Anatomy skull
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Reading File
Reading File
I now have all the information needed. Let me compile a comprehensive, detailed answer.
Skull Foramina & Their Contents
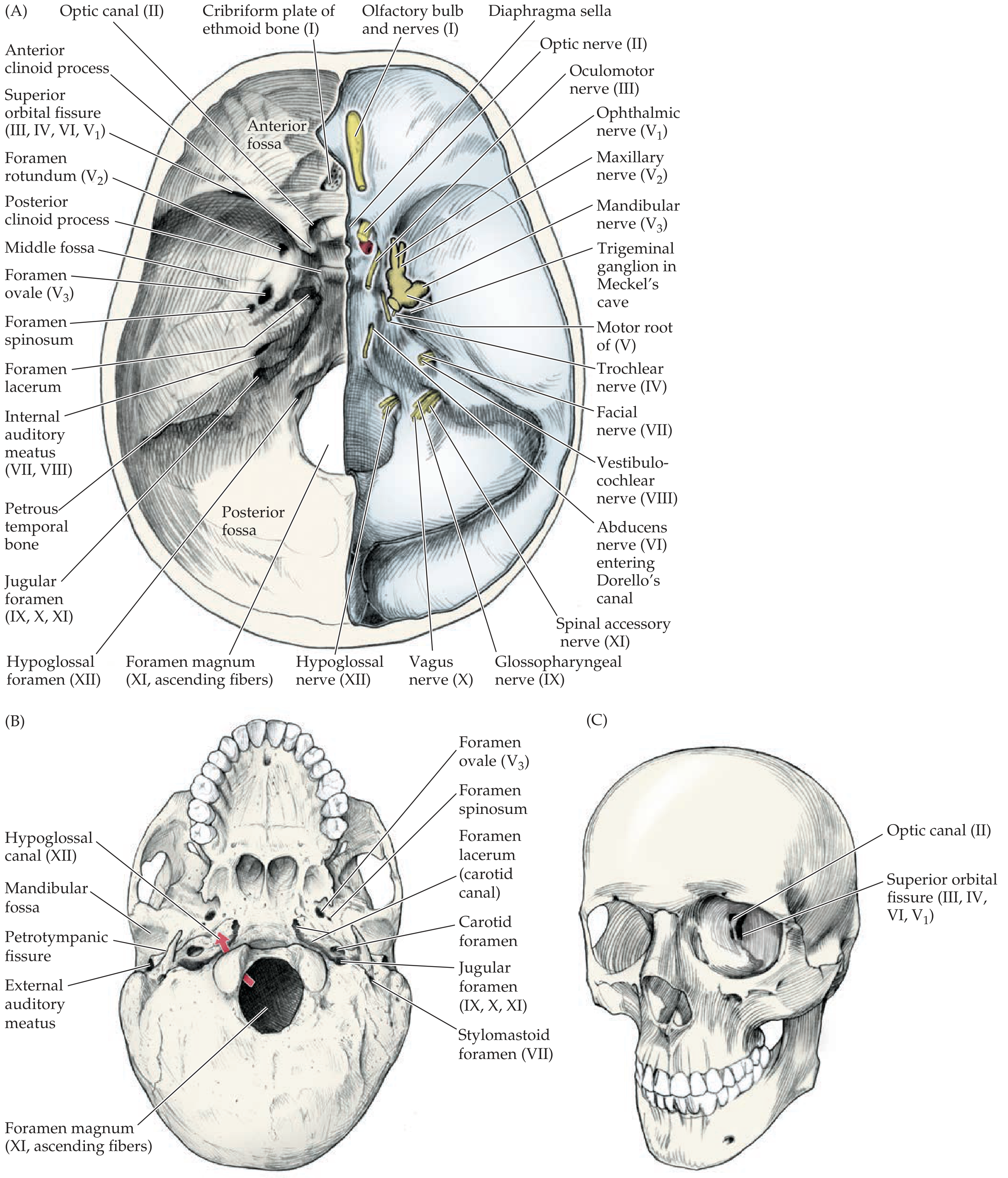
Figure 12.3 - Skull foramina serving as cranial nerve exit points. (A) Inside view of the cranial base from above; (B) External view of skull base from below; (C) Anterior view. - Neuroanatomy through Clinical Cases, 3rd Ed.
Organized by Cranial Fossa
Anterior Cranial Fossa
| Foramen | Contents |
|---|---|
| Foramina of cribriform plate (ethmoid bone) | Olfactory nerves (CN I) |
| Foramen cecum | Emissary veins to nasal cavity |
Middle Cranial Fossa
| Foramen | Contents |
|---|---|
| Optic canal | Optic nerve (CN II); ophthalmic artery |
| Superior orbital fissure | CN III (oculomotor), CN IV (trochlear), CN V1 (ophthalmic), CN VI (abducens via Dorello's canal); ophthalmic veins |
| Foramen rotundum | Maxillary nerve (CN V2) |
| Foramen ovale | Mandibular nerve (CN V3); lesser petrosal nerve; accessory meningeal artery; emissary vein |
| Foramen spinosum | Middle meningeal artery (and veins) |
| Foramen lacerum | Filled by fibrocartilage in life - no complete transit; the internal carotid artery traverses its superior part; deep petrosal nerve; greater petrosal nerve pass nearby |
| Hiatus for greater petrosal nerve | Greater petrosal nerve (branch of CN VII) |
| Hiatus for lesser petrosal nerve | Lesser petrosal nerve (from tympanic plexus, originally from CN IX) |
Posterior Cranial Fossa
| Foramen | Contents |
|---|---|
| Internal acoustic meatus (IAM) | CN VII (facial) including nervus intermedius; CN VIII (vestibulocochlear - superior vestibular, inferior vestibular, cochlear divisions); labyrinthine artery |
| Jugular foramen | Anterior part: inferior petrosal sinus; Middle: CN IX (glossopharyngeal), CN X (vagus), CN XI (accessory); Posterior: sigmoid sinus forming internal jugular vein; meningeal branches |
| Hypoglossal canal | CN XII (hypoglossal); meningeal branch of ascending pharyngeal artery; emissary vein; lymphatics |
| Foramen magnum | Medulla oblongata/upper spinal cord junction; vertebral arteries; anterior and posterior spinal arteries; ascending spinal rootlets of CN XI; meninges |
Cranial Nerve Exit Table (Quick Reference)
| CN | Name | Exit Foramen |
|---|---|---|
| I | Olfactory | Cribriform plate |
| II | Optic | Optic canal |
| III | Oculomotor | Superior orbital fissure |
| IV | Trochlear | Superior orbital fissure |
| V1 | Ophthalmic | Superior orbital fissure |
| V2 | Maxillary | Foramen rotundum |
| V3 | Mandibular | Foramen ovale |
| VI | Abducens | Superior orbital fissure (via Dorello's canal) |
| VII | Facial | Internal auditory canal → exits skull at stylomastoid foramen |
| VIII | Vestibulocochlear | Internal auditory canal |
| IX | Glossopharyngeal | Jugular foramen |
| X | Vagus | Jugular foramen |
| XI | Spinal accessory | Jugular foramen (enters via foramen magnum from below) |
| XII | Hypoglossal | Hypoglossal canal |
Key Clinical Points
- Foramen lacerum - the only foramen that is plugged with cartilage in life; nothing passes through it completely, though the carotid canal opens above it.
- CN VI has the longest intracranial course - travels through Dorello's canal before exiting the superior orbital fissure, making it vulnerable to raised intracranial pressure (false localizing sign).
- Jugular foramen syndrome - lesions here knock out CN IX, X, and XI together (Vernet's syndrome), causing hoarseness, dysphagia, and trapezius/SCM weakness.
- Cavernous sinus - CN III, IV, V1, V2, and VI all travel within or adjacent to the cavernous sinus before reaching the superior orbital fissure or foramen rotundum/ovale. A cavernous sinus lesion can hit multiple of these simultaneously.
- Stylomastoid foramen - CN VII exits here after traveling through the petrous temporal bone; this is the landmark used in parotid surgery.
Sources: Neuroanatomy through Clinical Cases, 3rd Ed. (Table 12.2, Fig. 12.3); Gray's Anatomy for Students (Table 8.2); K.J. Lee's Essential Otolaryngology; Cummings Otolaryngology
Frontalis skull
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Finding Sources
I have comprehensive material. Here is the full detailed answer:
The Frontal Bone - Detailed Anatomy
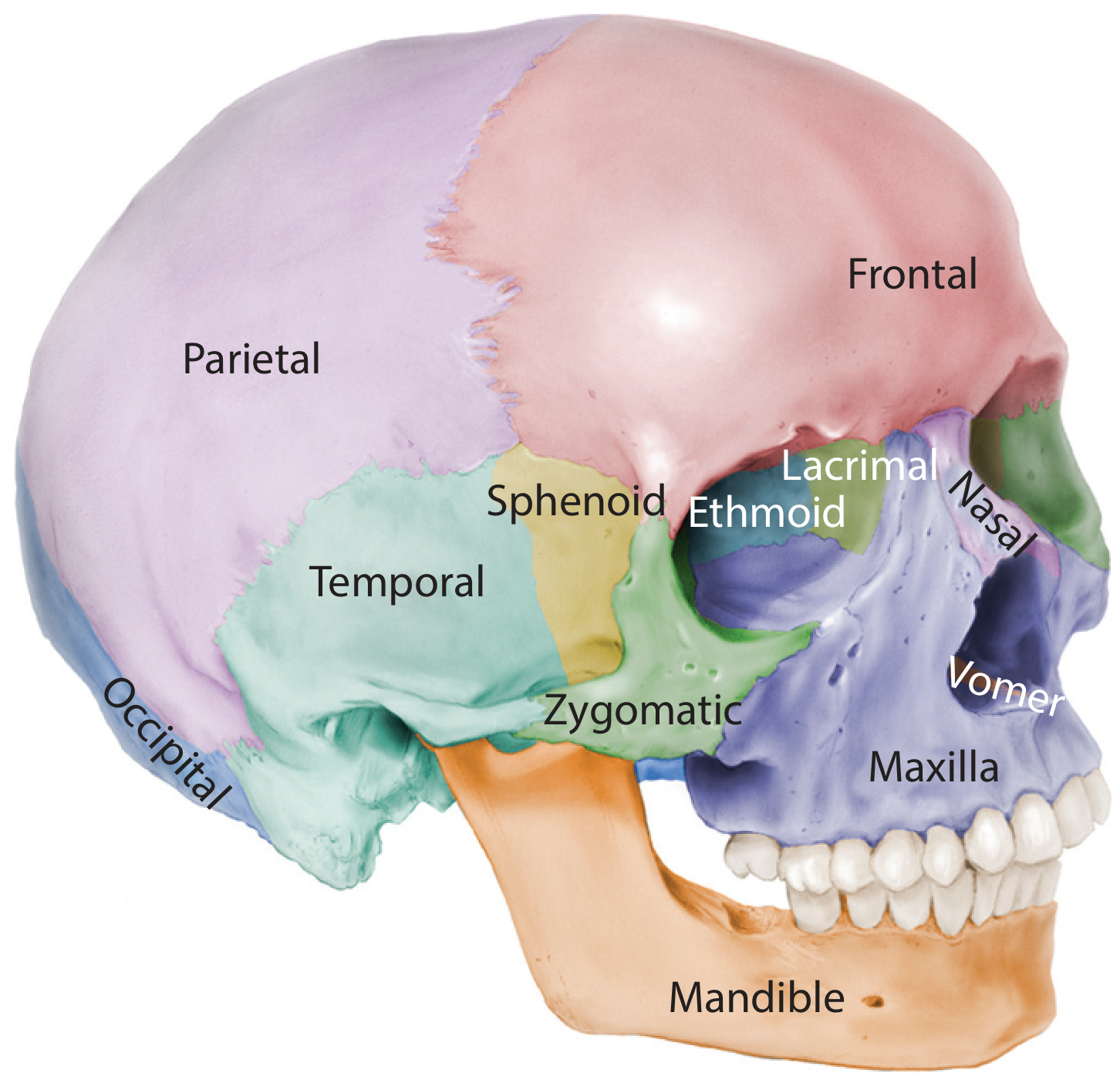
Lateral view of the skull with bones color-coded. The frontal bone (pink) occupies the forehead and superior orbital rim. - Forensic Anthropology: A Comprehensive Introduction
Overview
The frontal bone is a single bone (after fusion in early childhood) that forms:
- The forehead (squamous part)
- The superior rim and roof of both orbits (orbital parts)
- The floor of the anterior cranial fossa (internal surface)
- Houses the frontal sinuses (paired, internally)
Parts of the Frontal Bone
| Part | Location | Description |
|---|---|---|
| Squamous part | Forehead | Large, curved plate forming the forehead; bears the frontal eminences (bosses) |
| Orbital parts | Horizontal plates | Form the roof of the orbit and floor of the anterior cranial fossa; thin, perforated by the anterior and posterior ethmoidal foramina |
| Nasal part | Between orbits inferiorly | Articulates with nasal bones and nasal process of maxilla |
Key Surface Features
External (Anterior) Surface
| Feature | Description |
|---|---|
| Frontal eminences (bosses) | Bilateral rounded prominences above the orbits; more pronounced in females and children |
| Superciliary arches | Curved ridges above each orbit (eyebrow region); more prominent in males |
| Glabella | Smooth midline depression between the two superciliary arches |
| Supraorbital margin | Sharp inferior edge of the squamous part, forming the superior orbital rim |
| Supraorbital foramen (or notch) | Located at the junction of medial 1/3 and lateral 2/3 of the supraorbital margin; transmits supraorbital nerve and vessels (branch of CN V1) |
| Supratrochlear notch | Medial to the supraorbital foramen; transmits supratrochlear nerve and vessels |
| Zygomatic process | Lateral projection that articulates with the frontal process of the zygomatic bone; forms the upper lateral orbital rim |
| Temporal lines | Faint ridges on the lateral surface marking the attachment of temporalis muscle |
Internal (Endocranial) Surface
| Feature | Description |
|---|---|
| Frontal crest | Midline ridge for attachment of the falx cerebri (dura mater) |
| Foramen cecum | Small pit/foramen at the base of the frontal crest; transmits emissary veins between nasal mucosa and superior sagittal sinus (in fetal life; usually obliterated in adults) |
| Groove for superior sagittal sinus | Begins at the frontal crest, runs posteriorly |
| Orbital plate surfaces | Form the roof of the orbit; impressions of cerebral gyri visible |
Articulations
The frontal bone articulates with 8 bones:
| Bone | Suture / Joint |
|---|---|
| Parietal (×2) | Coronal suture (posteriorly) |
| Nasal (×2) | Frontonasal suture |
| Maxilla (×2) | Frontomaxillary suture |
| Ethmoid | Frontoethmoidal suture |
| Lacrimal (×2) | Frontolacrimal suture |
| Zygomatic (×2) | Zygomaticofrontal suture (lateral orbital rim) |
| Sphenoid | Inferoposteriorly (at pterion region) |
The two halves of the frontal bone fuse in the midline at the metopic suture during early childhood (2-3 years). A persistent metopic suture is present in ~8% of adults as a normal variant.
Skull Sutures Involving the Frontal Bone
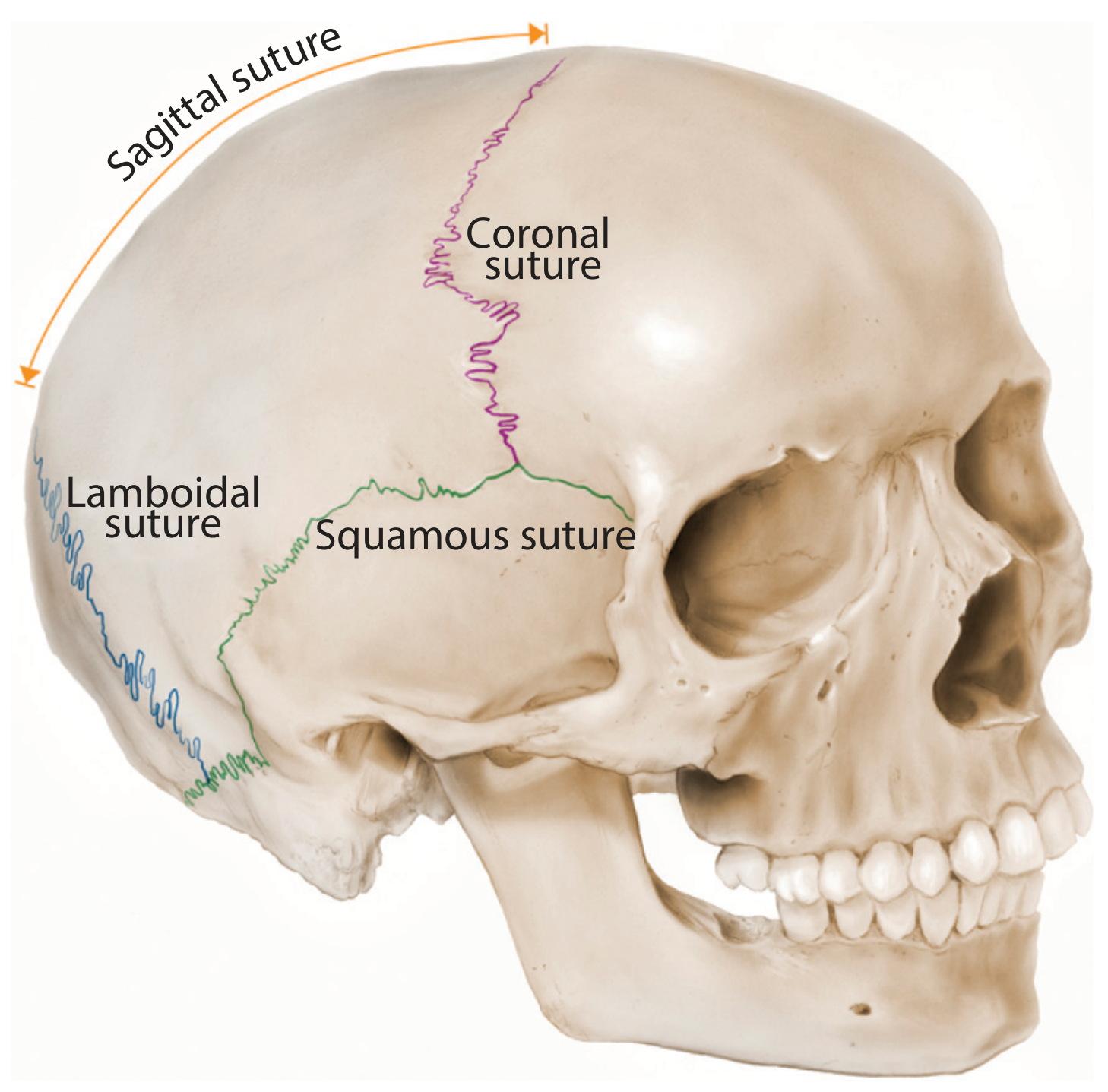
Skull sutures. The coronal suture (purple) separates the frontal bone anteriorly from the parietal bones posteriorly. - Forensic Anthropology: A Comprehensive Introduction
| Suture | Bones Joined | Location |
|---|---|---|
| Coronal | Frontal + both parietals | Runs coronally across the vault |
| Frontonasal | Frontal + nasal bones | Bridge of nose region |
| Zygomaticofrontal | Frontal + zygomatic | Lateral orbital rim |
| Metopic | Right + left frontal halves | Midline of forehead (fuses ~age 2) |
Bregma - the landmark point where the coronal suture meets the sagittal suture. Clinically important as the location of the anterior fontanelle in infants.
Frontal Sinuses
- Paired air spaces within the squamous part of the frontal bone, separated by a usually asymmetric septum
- Absent at birth; develop from age ~2 years, reach full size by late teens
- Drain via the frontonasal duct into the middle meatus of the nasal cavity (via the frontal recess/infundibulum)
- Lined by pseudostratified ciliated columnar epithelium (respiratory mucosa)
- Highly variable in size and shape between individuals
Clinical Relevance
| Condition | Relation to Frontal Bone |
|---|---|
| Frontal sinusitis | Infection of the frontal sinus; can spread intracranially through the thin posterior wall (extradural/subdural abscess, meningitis) - "Pott's puffy tumor" if subperiosteal abscess forms anteriorly |
| Frontal bone fracture | May involve the anterior table (cosmetic), posterior table (CSF leak risk, pneumocephalus), or frontal sinus (impaired drainage) |
| Craniosynostosis | Premature fusion of the coronal suture causes plagiocephaly or brachycephaly |
| Supraorbital nerve block | Injected at the supraorbital notch/foramen; provides anaesthesia to the forehead |
| Pterion | Thin region lateral to the frontal bone where frontal, parietal, temporal, and sphenoid converge - site of the middle meningeal artery; fractures here cause extradural haematoma |
Sources: Gray's Anatomy for Students; Forensic Anthropology: A Comprehensive Introduction, 2nd Ed.; Cummings Otolaryngology Head & Neck Surgery
Find research on metopic suture variations and clinical significance
Searching PubMed
metopic suture persistence variation anatomy
Searching PubMed
metopism craniosynostosis clinical significance
Finding Sources
Reading Article
PMID: 29049140
Reading Article
PMID: 39440539
Reading Article
PMID: 35523397
Reading Article
PMID: 32332546
Reading File
Reading Article
PMID: 34384857
Reading Article
PMID: 32266521
Reading Article
PMID: 38762603
Excellent - comprehensive data gathered. Here is the full synthesis:
Metopic Suture Variations & Clinical Significance
Background
The metopic suture (from Greek metopon = forehead) is a fibrous joint running in the midline of the frontal bone, from the nasion inferiorly to the bregma superiorly. It separates the two ossification centers of the frontal bone. Normally it fuses between 1-8 years of age, most commonly completing closure by age 2-3. Two distinct abnormalities arise from deviations in this process:
- Metopism - failure of fusion (suture persists into adulthood)
- Metopic craniosynostosis (trigonocephaly) - premature fusion
Part 1: Persistent Metopic Suture (Metopism)
Prevalence & Population Variation
Metopism is not rare, but its prevalence varies markedly across populations - a finding with both anthropological and diagnostic significance.
| Population | Prevalence |
|---|---|
| East Asian | ~15.4% |
| European | ~8.1% |
| Bengali | ~2.9% |
| Egyptian | ~2.2% |
| General mixed adult series | ~2.6-3.7% |
| African (non-Egyptian) | ~0% (not observed) |
| Peruvian | ~0% (not observed) |
| Females | ~3.8% |
| Males | ~1.8% |
Zdilla et al., 2018 (PMID: 29049140) - 505 crania from diverse populations
Metopism is more common in females than males across populations - a pattern not well explained but possibly linked to differences in suture closure timing.
Morphological Types
Both complete (nasion to bregma) and incomplete (partial) forms exist, each present in roughly equal proportions (~1.85% each in some series - Sharma et al., 2025, PMID: 39440539).
Effect on Overall Cranial Morphology
A 2022 geometric morphometric study (Nikolova et al., PMID: 35523397) on 63 metopic vs. 184 non-metopic male crania using 3D laser scanning found that metopism is not merely a local frontal variation - it reshapes the whole neurocranium:
- Anterior neurocranium enlarges at the expense of the middle and posterior parts
- Mediolateral widening with anteroposterior shortening - creating a more rounded overall skull shape
- Metopism represents "a complex condition associated with a combination of specific phenotypic characteristics," not an isolated finding
Effect on Sagittal Suture Closure
A striking finding (Nikolova et al., 2022, PMID: 34384857) using micro-CT in 122 male crania: sagittal suture closure is significantly delayed in metopic skulls compared to controls. This has two major practical implications:
- Forensic age-at-death estimates using sagittal suture closure are nearly twice as inaccurate in metopic individuals
- Persistent metopic suture and delayed sagittal closure may share a common biological pathway in suture patency regulation
Part 2: Metopic Craniosynostosis (Trigonocephaly)
Clinical Features
Premature fusion of the metopic suture produces a recognizable constellation (from Scott-Brown's Otorhinolaryngology, Head & Neck Surgery):
- Trigonocephaly - triangular, wedge-shaped forehead
- Supraorbital recession (flattening of the brow ridge)
- Hypotelorism - decreased interorbital and intercanthal distances
- Compensatory parietal widening - posterior skull growth increases to compensate for restricted anterior growth
- Incidence: the second most common single-suture craniosynostosis after sagittal synostosis
Spectrum: Metopic Ridge vs. Trigonocephaly
A key diagnostic challenge is distinguishing true trigonocephaly from a metopic ridge, which also results from early metopic closure but presents differently (Bloch et al., 2024, PMID: 38762603):
| Feature | Metopic Ridge | Trigonocephaly |
|---|---|---|
| Frontal shape | Mid-frontal bulging only | Triangular forehead |
| Hypotelorism | Absent | Present |
| Orbital morphology | Near-normal | Distinctly altered |
| Surgical correction | Rarely needed | Usually required |
| 3D frontal curvature | Intermediate | Clearly abnormal |
A 3D geometric morphometric approach (6 combined measurements) achieved 100% accuracy in distinguishing the two groups, outperforming standard 2D radiographic methods.
Genetics
A GWAS meta-analysis (Justice et al., 2020, PMID: 32266521 - Meta-Analysis, highest evidence tier) of 215 case-parent triads identified BMP7 locus (rs6127972) as the strongest replicated risk factor for nonsyndromic metopic craniosynostosis (OR 1.74, P = 1.27 × 10⁻⁸). Additional loci included SPRY3 and PCDH11X. Notably, the BMP7 enhancer region was significantly hypomethylated in mesenchymal stem cells from fused metopic sutures, suggesting an epigenetic mechanism.
Environmental teratogens during pregnancy are also a recognized cause. The empiric recurrence risk is ~5% for nonsyndromic cases with no identified cause.
Neurocognitive Outcomes
Long-term neurodevelopment after surgical correction correlates with preoperative radiographic severity (Gabrick et al., 2020, PMID: 32332546; Level II evidence):
- Overall, surgically corrected patients reach above-average IQ (mean 111.7) and near-national-average academic scores
- However, severe phenotype (endocranial bifrontal angle <124°) had significantly lower IQ and word reading scores vs. moderate phenotype
- Radiographic severity at diagnosis predicts long-term cognitive outcome - reinforcing the importance of early classification
Treatment
Fronto-orbital advancement and remodelling (FOAR) is the standard surgical approach, typically performed at 12-18 months of age:
- Coronal flap raised
- Forehead segment removed
- Supraorbital bar released, reshaped, advanced
- Neo-forehead attached with resorbable plate fixation
- Increases anterior cranial fossa volume, reduces raised ICP risk, corrects hypotelorism
Part 3: Clinical Significance Summary
| Clinical Context | Relevance |
|---|---|
| Radiology/Emergency | Persistent metopic suture mimics a frontal bone fracture on CT/X-ray - a potentially serious diagnostic pitfall in trauma |
| Forensic pathology | Metopism invalidates standard age-at-death models based on sagittal suture closure; separate regression models needed |
| Neurosurgery/Plastic surgery | Metopic craniosynostosis requires early surgical correction to prevent raised ICP and neurocognitive delay |
| Anthropology | Prevalence varies widely between populations; useful as a population-specific skeletal marker |
| Paediatrics | Metopic ridge vs. trigonocephaly distinction determines whether surgery is needed |
| Genetics counselling | ~5% recurrence risk; BMP7 pathway implicated; chromosomal copy number variants more common in metopic synostosis - aCGH warranted |
Key Papers
| PMID | Study | Finding |
|---|---|---|
| 29049140 | Zdilla et al. 2018 | Prevalence of metopism varies by population (0-15%); associated with frontal sinus abnormalities |
| 39440539 | Sharma et al. 2025 | 3.7% overall prevalence; both complete and incomplete forms; mimics fracture |
| 35523397 | Nikolova et al. 2022 | Metopism causes global cranial shape change - wider anteriorly, shorter AP |
| 34384857 | Nikolova et al. 2022 | Sagittal suture closure significantly delayed in metopic skulls - forensic age estimates unreliable |
| 32266521 | Justice et al. 2020 (Meta-Analysis) | BMP7 locus (rs6127972) is a replicated genetic risk factor for metopic craniosynostosis |
| 38762603 | Bloch et al. 2024 | 3D morphometric criteria distinguish trigonocephaly from metopic ridge with 100% accuracy |
| 32332546 | Gabrick et al. 2020 | Radiographic severity of craniosynostosis predicts long-term IQ and academic outcomes |
Textbook sources: Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol. 2; Forensic Anthropology: A Comprehensive Introduction, 2nd Ed.
Norma frontalis skull anatomy
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I have all the material needed. Here is the comprehensive Norma Frontalis answer:
Norma Frontalis - Anterior View of the Skull
Norma frontalis refers to the skull as viewed from directly in front. It is the most clinically and surgically relevant skull view, displaying the face, orbital cavities, nasal aperture, and the three key neurovascular foramina that lie in a vertical line.
Photograph - Anterior Skull (Norma Frontalis)
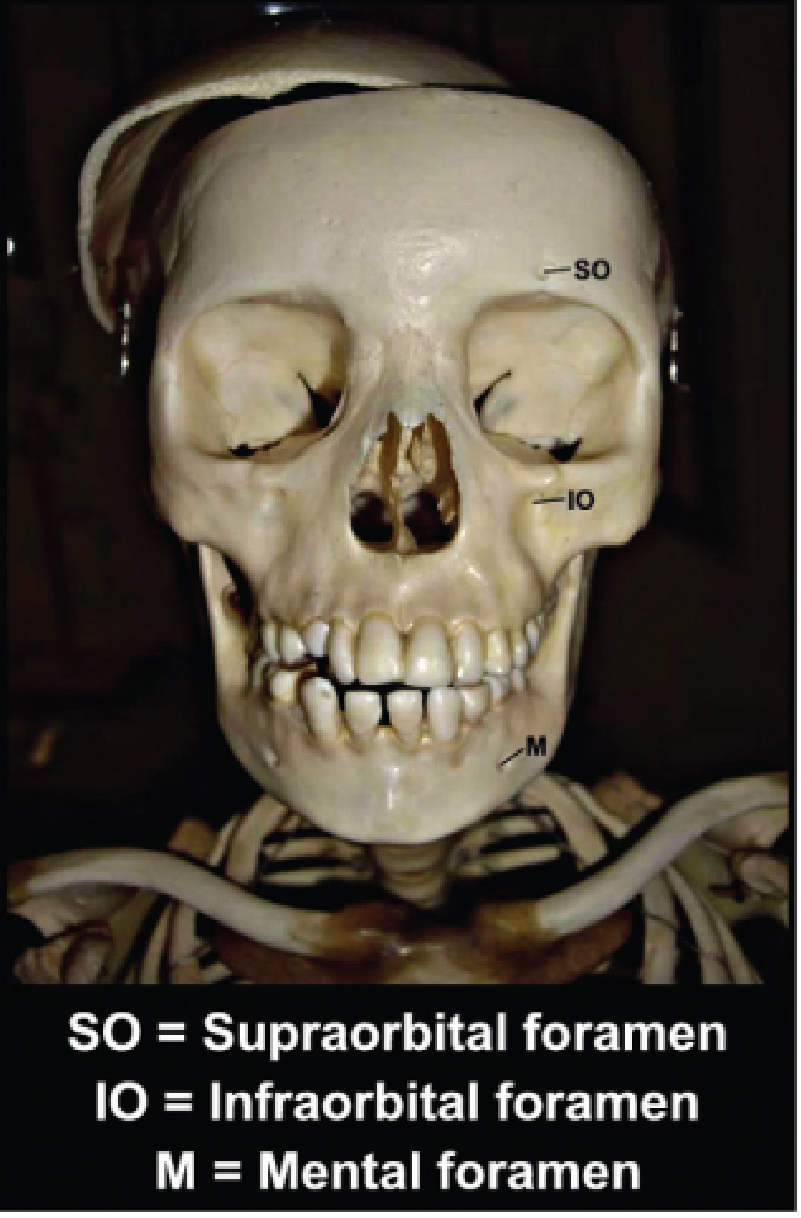
Norma frontalis of a dry skull. SO = supraorbital foramen; IO = infraorbital foramen; M = mental foramen - all three aligned vertically in the midpupillary line. - Barash Clinical Anesthesia, 9th Ed.
Bones Visible in Norma Frontalis
Working from top to bottom, the following bones contribute to the anterior skull:
| Bone | Region | Contribution |
|---|---|---|
| Frontal bone | Forehead & superior orbits | Forms the entire forehead; superior orbital margin; roof of orbit |
| Nasal bones (×2) | Bridge of nose | Form the bony bridge; articulate with each other at internasal suture and with frontal bone above |
| Zygomatic bones (×2) | Cheekbones | Form the lateral orbital wall and rim; the malar eminence of the cheek |
| Maxillae (×2) | Middle face | Inferior orbital rim; floor of orbit; anterior nasal spine; upper alveolar arch; hard palate anteriorly |
| Ethmoid bone | Between orbits | Contributes to the medial orbital wall (lamina papyracea); visible at the medial orbital margins |
| Lacrimal bones (×2) | Medial orbital wall | Tiny bones at the anteromedial orbital wall; contain the lacrimal groove |
| Vomer | Nasal septum | Lower part of bony nasal septum (partially visible through the piriform aperture) |
| Mandible | Lower face | Body (with mental protuberance) and part of the rami visible |
| Sphenoid (lesser wings) | Deep orbit | Visible in the depths of the orbit forming the posterior orbital wall |
Key Bony Landmarks (Norma Frontalis)
Midline Landmarks (Superior to Inferior)
| Landmark | Location | Description |
|---|---|---|
| Trichion | Hairline | Midline point of the hairline (soft tissue) |
| Glabella | Forehead | Smooth, slightly convex midline area between the two superciliary arches, above the nasion |
| Nasion | Nasofrontal junction | Deepest point of the nasofrontal angle; junction of frontal and nasal bones; corresponds to the frontonasal suture |
| Internasal suture | Bridge of nose | Vertical midline suture between the two nasal bones |
| Anterior nasal spine | Base of nasal aperture | Sharp midline bony projection at the base of the piriform aperture from the maxilla |
| Intermaxillary suture | Upper jaw midline | Suture between the two maxillae |
| Mental protuberance | Chin | Triangular bony prominence at the midline of the mandible body |
| Mental symphysis | Mandible midline | Fused midline of the mandible (fuses by age 1-2 years) |
The Orbit - Boundaries in Norma Frontalis
The orbit is a quadrilateral pyramid pointing posteriorly. Its anterior opening (aditus orbitae) is seen in full in norma frontalis:
| Margin | Bone(s) |
|---|---|
| Superior orbital margin | Frontal bone (entire) |
| Lateral orbital margin | Zygomatic bone (inferior 2/3) + Frontal bone (superior 1/3) |
| Inferior orbital margin | Maxilla (medial 2/3) + Zygomatic bone (lateral 1/3) |
| Medial orbital margin | Frontal bone (superiorly) + Maxilla (inferiorly) |
Within the orbit, the superior orbital fissure and optic canal are visible in the depths.
The Three Anterior Foramina - "The Vertical Line"
The most clinically important feature of norma frontalis is that the three major sensory foramina of the face all lie in the same vertical line - the midpupillary line (~2.5 cm lateral to the midline):
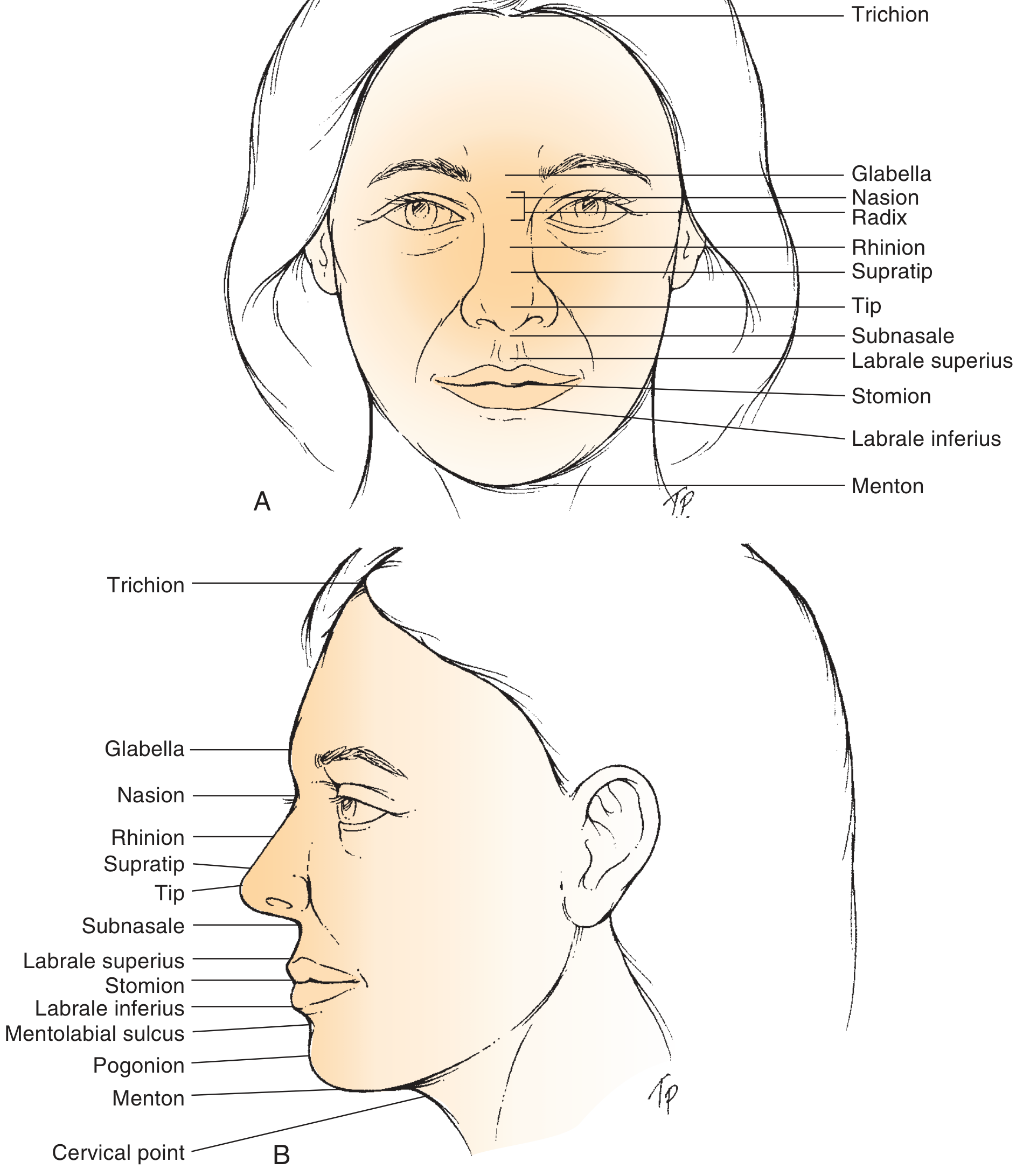
Soft tissue reference points of the face (frontal and lateral views). - Cummings Otolaryngology
| Foramen | Bone | Position | Nerve | Artery |
|---|---|---|---|---|
| Supraorbital foramen (or notch) | Frontal bone | Superior orbital margin, junction of medial 1/3 and lateral 2/3 | Supraorbital nerve (CN V1) | Supraorbital artery |
| Infraorbital foramen | Maxilla | 1 cm below inferior orbital rim, midpupillary line | Infraorbital nerve (CN V2) | Infraorbital artery |
| Mental foramen | Mandible | Midportion of mandibular body, between premolars | Mental nerve (CN V3) | Mental artery |
All three foramina are at the same vertical plane (~2.5 cm lateral to the midline). This is the basis for regional nerve block anaesthesia of the entire face using just three injections.
Sutures Visible in Norma Frontalis
| Suture | Bones Joined |
|---|---|
| Metopic suture | Between two halves of frontal bone (only visible if persistent into adulthood) |
| Frontonasal suture | Frontal bone + nasal bones |
| Frontozygomatic suture | Frontal bone + zygomatic bone (lateral orbital rim) |
| Frontomaxillary suture | Frontal bone + frontal process of maxilla (medial orbital rim) |
| Internasal suture | Right + left nasal bones |
| Nasomaxillary suture | Nasal bone + frontal process of maxilla |
| Zygomaticomaxillary suture | Zygomatic bone + maxilla (inferior orbital rim / cheek) |
| Intermaxillary suture | Right + left maxillae (midline upper jaw) |
| Mental symphysis | Two halves of mandible (fused in adult) |
The Piriform (Anterior Nasal) Aperture
The piriform aperture (pear-shaped nasal opening) is bounded by:
- Superiorly: Nasal bones (inferior free edges)
- Laterally and inferiorly: Nasal notch of the maxillae on each side
- Floor: Anterior nasal spine (midline projection from maxilla)
It is the anterior opening to the nasal cavity. The bony nasal septum (perpendicular plate of ethmoid + vomer) is visible through it.
Facial Thirds (Vertical Analysis)
The face in norma frontalis is classically divided into equal thirds - a key measurement in surgical and orthodontic planning:
| Third | Landmarks | Bony Basis |
|---|---|---|
| Upper third | Trichion → Glabella | Frontal bone |
| Middle third | Glabella → Subnasale | Nasal bones, maxilla, orbits |
| Lower third | Subnasale → Menton | Maxilla (lower) + Mandible |
An alternative method (excluding variable hairline) measures nasion → subnasale (43% of lower face height) and subnasale → menton (57%).
Facial Fifths (Horizontal Analysis)
The face is divided into 5 equal vertical fifths, each equal to one eye width:
- The intercanthal distance (medial canthus to medial canthus) should equal one eye width
- The nasal base width should equal the intercanthal distance
- The mouth width is approximately 1.5x the intercanthal distance
Clinical Relevance of Norma Frontalis
| Context | Relevance |
|---|---|
| Nerve blocks | All three foramina (supraorbital, infraorbital, mental) in the midpupillary line are injection targets for regional facial anaesthesia |
| Facial fractures | Le Fort fractures, orbital floor "blow-out" fractures, and nasal bone fractures all involve bones seen in this view |
| Rhinoplasty | Nasion position, intercanthal distance, and piriform aperture dimensions guide surgical planning |
| Orbital surgery | Orbital rim boundaries and sutures are surgical landmarks |
| Forensic identification | Glabella, nasion, orbits, and piriform aperture morphology are used in facial reconstruction and sex/population determination |
Sources: Barash Clinical Anesthesia, 9th Ed.; Cummings Otolaryngology Head & Neck Surgery; Dermatology 2-Volume Set, 5th Ed.; Gray's Anatomy for Students; Forensic Anthropology: A Comprehensive Introduction, 2nd Ed.
Photo dikha sutures ki
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Loading Image
Finding Sources
Loading Image
Loading Image
Loading Image
4 excellent images mil gayi hain - lateral view, superior (internal) view, newborn skull, aur craniosynostosis diagram. Sab clearly labeled hain. Ab complete answer present karta hoon:
Skull Sutures - Photos & Diagrams
Yahan skull ki sutures ki 4 different views ki images hain, sab textbooks se:
1. Lateral View (Side se) - Sutures Highlighted
Yahan dikhi sutures:
- 🟣 Coronal suture - Frontal bone ko Parietal bones se alag karti hai (forehead ke peeche)
- 🟢 Squamous suture - Parietal bone ko Temporal bone se alag karti hai (side mein)
- 🔵 Lambdoidal suture - Parietal bones ko Occipital bone se alag karti hai (peeche)
- Sagittal suture - Orange arrow se dikhaya gaya hai - midline mein upar se peeche tak chali jaati hai
2. Superior View (Upar se, Internal) - Detailed Labeled
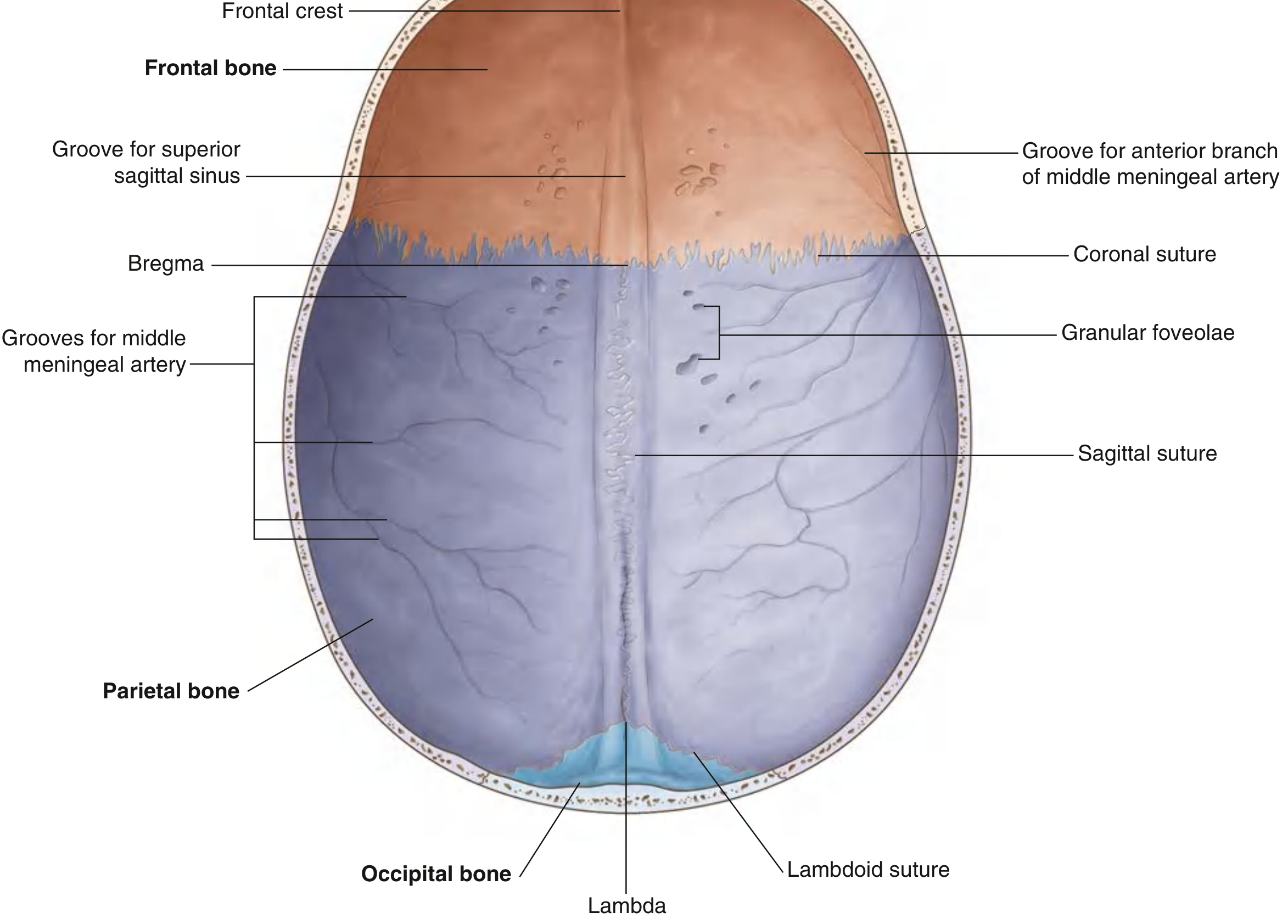
Key points:
- Bregma = Coronal + Sagittal sutures ka meeting point (anterior fontanelle ki jagah)
- Lambda = Sagittal + Lambdoid sutures ka meeting point (posterior fontanelle ki jagah)
- Groove for superior sagittal sinus midline mein clearly dikha raha hai
- Granular foveolae = Arachnoid granulations ki impressions
3. Newborn Skull - Superior View (Fontanelles ke saath)
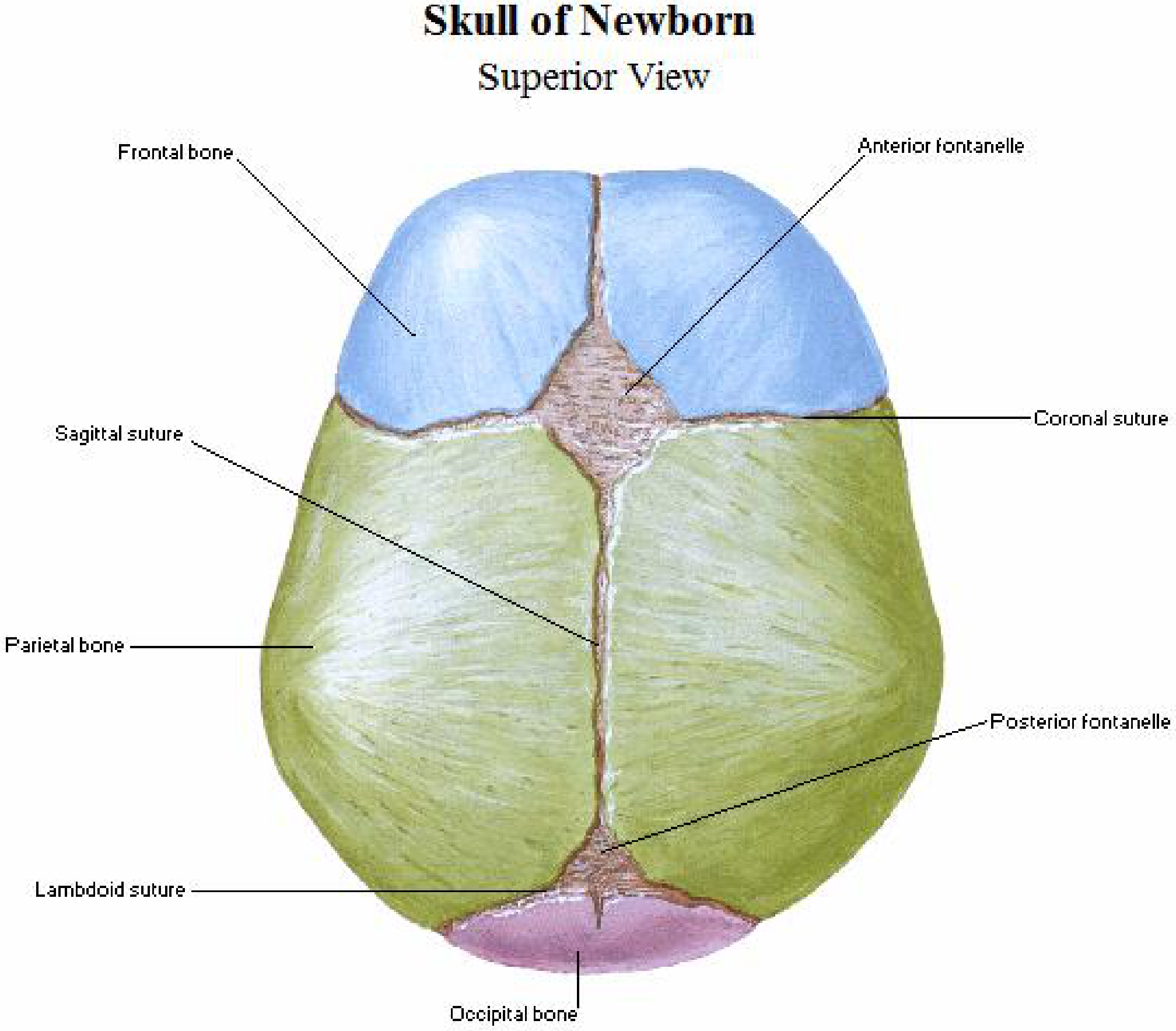
Newborn mein sutures ke saath fontanelles bhi hoti hain:
| Fontanelle | Sutures ka Junction | Closure Age |
|---|---|---|
| Anterior (Bregma) | Coronal + Sagittal + Metopic | 18-24 months |
| Posterior (Lambda) | Sagittal + Lambdoid | 2-3 months |
4. Sutures aur Premature Closure se Skull Shapes
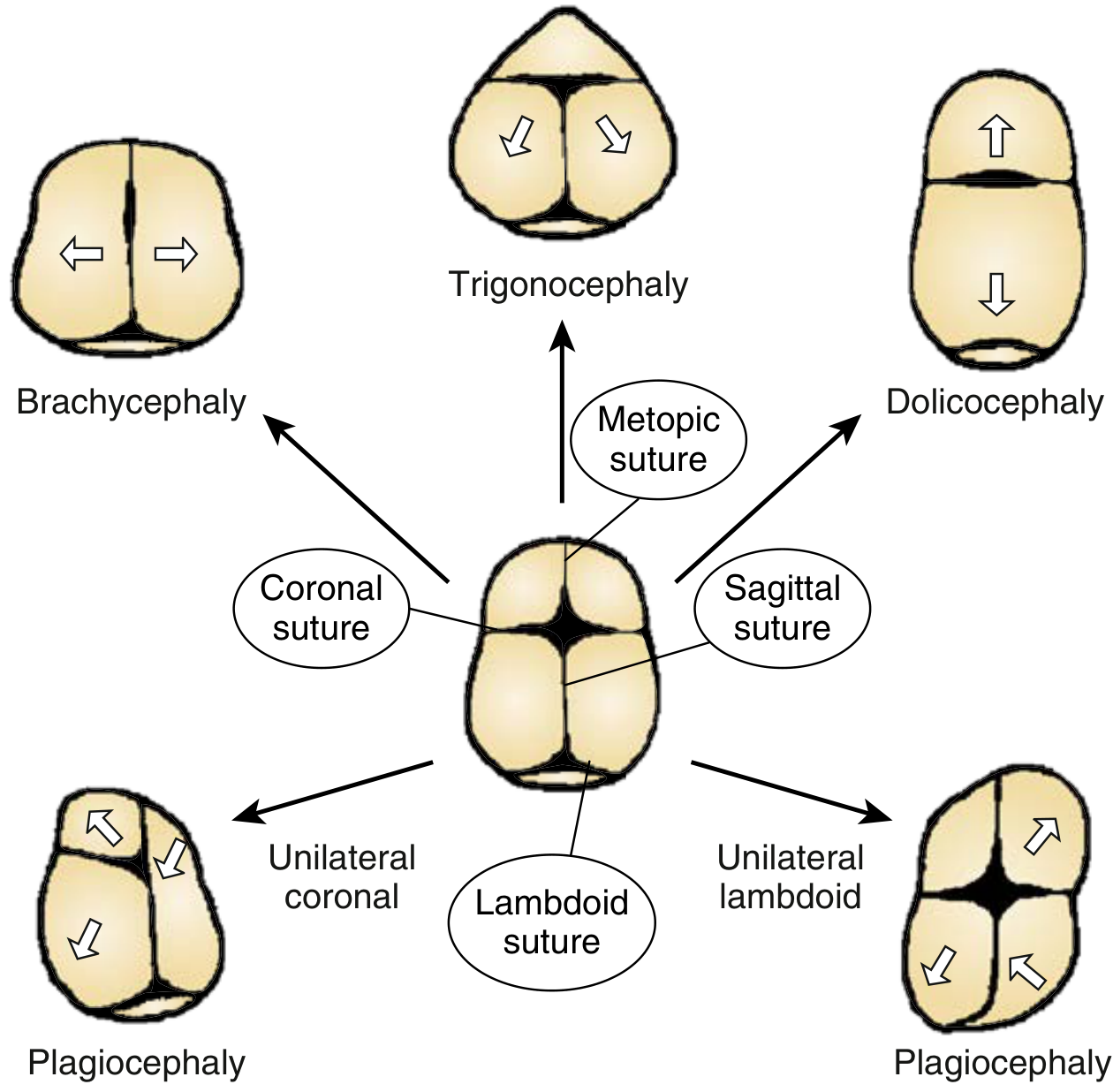
Agar suture premature fuse ho jaye to:
| Suture | Deformity |
|---|---|
| Metopic (midline frontal) | Trigonocephaly - triangular forehead |
| Coronal (bilateral) | Brachycephaly - wide, short skull |
| Sagittal (midline) | Dolichocephaly - long, narrow skull |
| Unilateral Coronal/Lambdoid | Plagiocephaly - asymmetric/oblique skull |
Quick Summary - Skull Ki Major Sutures
| Suture | Bones Joined | Location |
|---|---|---|
| Sagittal | Right + Left Parietal | Midline, top of skull |
| Coronal | Frontal + Both Parietals | Across the vault (transverse) |
| Lambdoid | Both Parietals + Occipital | Posterior, λ-shaped |
| Squamous | Parietal + Temporal | Side of skull |
| Metopic | Two halves of Frontal | Midline forehead (fuses by age 2-3) |
| Sphenoparietal | Sphenoid + Parietal | Pterion region |
Closure Order (Forensic importance):
Sagittal (30-35 yr) → Coronal (35-40 yr) → Lambdoid (45-50 yr) → Squamous (55-60 yr)
Sources: Forensic Anthropology: A Comprehensive Introduction, 2nd Ed.; Gray's Anatomy for Students; Netter's Atlas of Human Anatomy; Creasy & Resnik's Maternal-Fetal Medicine
Orbital
Your credits are exhausted. You can purchase a top-up or subscribe to a plan to continue using Orris. If you're already subscribed, your daily credits will reset tomorrow.
This is a shared conversation. Sign in to Orris to start your own chat.