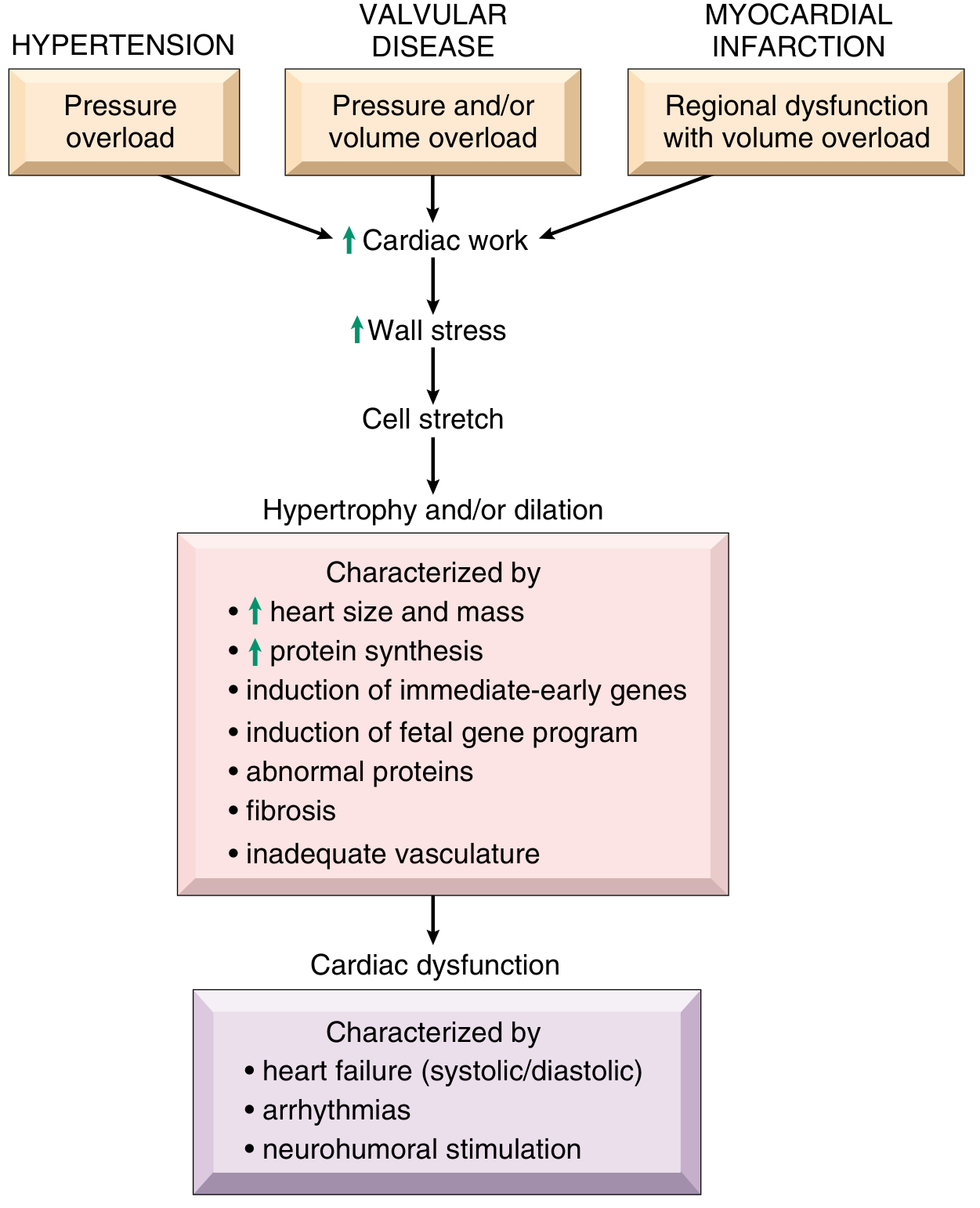
-
Pressure overload (e.g., hypertension, aortic stenosis): new sarcomeres assemble in parallel → concentric hypertrophy → wall thickens, chamber shrinks
-
Volume overload (e.g., aortic/mitral regurgitation): new sarcomeres assemble in series → eccentric hypertrophy → chamber dilates, wall may thin
-
Patients with hypertension, IHD, aortic stenosis, MR, or dilated CMP frequently have heart weights double or triple the average.
-
Robbins, Cotran & Kumar Pathologic Basis of Disease
Molecular Changes in the Failing Heart
Initially beneficial hypertrophy becomes harmful over time:
-
Immediate-early genes (FOS, JUN, MYC) are induced
-
Fetal gene program is re-expressed (fetal myosin isoforms, natriuretic peptides, collagen)
-
Capillary density does NOT increase proportionally to muscle mass → relative ischemia
-
Mitochondrial dysfunction → impaired energy production
-
Calcium handling is disrupted (SERCA impaired, RyR channels leak Ca²⁺ → arrhythmias)
-
Accelerated myocyte apoptosis → progressive loss of contractile mass
-
The result: cardiac remodeling - progressive dilation, fibrosis, and dysfunction
-
Katzung's Basic and Clinical Pharmacology, 16th Edition; Robbins Pathology
Neurohumoral Compensation (the Vicious Cycle)
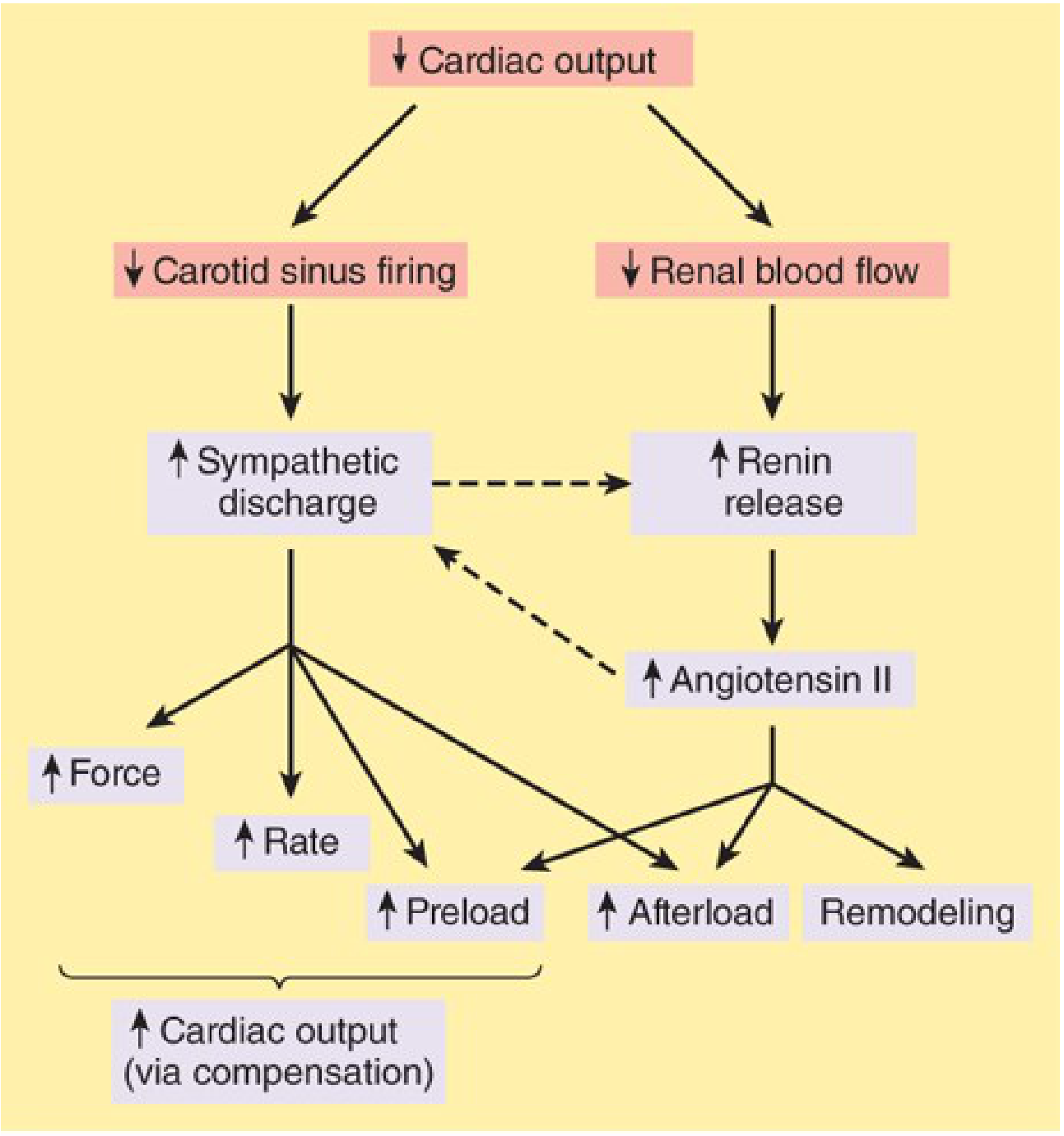
Low cardiac output triggers two major compensatory axes:
-
Sympathetic nervous system: Baroreceptors are reset; sympathetic outflow increases → tachycardia, increased contractility, vasoconstriction. Chronically, norepinephrine promotes myocyte hypertrophy and apoptosis.
-
RAAS: Reduced renal perfusion → renin release → angiotensin II → aldosterone → sodium and water retention → increased preload and afterload. Angiotensin II also promotes remodeling and vasoconstriction.
Both mechanisms initially compensate but ultimately worsen cardiac function through increased afterload and remodeling - creating the classic vicious cycle of progressive heart failure.
- Katzung's Basic and Clinical Pharmacology, 16th Edition
Types of CHF
1. HFrEF (Heart Failure with Reduced Ejection Fraction)
- EF < 40-45%; also called "systolic failure" or "pump failure"
- The heart is big and floppy (eccentric hypertrophy/dilation)
- Responds to positive inotropes, neurohormonal blockers
- Most common after MI, in dilated CMP
2. HFpEF (Heart Failure with Preserved Ejection Fraction)
- EF ≥ 50%; also called "diastolic failure"
- LV is stiff and cannot relax - filling is impaired
- Any increase in filling pressure is immediately transmitted back to the lungs → pulmonary edema
- Most common in elderly, hypertensives, diabetics, obese patients
- Does NOT respond well to positive inotropes
- Also associated with myocardial fibrosis (IHD, cardiomyopathies) and infiltrative disease (amyloidosis)
3. Left-Sided vs. Right-Sided vs. Biventricular
Left-sided failure → back-pressure into pulmonary circulation:
- Pulmonary congestion, edema, dyspnea, orthopnea, PND
- "Heart failure cells" (hemosiderin-laden macrophages) in alveoli - a pathological hallmark
- Pulmonary rales, S3/S4, displaced apex, cardiomegaly
Right-sided failure → back-pressure into systemic circulation:
- Peripheral edema (feet, ankles, presacral)
- Hepatomegaly ("nutmeg liver" - centrilobular congestion), congestive splenomegaly
- Ascites, pleural effusions
- Raised JVP, with or without pulsatile liver
- In severe/chronic cases: cardiac cirrhosis
Biventricular / Global CHF: Most chronic CHF patients develop this; left-sided failure commonly causes right-sided failure by increasing pulmonary pressure, increasing RV afterload.
- Robbins, Cotran & Kumar Pathologic Basis of Disease
4. High-Output Failure
- Cardiac output is increased (>8-10 L/min), yet still insufficient for the body's demands
- Causes: hyperthyroidism, severe anemia, beriberi, AV shunts
- Responds poorly to standard HF drugs; treat the underlying cause
Clinical Features
Symptoms
| Left Heart Failure | Right Heart Failure |
|---|---|
| Dyspnea on exertion (earliest) | Peripheral edema |
| Orthopnea | Abdominal distension (ascites) |
| Paroxysmal nocturnal dyspnea (PND) | Right upper quadrant discomfort (hepatomegaly) |
| Cough (frothy, sometimes pink) | Anorexia, nausea (gut edema) |
| Fatigue, reduced exercise tolerance | Weight gain (fluid retention) |
In advanced CHF:
- Prerenal azotemia (reduced renal perfusion)
- Cerebral hypoperfusion: confusion, irritability, stupor, coma
- Cardiac cachexia (chronic severe CHF)
Signs
-
Tachycardia - earliest compensatory sign
-
S3 gallop - early diastolic sound; indicates volume overload and systolic dysfunction (high specificity)
-
S4 gallop - increased myocardial stiffness (diastolic dysfunction)
-
Displaced apex beat toward the axilla (eccentric hypertrophy)
-
Cardiomegaly on CXR
-
Bilateral basal crepitations/rales - alveolar fluid
-
Raised JVP
-
Pitting edema (dependent)
-
Hepatojugular reflux
-
Mitral regurgitation murmur (functional - from papillary muscle displacement due to LV dilation)
-
Pleural effusion (particularly right-sided)
-
Robbins, Cotran & Kumar Pathologic Basis of Disease
NYHA Functional Classification
| Class | Description |
|---|---|
| I | No symptoms with ordinary activity |
| II | Slight limitation; comfortable at rest, symptoms with moderate exertion |
| III | Marked limitation; comfortable at rest, symptoms with minimal exertion |
| IV | Symptoms at rest or with any activity |
ACC/AHA Staging (A-D)
| Stage | Description |
|---|---|
| A | High risk, no structural disease, no symptoms |
| B | Structural disease, no symptoms |
| C | Structural disease with current or prior symptoms |
| D | Refractory heart failure requiring advanced interventions |
Investigations
| Test | Findings / Purpose |
|---|---|
| CXR | Cardiomegaly (CTR ≥0.5), cephalization, Kerley B lines, pulmonary edema, pleural effusion |
| ECG | LVH, LBBB, Q waves, arrhythmias (AF is present in 10-50% depending on NYHA class) |
| Echocardiogram | EF, chamber dimensions, wall motion, valve function, pericardial effusion; KEY investigation |
| BNP / NT-proBNP | Elevated with ventricular wall stress; high negative predictive value when low |
| Troponin | Rules out acute ischemic cause; mildly elevated in decompensated CHF |
| U&E, creatinine | Baseline renal function; monitor for cardiorenal syndrome |
| FBC | Anemia (aggravates CHF) |
| TFTs | Hypo-/hyperthyroidism as cause or aggravator |
| Iron studies | Hemochromatosis; iron deficiency (treat even without anemia in CHF) |
| Cardiac MRI | Tissue characterization, fibrosis mapping, myocarditis, infiltrative disease |
Management
General Principles
Treatment first corrects any reversible underlying cause (valvular disease, ischemia, arrhythmia, thyroid disease), then targets the neurohumoral dysregulation driving progression.
Non-Pharmacological
- Salt restriction (evidence supports modest restriction in chronic CHF; recent meta-analysis 2024 - PMID 37389661)
- Fluid restriction in hyponatremia or severe CHF
- Daily weight monitoring (alert if >2 kg in 2 days)
- Aerobic exercise rehabilitation (improves symptoms and quality of life)
- Smoking cessation, alcohol abstinence (alcoholic CMP may partially reverse)
- Treat sleep apnea (CPAP reduces symptoms)
- Vaccination (influenza, pneumococcal)
Pharmacotherapy for HFrEF - the "Fantastic Four"
Current guidelines recommend four pillars of disease-modifying therapy for HFrEF (EF <40%):
| Drug Class | Examples | Key Benefits |
|---|---|---|
| ARNI (preferred) or ACE inhibitor / ARB | Sacubitril/valsartan (ARNI); enalapril, ramipril (ACE-i); losartan, candesartan (ARB) | Reduces afterload, blocks angiotensin II, prevents remodeling, ↓ mortality |
| Beta-blocker | Carvedilol, bisoprolol, metoprolol succinate | ↓ HR, ↓ catecholamine toxicity, ↑ EF, ↓ mortality by ~27-34% in sinus rhythm |
| Mineralocorticoid receptor antagonist (MRA) | Spironolactone, eplerenone | Blocks aldosterone → ↓ Na/water retention, ↓ fibrosis, ↓ mortality |
| SGLT2 inhibitor | Dapagliflozin, empagliflozin | Osmotic diuresis, metabolic effects, cardioprotection; ↓ hospitalizations and mortality |
The combination of a beta-blocker with an ARNI (or ACE inhibitor/ARB) is a cornerstone of treatment of symptomatic heart failure. Treatment should be started at low dose ("start low, go slow") and up-titrated toward trial-proven target doses.
- Goldman-Cecil Medicine
Diuretics (not disease-modifying but essential for symptom relief):
- Loop diuretics (furosemide, torasemide) for most patients
- Thiazides can be added in combination for diuretic resistance (sequential nephron blockade)
- IV diuretics if oral absorption impaired by gut edema
Digoxin: Reduces hospitalizations, rate control in AF with HFrEF, does not reduce mortality
Device Therapy
| Device | Indication |
|---|---|
| ICD (Implantable Cardioverter-Defibrillator) | EF ≤35% on optimal medical therapy (primary prevention of sudden cardiac death) |
| CRT (Cardiac Resynchronization Therapy) | EF ≤35% + LBBB + QRS ≥130 ms + NYHA II-IV symptoms; improves EF and symptoms |
| CRT-D | When EF ≤30-35% and unlikely to recover; provides both CRT and ICD benefit |
| LVAD (Left Ventricular Assist Device) | Bridge to transplant or destination therapy in stage D HF |
Atrial fibrillation management in CHF:
- Rate control: beta-blockers preferred in HFrEF; non-dihydropyridine CCBs in HFpEF
- Rhythm control: amiodarone and dofetilide are the only antiarrhythmics safe in HF
- AF catheter ablation in HF patients: associated with greater improvement in LVEF, quality of life, and reduced mortality (CASTLE-AF trial)
- AV node ablation + biventricular pacing when rate cannot be controlled
- Braunwald's Heart Disease, 2 Vol Set
Advanced/End-Stage HF (Stage D)
- Cardiac transplantation (gold standard for eligible patients)
- LVAD as destination therapy
- Ultrafiltration for refractory volume overload
- Palliative care
Key Pathological Findings
| Location | Finding in CHF |
|---|---|
| Lungs | Pulmonary edema, "heart failure cells" (hemosiderin-laden macrophages) |
| Liver | "Nutmeg liver" (centrilobular congestion), cardiac cirrhosis (chronic) |
| Spleen | Congestive splenomegaly with platelet sequestration |
| Kidneys | Increased congestion in right HF; prerenal azotemia |
| Periphery | Pitting edema, sacral edema in bedridden patients, anasarca (severe) |
| Pleura/Peritoneum | Transudative pleural effusions, ascites |
- Robbins, Cotran & Kumar Pathologic Basis of Disease
Prognosis
CHF remains a serious cause of morbidity and mortality despite modern therapy. The annual mortality in severe (NYHA class IV) heart failure exceeds 50%. Key prognostic factors include:
- LVEF
- NYHA functional class
- BNP/NT-proBNP levels
- Serum sodium (hyponatremia = poor prognosis)
- Heart rate in sinus rhythm (higher HR = worse outcome)
- Comorbidities (renal dysfunction, diabetes, COPD)
Summary
CHF is the common final pathway of most cardiac diseases. It is driven by a self-amplifying neurohumoral spiral (SNS + RAAS activation) that initially compensates but ultimately accelerates myocardial deterioration through remodeling, apoptosis, and arrhythmogenesis. Modern treatment - combining ARNI/ACE-i, beta-blocker, MRA, and SGLT2 inhibitor - targets each arm of this spiral and has dramatically improved outcomes over the past three decades.
Dv t
Reading File
Finding Sources
Finding Sources
Searching PubMed
"deep vein thrombosis" diagnosis treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the material needed for a comprehensive, well-illustrated answer. Here it is:
Deep Vein Thrombosis (DVT)
Definition
Deep vein thrombosis is the formation of a thrombus within the deep venous system, most commonly in the lower extremity. It is part of the spectrum of venous thromboembolism (VTE), which also includes pulmonary embolism (PE) - the most feared complication, which may be fatal. VTE causes more than 50,000 deaths per year in the United States, with ~25% occurring in the perioperative period.
- Sabiston Textbook of Surgery
Relevant Anatomy
The deep venous system of the lower extremity (the usual site of DVT):
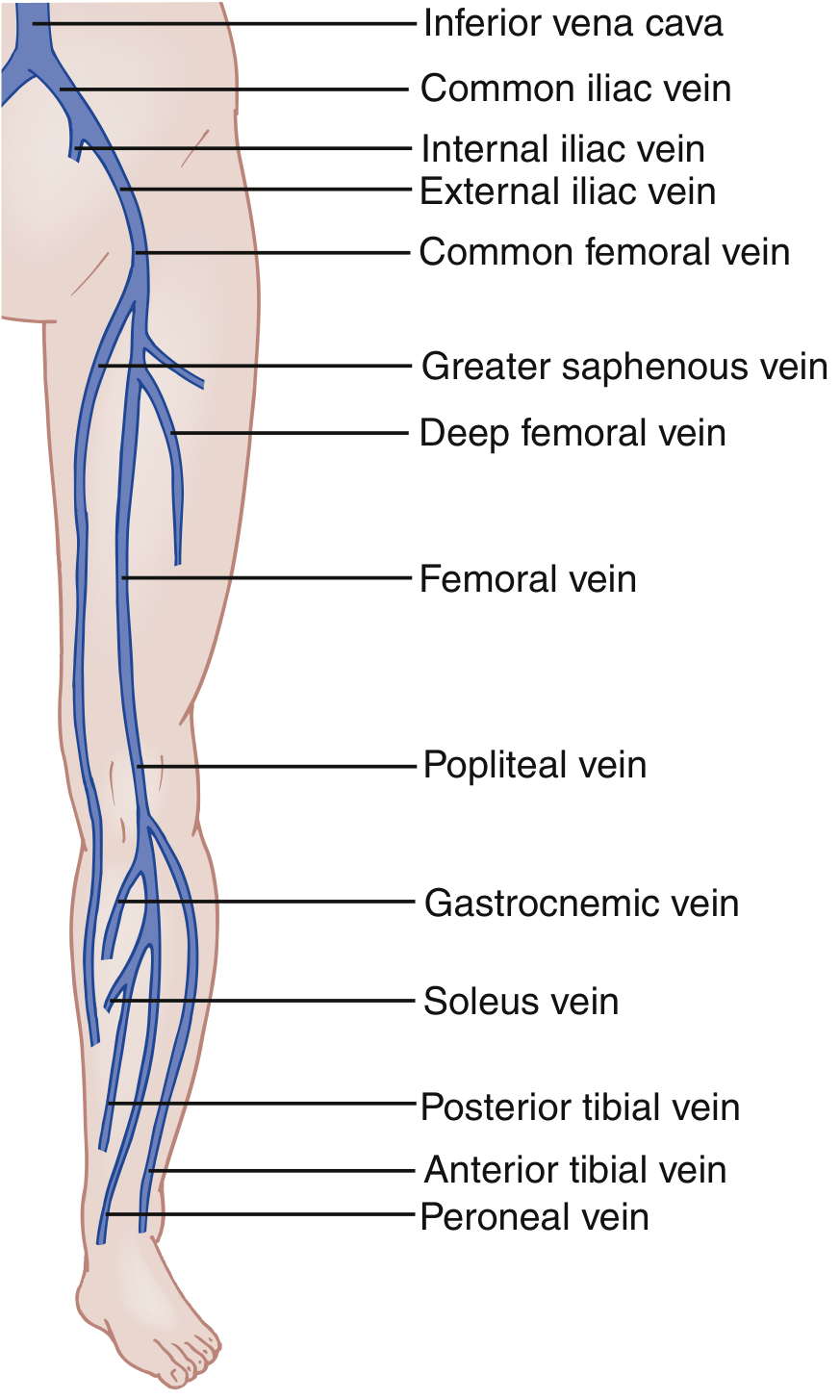
Key veins involved (proximal to distal): common femoral → femoral → popliteal → posterior tibial / peroneal / anterior tibial → calf (gastrocnemius, soleus)
- Proximal DVT: involves popliteal vein or above - higher risk of PE
- Distal DVT: isolated calf vein involvement - lower PE risk; may propagate proximally if untreated
- Iliac/pelvic DVT: requires CT venography or MRI to diagnose (not seen on standard duplex US)
Note: DVT occurs with slightly higher frequency on the left leg because the left iliac vein is vulnerable to compression by the left iliac artery - May-Thurner syndrome.
- Rosen's Emergency Medicine
Pathophysiology - Virchow's Triad
Rudolf Virchow (1856) described three factors that predispose to venous thrombosis - collectively known as Virchow's Triad:
| Component | Mechanism | Examples |
|---|---|---|
| 1. Venous stasis | Reduced flow creates hypoxia; downregulates antithrombotic proteins (thrombomodulin, endothelial protein C receptor); allows clotting factors to accumulate | Immobility, long-haul travel, paralysis, CHF, obesity, pregnancy (uterine compression) |
| 2. Endothelial injury | Exposes subendothelial tissue factor (TF); activates coagulation cascade; hypoxia + cytokines induce TF expression and P-selectin on intact endothelium | Surgery, trauma, IV catheters, vasculitis |
| 3. Hypercoagulability | Hereditary or acquired procoagulant state; impaired fibrinolysis | Factor V Leiden, antiphospholipid syndrome, malignancy, OCP use, pregnancy |
The molecular cascade once initiated: TF:FVIIa → thrombin generation → platelet activation → polyphosphate release + neutrophil extracellular traps (NETs) → intrinsic pathway activation via FXI → propagating procoagulant environment.
- Sabiston Textbook of Surgery; Gray's Anatomy for Students
Risk Factors
Acquired Risk Factors
- Immobility: prolonged bed rest (≥3 days), long-haul travel, plaster cast, paralysis
- Surgery: particularly high-risk - pelvic surgery, total hip/knee replacement, major abdominal surgery
- Malignancy: especially pancreatic, lung, ovarian, GI cancers (Trousseau's syndrome)
- Pregnancy & postpartum: compression of iliac veins by gravid uterus + hypercoagulable state
- Combined oral contraceptive pill / HRT
- Prior DVT / PE
- Obesity
- Age > 60
- Heart failure, nephrotic syndrome, dehydration
- Indwelling venous catheters (>90% of upper extremity DVTs occur in the presence of a catheter/device)
- Antiphospholipid antibody syndrome
Inherited Thrombophilias
| Thrombophilia | Mechanism | Notes |
|---|---|---|
| Factor V Leiden | Arg506Gln mutation → resistance to activated Protein C | Most common inherited thrombophilia in White populations (heterozygote prevalence ~4.7%); RR 6-8x |
| Prothrombin gene mutation (G20210A) | Gly→Ala at position 20210 → increased thrombin synthesis | Second most common |
| Protein C deficiency | Reduced natural anticoagulant; cannot inactivate FVa and FVIIIa | Autosomal dominant |
| Protein S deficiency | Cofactor for Protein C; disrupted interaction with APC and TFPI | Levels lower in females, pregnancy, OCP use |
| Antithrombin deficiency | Cannot clear thrombin and FXa | SERPINA1 mutation |
- Sabiston Textbook of Surgery
Surgical Risk Stratification
| Risk Level | Procedures |
|---|---|
| Low | Maxillofacial, neurosurgery, cardiothoracic surgery |
| Medium | Inguinal hernia repair, abdominal, gynaecological, urological surgery |
| High | Pelvic surgery (elective and trauma), total hip and knee replacement |
- Bailey and Love's Short Practice of Surgery
Clinical Features
Symptoms
- Unilateral leg swelling (hallmark)
- Calf pain or aching - may be only mild cramping or a "sense of fullness"
- Redness and warmth of the affected limb
- Engorged superficial (collateral) veins
- Rarely: a palpable venous cord
Key point: Most DVTs show NO physical signs. Clinical examination alone is unreliable.
Signs
- Pitting edema of the affected limb
- Erythema and warmth
- Tenderness along the course of the deep venous system
- Homans' sign (calf pain on dorsiflexion of the foot) - historically described but neither sensitive nor specific; do not rely on it
Special Scenarios
-
Upper extremity DVT: Arm pain/swelling ipsilateral to an IV catheter or pacemaker wire. In young athletes without a device: Paget-Schroetter syndrome (effort-induced thrombosis from thoracic outlet compression, dominant arm)
-
Bilateral DVT: Less than 10% of ED-diagnosed DVT cases
-
Pregnancy: Left leg more commonly affected (gravid uterus compresses left external iliac vein)
-
Rosen's Emergency Medicine; Bailey and Love's Surgery
Differential Diagnosis
| Diagnosis | Distinguishing Feature |
|---|---|
| Cellulitis | Fever, no deep tenderness; DVT concurrent in only ~3% |
| Ruptured Baker cyst | Often has prior knee effusion; sudden onset calf swelling |
| Gastrocnemius muscle tear / Achilles injury | History of exertion/trauma |
| Superficial thrombophlebitis | Palpable, tender, indurated superficial cord; overlying skin erythema |
| Venous insufficiency | Bilateral, chronic; varicosities |
| Asymmetric edema from CHF, liver disease | Bilateral in most cases; no deep tenderness |
| Hematoma (spontaneous calf) | Coagulopathy history, no systemic features |
Diagnosis
Step 1 - Pretest Probability: Wells DVT Score
| Clinical Feature | Score |
|---|---|
| Active cancer (treatment in last 6 months or palliative) | +1 |
| Paralysis, paresis, or recent plaster immobilization of lower limbs | +1 |
| Bedridden ≥3 days or major surgery within 12 weeks (general/regional anesthesia) | +1 |
| Localized tenderness along the deep venous system | +1 |
| Entire leg swollen | +1 |
| Calf swelling ≥3 cm larger than asymptomatic side (measured 10 cm below tibial tuberosity) | +1 |
| Pitting edema confined to symptomatic leg | +1 |
| Collateral superficial veins (non-varicose) | +1 |
| Previously documented DVT | +1 |
| Alternative diagnosis at least as likely as DVT | -2 |
Score < 2 = Low PTP | Score ≥ 2 = High PTP
Step 2 - Diagnostic Algorithm
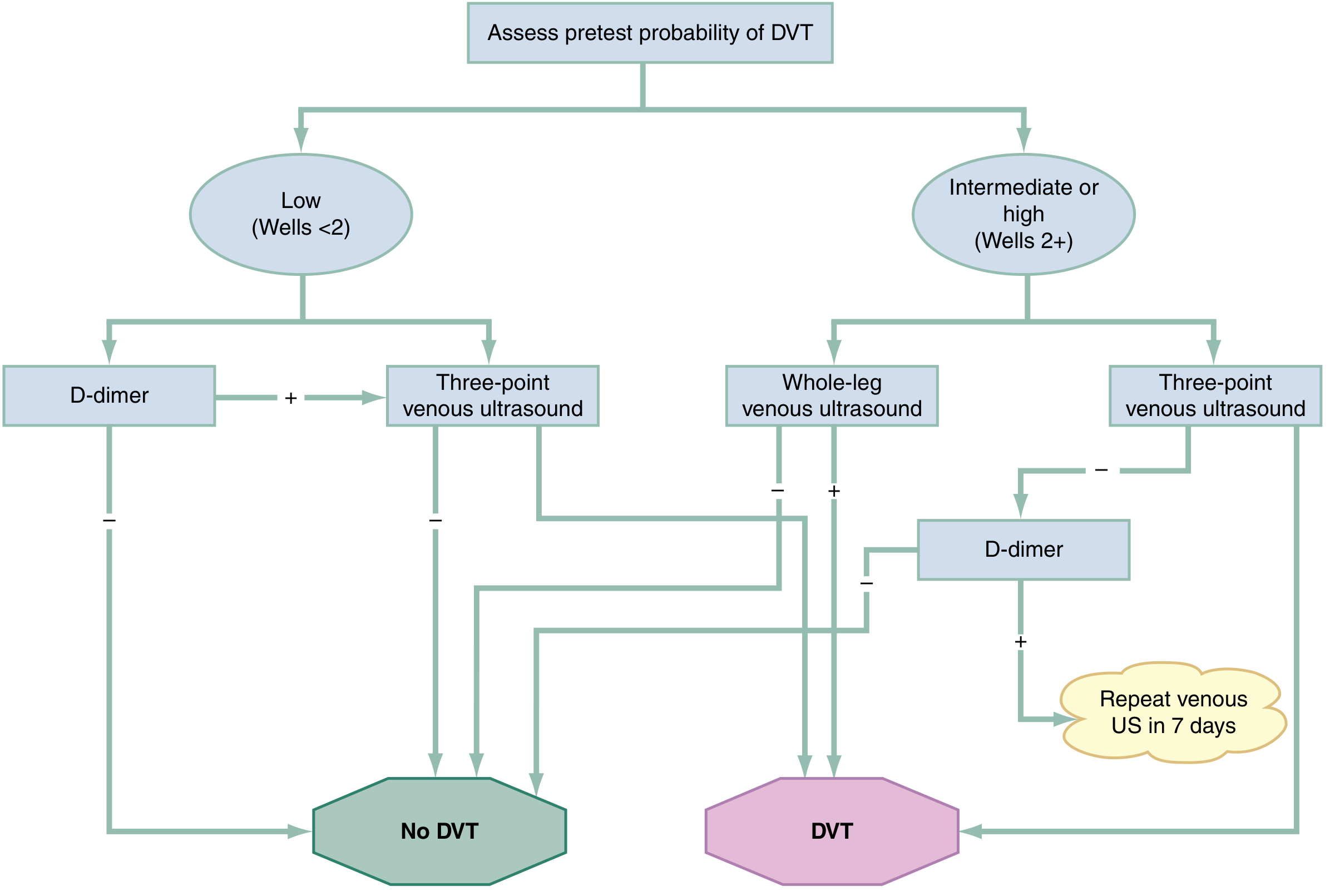
D-Dimer
- Measures enzymatic breakdown of cross-linked fibrin from any intravascular thrombus
- Standard cutoff: >500 ng/mL = positive
- Age-adjusted cutoff: Age × 10 ng/mL (e.g., for an 80-year-old, cutoff = 800 ng/mL) - safely increases percentage of patients who can avoid US
- Sensitivity ~92%, Specificity ~45% for DVT in low PTP patients
- False positives in: pregnancy, malignancy, recent surgery, trauma, infection, inflammation, liver disease, renal failure
- Note: warfarin use is associated with false-negative D-dimer results
Venous Ultrasound (Duplex)
- Gold standard investigation; non-invasive, no radiation
- Criteria for DVT on US: non-compressibility of the vein, absence of flow, absent respiratory variation, no augmentation on calf compression
- Whole-leg US (criterion standard): images all deep and superficial veins; 3-month VTE event rate 0.5% after negative result
- Three-point (compression) US: common femoral, femoral, popliteal veins; sensitivity 95%, specificity 95% for proximal DVT
- POCUS (bedside): 90-95% accurate in trained hands for proximal veins
Imaging Limitations
-
US cannot evaluate iliac veins or IVC - CT venography or MRI required for suspected pelvic/iliac DVT
-
MRI preferred in pregnant patients (no ionizing radiation)
-
Rosen's Emergency Medicine
Complications
Pulmonary Embolism (PE)
The most serious complication. Thrombus dislodges from the leading edge of the DVT, passes through the right heart, and lodges in the pulmonary arterial tree. Symptoms range from pleuritic chest pain (small emboli) to haemodynamic collapse and death (massive PE).
Post-Thrombotic Syndrome (PTS)
- Chronic venous insufficiency, persistent leg swelling, pain, skin changes, venous ulceration
- Occurs in 20-50% of DVT patients over time
- Caused by valvular incompetence from thrombus damage
Phlegmasia Cerulea Dolens
- Massive iliofemoral DVT causing complete venous outflow obstruction
- Limb becomes cyanotic, intensely swollen, and extremely painful
- Risk of venous gangrene without urgent intervention
Treatment
Anticoagulation Options
| Anticoagulant | Initial Dose | Key Restriction |
|---|---|---|
| Unfractionated heparin (UFH) | 70-80 U/kg IV bolus then 17-18 U/kg/h | HIT; use when rapid reversibility needed |
| Enoxaparin (LMWH) | 1 mg/kg q12h or 1.5 mg/kg q24h SC | CrCl < 30 mL/min |
| Dalteparin (LMWH) | 200 U/kg daily SC | CrCl < 30 mL/min |
| Fondaparinux | 5-10 mg SC daily | CrCl < 30 mL/min; use in HIT |
| Rivaroxaban (DOAC) | 15 mg BD × 21 days, then 20 mg OD | CrCl < 30; no bridging needed |
| Apixaban (DOAC) | 10 mg BD × 7 days, then 5 mg BD | CrCl < 30; no bridging needed |
| Dabigatran (DOAC) | After 5-10 days of LMWH | Requires initial parenteral lead-in |
| Warfarin | Bridged with LMWH until INR 2-3 for 2 consecutive days | Interactions, INR monitoring; less favoured now |
DOACs (rivaroxaban, apixaban) are now first-choice for most patients with DVT - equally effective as warfarin for preventing recurrent VTE, with fewer major bleeding events, and no need for INR monitoring or bridging with LMWH.
DOAC contraindications/cautions: pregnancy, severe renal failure (CrCl < 30), liver failure, antiphospholipid antibody syndrome, high-risk PE.
Cancer-associated thrombosis: LMWH traditionally preferred for lower VTE recurrence risk, but recent evidence suggests DOACs are also safe and effective - meta-analysis 2025, PMID 40578592.
Isolated distal (calf) DVT: Whether to anticoagulate remains controversial. A recent 2025 meta-analysis (PMID 40400471) evaluated anticoagulant treatment for isolated distal DVT; serial surveillance US is an acceptable alternative in low-risk patients without symptoms or propagation risk.
Duration of Anticoagulation
| Scenario | Duration |
|---|---|
| First DVT, provoked (reversible risk factor) | 3 months minimum |
| First DVT, unprovoked | 3-6 months; consider indefinite if low bleed risk |
| Recurrent DVT | Indefinite anticoagulation |
| Active cancer | Indefinite (or until cancer resolved) |
| Antiphospholipid syndrome | Indefinite |
Reversal Agents
| Drug | Reversal Agent |
|---|---|
| Heparin / LMWH | Protamine sulfate |
| Warfarin | FFP, 4-factor PCC, Vitamin K |
| Dabigatran | Idarucizumab |
| Rivaroxaban / Apixaban | Andexanet alfa |
IVC Filter
- For patients who cannot be safely anticoagulated (e.g., active bleeding, recent intracranial surgery)
- Temporary/retrievable filters preferred
- Reduces PE risk but does NOT treat DVT; retrieve when anticoagulation becomes safe
Endovascular Intervention (Catheter-Directed Thrombolysis / Thrombectomy)
-
Increasingly used in acute iliofemoral DVT (proximal, large-burden thrombosis)
-
Goals: restore patency, reduce post-thrombotic syndrome risk
-
Techniques: pharmacomechanical thrombolysis, aspiration thrombectomy, venous stenting
-
Best evidence in selected patients with acute proximal iliofemoral DVT and low bleed risk
-
Bailey and Love's Short Practice of Surgery; Rosen's Emergency Medicine
Prophylaxis
All hospitalised patients must be risk-assessed within 24 hours of admission for VTE risk.
| Method | Notes |
|---|---|
| Graduated compression stockings | Avoid in: PAD, neuropathy, severe leg oedema, skin breakdown, leg deformity, allergy |
| Intermittent pneumatic compression (calf pumps) | For patients at high DVT risk who cannot have anticoagulation |
| LMWH (e.g., enoxaparin 40 mg SC OD) | Mainstay of pharmacological prophylaxis in surgical/medical patients |
| Unfractionated heparin | Alternative if renal impairment |
| Fondaparinux | Option in HIT; good for orthopaedic prophylaxis |
Risk should be reviewed if the patient's clinical condition changes.
- Bailey and Love's Short Practice of Surgery
Summary
DVT is a common, potentially life-threatening condition driven by Virchow's triad (stasis, endothelial injury, hypercoagulability). Diagnosis requires systematic pretest probability assessment (Wells score), followed by D-dimer and/or venous duplex ultrasound. DOACs (rivaroxaban, apixaban) are now first-line treatment, offering equal efficacy to warfarin with a better safety profile and simpler dosing. Duration depends on provoked vs unprovoked DVT, with unprovoked and recurrent DVT warranting longer or indefinite anticoagulation. Prevention through VTE risk assessment and prophylaxis in all surgical and hospitalised patients remains the most effective strategy.
This is a shared conversation. Sign in to Orris to start your own chat.