Explain pleth waveform and it's types using images
Reading File
Finding Sources
Searching the Web
pleth waveform types pulse oximeter photoplethysmography explained images
Loading Image
Loading Image
Loading Image
Finding Sources
Reading Web Page
https://www.frontiersin.org/journals/physiology/articles/10.…
Loading Image
Loading Image
Searching the Web
PPG pleth waveform respiratory variation pulsus paradoxus hypovolemia clinical types anesthesia
Loading Image
Loading Image
I now have comprehensive material. Here is the full explanation:
The Pleth Waveform (Photoplethysmography / PPG)
What Is the Pleth Waveform?
"Pleth" is short for photoplethysmography (PPG) - the graphical waveform displayed on pulse oximeters. It works by shining two wavelengths of light (red ~660 nm and infrared ~880 nm) through tissue (usually a fingertip) and measuring the changes in light absorption caused by pulsatile blood flow over time.
- The AC component (pulsatile) reflects the cyclic change in blood volume with each heartbeat
- The DC component (non-pulsatile) reflects the background absorption from venous blood, tissue, and bone
In essence, the pleth is an indirect, optical analogue of the arterial pressure waveform.
Anatomy of a Single PPG Waveform
Each individual wave has two phases:
| Phase | Description |
|---|---|
| Systolic (ascending) limb | Steep upstroke as the ventricle contracts and blood volume in the capillaries peaks |
| Systolic peak | Maximum blood volume under the sensor |
| Dicrotic notch | Brief dip caused by aortic valve closure and reflection of the pressure wave; may not always be visible on the pleth |
| Diastolic (descending) limb | Gradual downslope as blood volume falls |
| Diastolic peak | Secondary rise due to backward pressure wave just before the aortic valve closes |

Types of Pleth Waveform
1. Normal Pleth Wave
- Smooth, symmetric, consistent humps at regular intervals
- Amplitude matches heart rate
- The dicrotic notch may or may not be visible depending on monitor processing
- Indicates good perfusion and reliable SpO2 reading
2. Weak / Low Perfusion Pleth Wave
- Small amplitude, flattened waves
- Signal barely rises above baseline
- Causes: vasoconstriction, hypothermia, hypovolemia, peripheral vascular disease, cold hands, loose probe
Note: Some monitors auto-scale the Y-axis and artificially amplify a weak signal - this can mislead clinicians into thinking perfusion is adequate.
3. Noisy / Motion Artifact Pleth Wave
- Irregular, high-frequency, chaotic appearance
- Difficult to identify individual peaks
- Causes: patient movement, tremors, Parkinsonian tremor, shivering, poor probe contact
4. Motion-Affected / Irregular Pleth Wave
- Large irregular swings, variable peak heights, sudden drops
- The rhythm is recognizable but distorted
- Causes: talking, moving fingers, fidgeting, restlessness
5. Fading / Flattened Pleth Wave
- Wave amplitude gradually decreases and the signal disappears
- Causes: improper finger placement, artificial nails, dark nail polish, low battery, sensor malfunction

Clinical Waveform Pattern Types (ICU/Anesthesia Perspective)
These four patterns are specifically recognized in critical care monitoring:
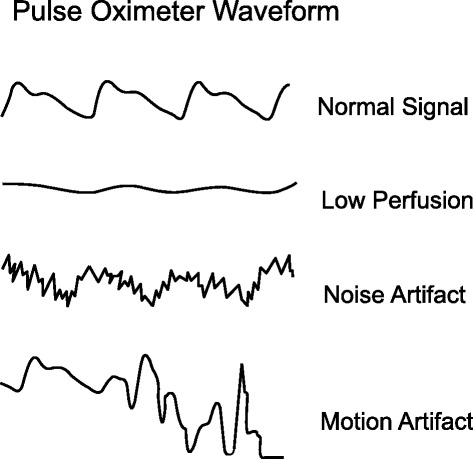
| Pattern | Appearance | Clinical Meaning |
|---|---|---|
| Normal signal | Regular, well-formed humps | Good perfusion, reliable reading |
| Low perfusion | Barely perceptible, flat | Vasoconstriction, shock, poor probe placement |
| Noise artifact | Rapid, chaotic, high-frequency spikes | Movement, shivering, EMI |
| Motion artifact | Irregular, large distorted swings | Patient movement |
Respiratory Modulation of the Pleth (Advanced)
The pleth waveform is modulated by breathing in three ways, visible as respiratory variation in the waveform:
| Modulation Type | Mechanism | Clinical Use |
|---|---|---|
| Baseline modulation (BM) | Respiratory changes in venous return shift the DC baseline up and down | Can extract respiratory rate non-invasively |
| Pulse amplitude modulation (AM) | Inspiration reduces venous return -> reduced stroke volume -> smaller pulse amplitude | Forms the basis of delta-POP and Pleth Variability Index (PVI) for fluid responsiveness |
| Respiratory sinus arrhythmia (RSA) | Heart rate increases on inspiration, decreases on expiration | Reflects autonomic tone |
A large respiratory swing in pulse amplitude on the pleth (>13%) - called delta-POP (DPOP) or the Pleth Variability Index (PVI) - predicts fluid responsiveness in mechanically ventilated patients, similar to pulse pressure variation (PPV) on an arterial line. This is a completely non-invasive method.
Pathological Pleth Patterns
| Condition | Pleth Finding |
|---|---|
| Hypovolemia / hemorrhage | Progressively decreasing amplitude with increased respiratory swings |
| Cardiac arrhythmia | Irregular peak-to-peak intervals; variable amplitude with AFib |
| Pulsus paradoxus (cardiac tamponade, severe asthma) | Exaggerated respiratory variation - amplitude drops >10 mmHg equivalent during inspiration |
| Vasodilation (sepsis, vasodilator drugs) | Bounding, large amplitude waves |
| Vasoconstriction (vasopressors, cold) | Diminished amplitude, sometimes absent |
| Aortic regurgitation | Bisferiens-type double peak pattern |
Two Measurement Configurations
PPG devices can be set up in two ways:
- Transmissive type: Light source and detector on opposite sides of tissue (e.g., fingertip probe) - most common in clinical settings
- Reflective type: Light source and detector on the same side (e.g., forehead sensor, wrist wearables) - more useful in vasoconstricted states and during hemorrhage, as the forehead is better perfused
Key Takeaways
- The pleth is far more than just a signal quality indicator - it contains rich cardiovascular, respiratory, and autonomic information
- Always check the waveform morphology alongside the SpO2 number - a falsely normal SpO2 can occur with a poor signal
- In ventilated patients, respiratory variation in the pleth (PVI/delta-POP) is a reliable non-invasive predictor of fluid responsiveness
- Amplitude correlates with cardiac output; regularity reflects rhythm; respiratory swing reflects volume status
Sources: Frontiers in Physiology (Elul et al., 2022, PMC8920970) | OpenCriticalCare.org | ScienceDirect - Photoplethysmography | Anesthesia & Analgesia - Shelley 2007
This is a shared conversation. Sign in to Orris to start your own chat.