Explain me about regulation of ph of acid and base
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Reading File
I now have comprehensive information from the textbooks to give a thorough answer. Let me compile it.
Regulation of pH: Acid-Base Balance
1. What is pH and Why It Matters
pH is defined as the negative logarithm of hydrogen ion (H⁺) activity:
pH = −log₁₀[H⁺]
Normal arterial blood pH is 7.35–7.45 (average 7.40), corresponding to [H⁺] of ~40 nmol/L.
| Condition | pH |
|---|---|
| Acidemia | < 7.35 |
| Normal | 7.35–7.45 |
| Alkalemia | > 7.45 |
| Death (severe) | < 6.8 or > 7.8 |
Even tiny pH changes matter because most biologically important molecules (enzymes, receptors, ion channels, transporters) contain chemical groups that donate or accept H⁺. For example, phosphofructokinase activity falls ~90% with a pH drop of just 0.1; cell proliferation may fall 85% when intracellular pH drops by 0.4.
— Medical Physiology (Boron & Boulpaep)
2. The Three Lines of Defense
The body uses three interrelated systems to maintain pH:
1. Chemical Buffers (seconds)
2. Respiratory System (minutes)
3. Renal System (hours to days)
3. Chemical Buffer Systems
A buffer is any substance that reversibly consumes or releases H⁺, minimizing (not preventing) pH changes. Buffers work best within ±1 pH unit of their pKa.
A. Bicarbonate/Carbonic Acid Buffer (most important in plasma)
H⁺ + HCO₃⁻ ⇌ H₂CO₃ ⇌ CO₂ + H₂O
- pKa = 6.1 (seemingly far from plasma pH of 7.4)
- Despite the mismatch, it is the most effective buffer because:
- CO₂ is continuously exhaled by the lungs (open system)
- HCO₃⁻ is reclaimed/excreted by the kidneys
- It is present at relatively high concentrations
Normal plasma ratio: HCO₃⁻ / dissolved CO₂ = 20:1
This is described by the Henderson-Hasselbalch equation:
pH = pKa + log([HCO₃⁻] / [dissolved CO₂]) pH = 6.1 + log(25/1.25) = 6.1 + log(20) = 7.4
Buffer value (β) of bicarbonate in plasma = 55.6 mmol/L
The balance diagram below illustrates how changes in this ratio shift pH:
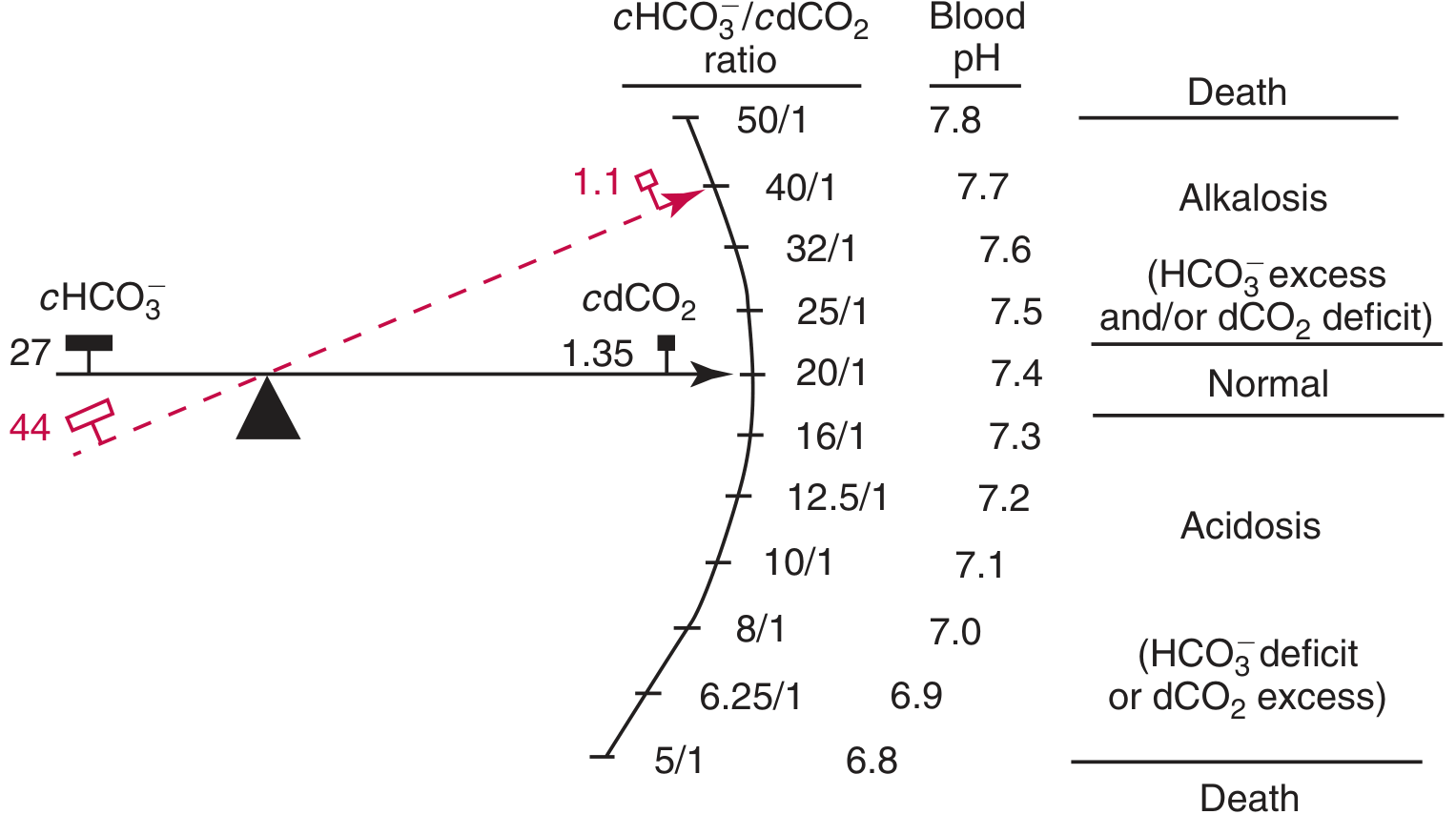
The teeter-totter: when HCO₃⁻/dCO₂ = 20:1 → pH 7.4 (normal). If the ratio rises → alkalosis; if it falls → acidosis. — Tietz Textbook of Laboratory Medicine
B. Phosphate Buffer System
- At pH 7.4: HPO₄²⁻ / H₂PO₄⁻ = 4:1 (pKa = 6.8)
- Reactions:
- HPO₄²⁻ + H⁺ → H₂PO₄⁻
- H₂PO₄⁻ + OH⁻ → HPO₄²⁻ + H₂O
- Accounts for ~5% of non-bicarbonate buffer value of plasma
- Most important in urine — titrates and excretes acids in renal tubules
- Organic phosphate (2,3-DPG in RBCs) accounts for ~16% of non-bicarbonate buffering in erythrocytes
C. Plasma Protein Buffer System (especially albumin)
- Non-bicarbonate buffer value of plasma ≈ 7.7 mmol/L
- Proteins (>90% albumin) dominate non-bicarbonate buffering
- Imidazole groups of histidine residues are key proton acceptors/donors
D. Hemoglobin Buffer System
- Non-bicarbonate buffer value of erythrocyte fluid ≈ 63 mmol/L
- Hb accounts for ~53 mmol/L of this (major intracellular buffer)
- Critical because Hb carries CO₂ and buffers H⁺ generated in tissues
E. Intracellular Buffers
- Negatively charged phosphates and proteins inside cells
- Bone carbonate and phosphate also contribute (especially in chronic acidosis)
4. Respiratory Regulation (Fast, Minutes)
The lungs regulate PCO₂ (the acid component):
- Acidosis → chemoreceptors detect ↑H⁺ → hyperventilation → ↑CO₂ exhaled → PCO₂ falls → pH rises
- Alkalosis → hypoventilation → CO₂ retained → PCO₂ rises → pH falls
"The pH of plasma can be considered a function of two independent variables: (1) PCO₂, regulated by the lungs; and (2) the concentration of titratable base (HCO₃⁻), regulated by the kidneys." — Tietz Textbook of Laboratory Medicine
5. Renal Regulation (Slow but Powerful, Hours–Days)
The kidneys regulate [HCO₃⁻] (the base component). Renal tubule cells contain active carbonic anhydrase, enabling H⁺ and HCO₃⁻ production from CO₂.
| Condition | Kidney Response |
|---|---|
| Acidosis | ↑H⁺ secretion into tubular fluid (exchanged for Na⁺) + ↑HCO₃⁻ reabsorption → HCO₃⁻ returned to blood |
| Alkalosis | ↓H⁺ secretion + ↓HCO₃⁻ reabsorption → HCO₃⁻ lost in urine |
For each H⁺ secreted in response to acidosis, one Na⁺ and one HCO₃⁻ are added to the blood.
— Ganong's Review of Medical Physiology
6. Compensation vs. Correction
| Disturbance | Primary Change | Compensation |
|---|---|---|
| Metabolic acidosis | ↓HCO₃⁻ | Hyperventilation → ↓PCO₂ |
| Metabolic alkalosis | ↑HCO₃⁻ | Hypoventilation → ↑PCO₂ |
| Respiratory acidosis | ↑PCO₂ | Kidneys retain HCO₃⁻ (hours-days) |
| Respiratory alkalosis | ↓PCO₂ | Kidneys excrete HCO₃⁻ (hours-days) |
Compensatory mechanisms restore the HCO₃⁻/CO₂ ratio toward 20:1 without necessarily correcting the underlying cause. Importantly, the body never overcompensates — if pH is overcorrected, a second primary disturbance must be present.
7. Clinical Definitions Summary
| Term | Meaning |
|---|---|
| Acidemia | Arterial pH < 7.35 |
| Alkalemia | Arterial pH > 7.45 |
| Acidosis | Pathologic process tending to lower pH |
| Alkalosis | Pathologic process tending to raise pH |
| Mixed disorder | Two simultaneous primary processes |
Key Takeaway
pH regulation is an integrated system. Chemical buffers provide the immediate defense; the lungs respond within minutes by adjusting CO₂; and the kidneys provide the most sustained and powerful correction over hours to days by independently controlling plasma HCO₃⁻ concentration. All three systems act together to keep arterial pH within the narrow range of 7.35–7.45.
Sources: Medical Physiology (Boron & Boulpaep); Tietz Textbook of Laboratory Medicine, 7th Ed.; Ganong's Review of Medical Physiology, 26th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.