Shoulder joint in anatomy
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
I now have comprehensive content from Gray's Anatomy for Students and the THIEME Atlas of Anatomy. Let me compile the full detailed answer.
Shoulder Joint (Glenohumeral Joint) - Complete Anatomy
1. Classification and Overview
The shoulder (glenohumeral) joint is a synovial ball-and-socket articulation between the large spherical head of the humerus and the small, shallow glenoid cavity of the scapula. It is multiaxial - the most mobile joint in the body - allowing movement in virtually all planes, but at the cost of bony stability. Stability is maintained instead by surrounding muscles, ligaments, and the glenoid labrum.
Fig. 7.25 - Articular surfaces of the glenohumeral joint (A = anatomy diagram; B = normal AP radiograph):
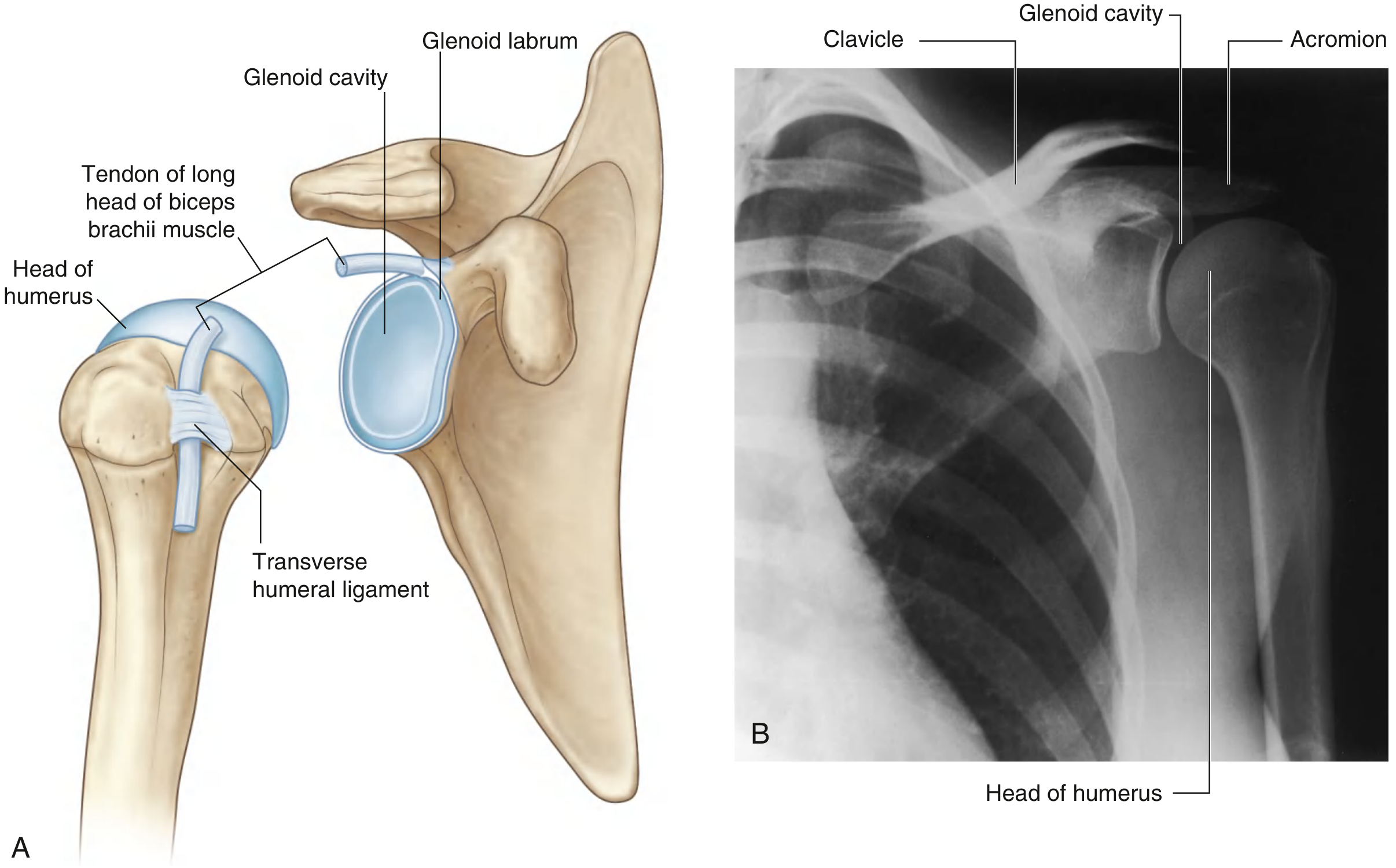
2. Articular Surfaces
| Surface | Bone | Description |
|---|---|---|
| Head of humerus | Humerus | Large, spherical; covered by hyaline cartilage |
| Glenoid cavity | Scapula | Small, shallow pear-shaped fossa; covered by hyaline cartilage |
The glenoid cavity is approximately one-third the size of the humeral head, making congruency poor by itself.
3. Glenoid Labrum
A fibrocartilaginous rim - the glenoid labrum - attaches to the margin of the glenoid cavity, deepening and expanding it peripherally. It increases the depth of the socket only modestly, but:
- Superiorly, it is continuous with the tendon of the long head of biceps brachii (which attaches to the supraglenoid tubercle and passes through the articular cavity above the humeral head).
- Tears of the anteroinferior labrum (Bankart lesion) predispose to recurrent dislocation.
4. Joint Capsule
Fibrous membrane:
- Attaches medially to the margin of the glenoid cavity (outside the labrum) and laterally to the anatomical neck of the humerus
- On the humerus, the medial attachment extends onto the shaft, creating a redundant (loose) inferior fold that accommodates abduction
- Contains openings for communication with bursae
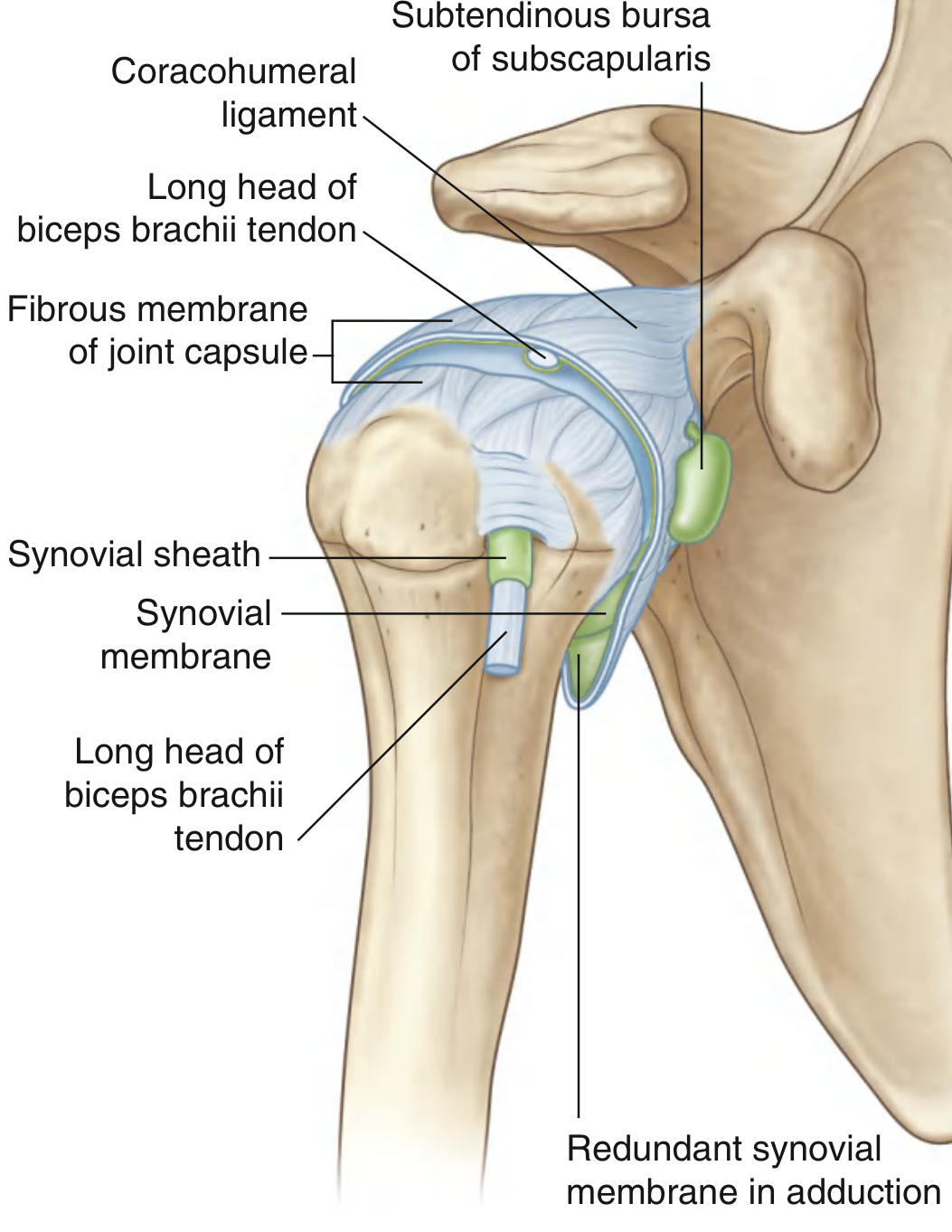
Synovial membrane:
- Lines the entire fibrous capsule
- Is especially loose inferiorly (the axillary recess) - this redundancy allows full abduction
- Protrudes through capsule apertures to form bursae
- Wraps around the tendon of the long head of biceps within the joint and extends along it into the intertubercular sulcus (bicipital groove)
Synovial membrane and joint capsule showing the redundant inferior fold and bursae:
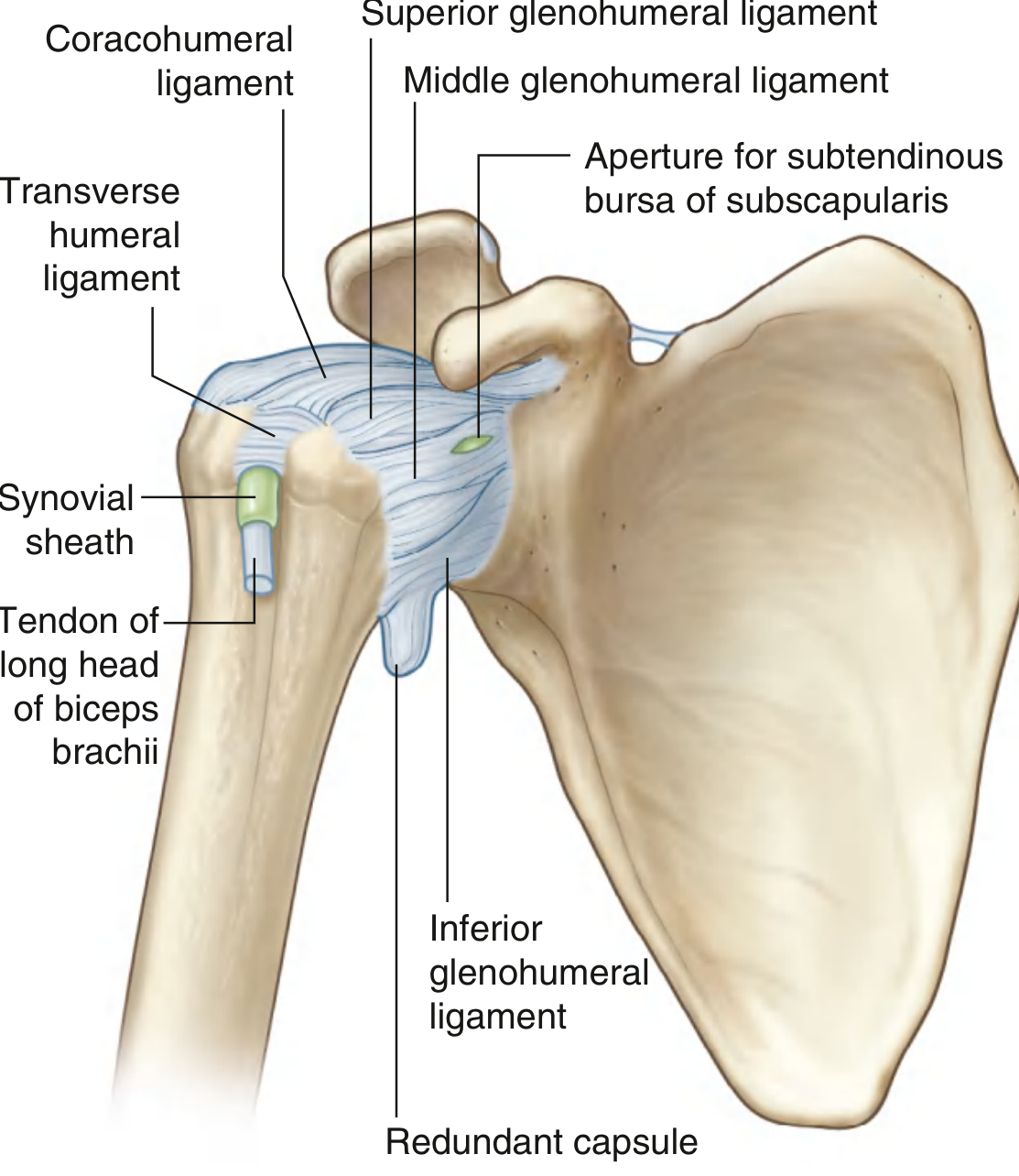
5. Ligaments
A. Glenohumeral Ligaments (thickenings of the anterior capsule)
These three ligaments reinforce the anterosuperior capsule and are most clearly visible arthroscopically:
| Ligament | Attachment | Role |
|---|---|---|
| Superior GHL | Upper margin of glenoid to intertubercular groove/lesser tubercle | Forms floor of "biceps pulley" in the rotator interval |
| Middle GHL | Upper margin of glenoid to anatomic neck of humerus | Runs at almost a right angle to subscapularis tendon |
| Inferior GHL | Inferior margin of glenoid to anatomic/surgical neck | Three parts: anterior band, posterior band, axillary recess; acts as a "hammock" - primary stabilizer against anteroinferior dislocation during abduction |
B. Coracohumeral Ligament
- Arises from the base of the coracoid process as a strong, broad band
- Its two parts pass to the greater and lesser tubercles
- Together with the superior GHL, it forms the rotator interval and creates the "biceps pulley" that stabilizes the long head of biceps tendon
C. Transverse Humeral Ligament
- Bridges between the greater and lesser tubercles of the humerus
- Holds the tendon of the long head of biceps brachii within the intertubercular sulcus
D. Coracoacromial Ligament (extracapsular)
- Passes from the coracoid process to the acromion
- Together with the acromion and coracoid process, forms the coracoacromial arch - a bony/ligamentous roof that prevents superior dislocation
Capsule and ligaments - anterior view of right glenohumeral joint:
6. Bursae
Several bursae reduce friction around the joint:
| Bursa | Location | Communication |
|---|---|---|
| Subtendinous bursa of subscapularis | Between subscapularis tendon and fibrous capsule | Communicates with joint (most consistent) |
| Subacromial (subdeltoid) bursa | Between acromion/deltoid and supraspinatus/capsule | Does NOT communicate with joint normally |
| Subcoracoid bursa | Between coracoid process and joint capsule | May communicate with joint |
| Subcutaneous acromial bursa | Between acromion and skin | No communication |
| Subtendinous bursa of infraspinatus | Deep to infraspinatus | May communicate |
The subacromial and subdeltoid bursae consistently communicate with each other. They are clinically important in rotator cuff impingement.
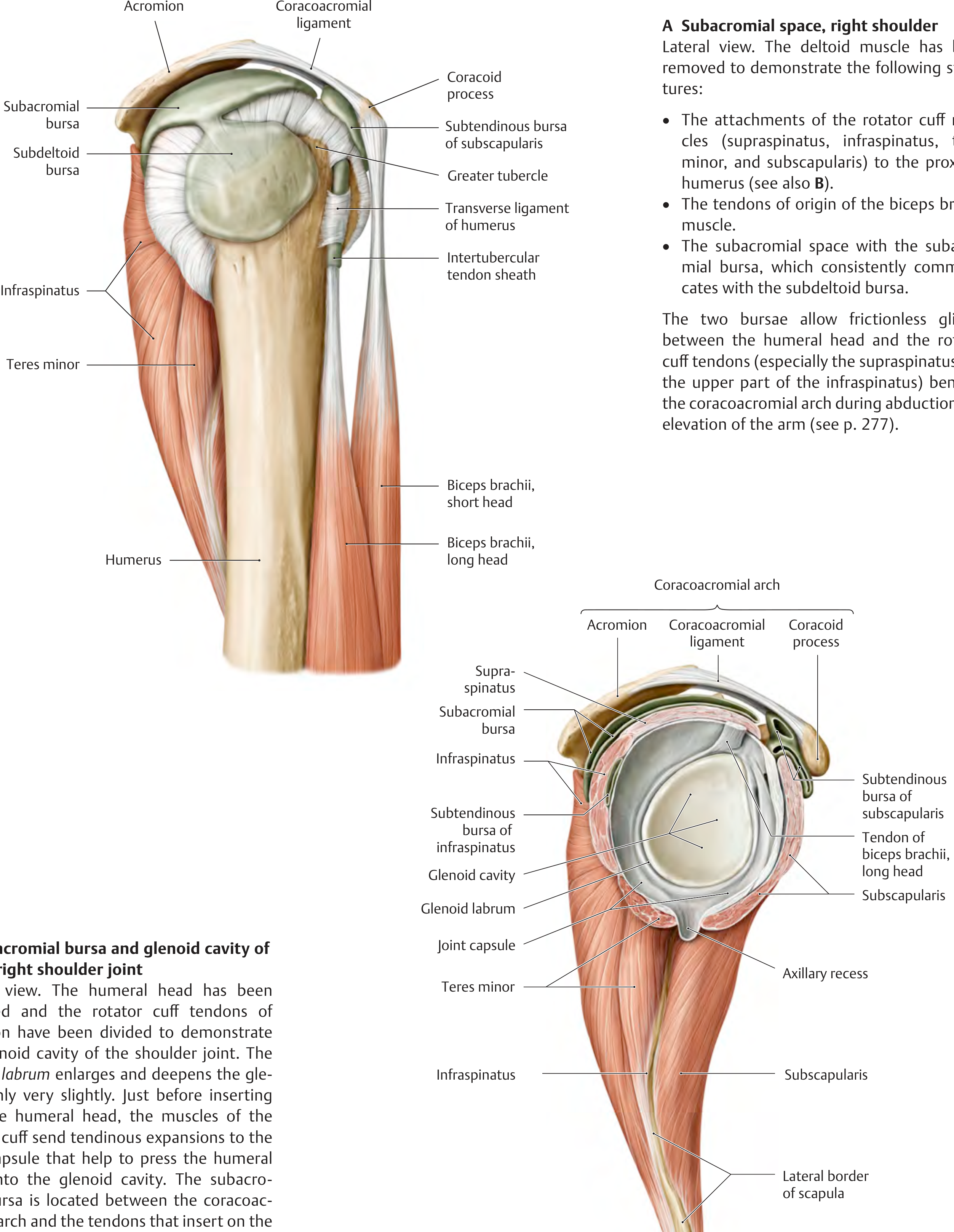
7. Rotator Cuff - The Key Stabilizers
The rotator cuff is a musculotendinous collar formed by four muscles whose tendons blend with the joint capsule and hold the humeral head in the glenoid. They surround the posterior, superior, and anterior aspects of the joint.
Mnemonic: SITS
| Muscle | Origin | Insertion | Action | Nerve |
|---|---|---|---|---|
| Supraspinatus | Supraspinous fossa | Greater tubercle (superior facet) | Initiates abduction (0-15°) | Suprascapular n. |
| Infraspinatus | Infraspinous fossa | Greater tubercle (middle facet) | Lateral rotation | Suprascapular n. |
| Teres minor | Lateral border of scapula | Greater tubercle (inferior facet) | Lateral rotation | Axillary n. |
| Subscapularis | Subscapular fossa | Lesser tubercle | Medial rotation; anterior stability | Upper & lower subscapular nn. |
The inferior aspect of the joint is the weakest point of the cuff - it is not covered by rotator cuff muscle, which is why most dislocations go anteroinferiorly.
Lateral view showing the rotator cuff muscles, subacromial space, and bursae:
8. Rotator Interval
The rotator interval is the triangular capsular gap between the:
- Superior edge of subscapularis (anteriorly)
- Anterior edge of supraspinatus (superiorly)
It is reinforced by the superior GHL and coracohumeral ligament, which together form the biceps pulley - a sling that prevents medial dislocation of the biceps long head tendon.
9. Other Muscles Acting at the Shoulder
Beyond the rotator cuff, several larger muscles produce the powerful movements of the arm:
Posterior/Lateral:
- Deltoid - primary abductor (15-90°); anterior fibers flex, posterior fibers extend
- Teres major - adduction, medial rotation, extension
- Latissimus dorsi - adduction, medial rotation, extension
Anterior:
- Pectoralis major - flexion (clavicular head), adduction, medial rotation
- Coracobrachialis - flexion, adduction
Crossing the joint:
- Biceps brachii (long head) - depresses humeral head, restricts upward translation
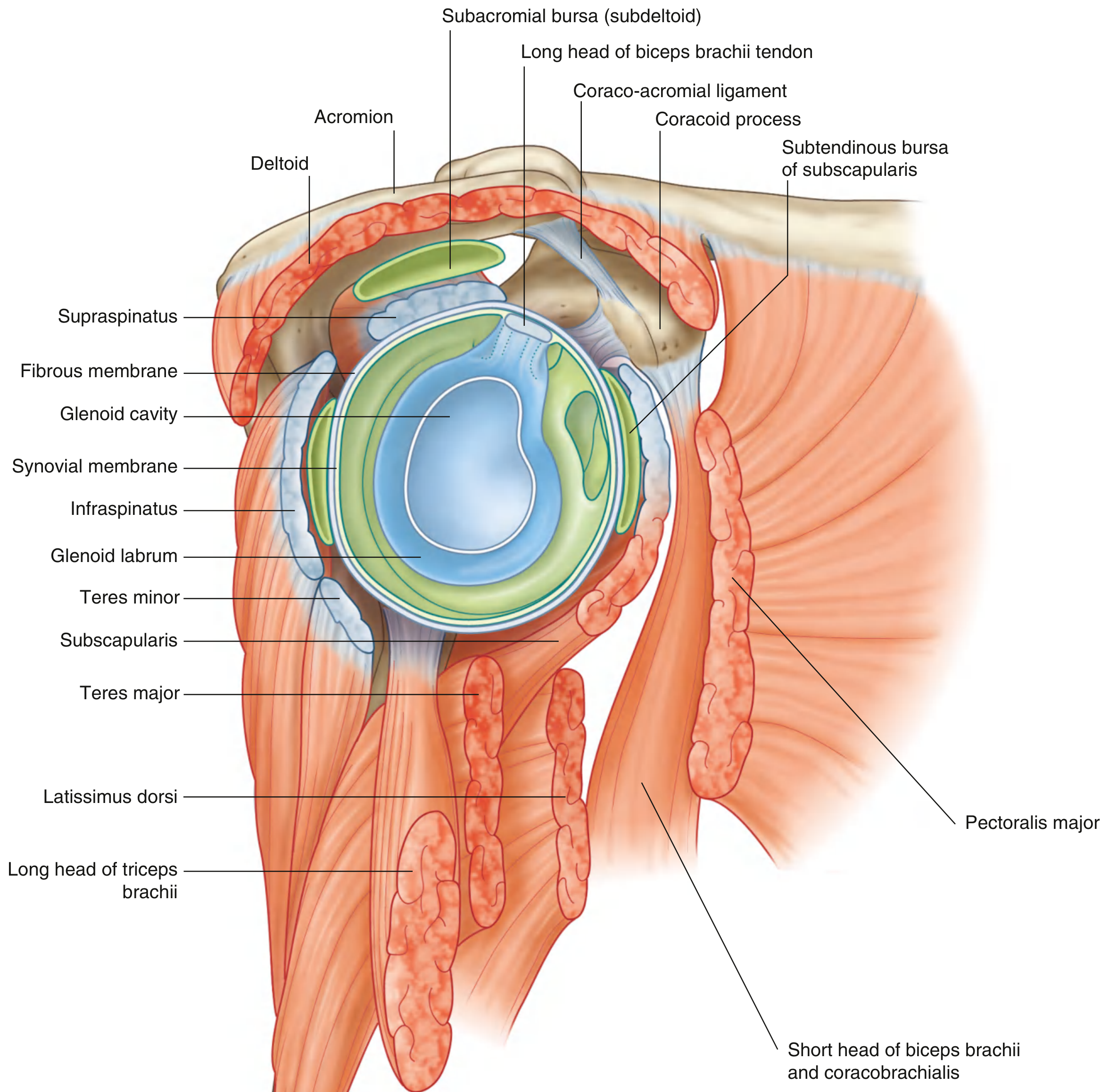
Cross-sectional lateral view showing all muscle relationships:
10. Movements and Range
| Movement | Range | Prime Movers |
|---|---|---|
| Flexion | 0-180° (with scapular rotation) | Anterior deltoid, pectoralis major (clavicular), coracobrachialis |
| Extension | 0-60° | Posterior deltoid, teres major, latissimus dorsi |
| Abduction | 0-180° (glenohumeral + scapulothoracic) | Supraspinatus (0-15°), deltoid (15-90°), trapezius + serratus anterior (90-180°) |
| Adduction | 0-50° | Pectoralis major, latissimus dorsi, teres major |
| Medial rotation | 0-90° | Subscapularis, pectoralis major, teres major, latissimus dorsi |
| Lateral rotation | 0-60° | Infraspinatus, teres minor, posterior deltoid |
| Circumduction | Full cone of movement | Combined above |
Note: True glenohumeral abduction is 0-120°; the remaining 60° involves rotation of the scapula on the thorax (scapulothoracic rhythm, 2:1 ratio).
11. Blood Supply
Primarily from branches of the axillary artery:
- Anterior circumflex humeral artery - runs in front of the surgical neck
- Posterior circumflex humeral artery - passes through the quadrangular space with the axillary nerve
- Suprascapular artery - also contributes
The supraspinatus tendon has a relatively avascular zone near its insertion - the "critical zone" - making it susceptible to degeneration and tears.
12. Nerve Supply (Hilton's Law)
The glenohumeral joint is innervated by branches from the posterior cord of the brachial plexus and from:
- Suprascapular nerve (C5, C6) - posterior and superior capsule
- Axillary nerve (C5, C6) - anterior and inferior capsule
- Lateral pectoral nerve - anterior capsule
The axillary nerve is vulnerable in anteroinferior dislocation as it winds around the surgical neck in the quadrangular space.
13. Clinical Correlates
| Condition | Anatomy Involved |
|---|---|
| Anterior dislocation | Weak anteroinferior capsule, Bankart lesion (labral tear), possible Hill-Sachs lesion; axillary nerve injury |
| Posterior dislocation | Rare; associated with seizures/electrocution |
| Rotator cuff impingement | Supraspinatus compressed under coracoacromial arch; subacromial bursitis |
| Rotator cuff tear | Usually supraspinatus at its avascular zone |
| SLAP lesion | Superior labrum, anterior to posterior tear; involves biceps anchor |
| Frozen shoulder (adhesive capsulitis) | Contracted joint capsule, especially inferior recess and rotator interval |
| Biceps tendon dislocation | Disruption of biceps pulley (transverse humeral ligament + superior GHL) |
Sources:
- Gray's Anatomy for Students, 4th Ed., p. 826-831 (Glenohumeral Joint chapter)
- THIEME Atlas of Anatomy: General Anatomy and Musculoskeletal System, pp. 284-286 (Shoulder joint ligaments and subacromial space)
This is a shared conversation. Sign in to Orris to start your own chat.