Glaucoma basic to clinics
Reading File
Finding Sources
Searching PubMed
glaucoma pathophysiology treatment
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have everything needed for a comprehensive, image-rich response. Let me compile it:
Glaucoma: Basic to Clinics
1. Definition and Epidemiology
Glaucoma is a group of conditions sharing a common pathology: chronic progressive optic neuropathy resulting in characteristic morphological changes at the optic nerve head, retinal nerve fiber layer (RNFL), and progressive visual field loss. Intraocular pressure (IOP) is the key modifiable risk factor, but it is not the sole determinant of damage.
- Affects 2-3% of people over age 40; up to 50% may be undiagnosed
- Second leading cause of blindness worldwide
- Primary open-angle glaucoma (POAG) is the most common form in White, Hispanic/Latino, and African populations
- Risk factors: elevated IOP, older age, African ancestry, positive family history, myopia, low blood pressure, disc hemorrhages, thin central corneal thickness (CCT)
(Kanski's Clinical Ophthalmology, 10th ed.; Goldman-Cecil Medicine)
2. Aqueous Humor Dynamics - The Core Pathophysiology
Understanding glaucoma requires grasping how aqueous humor is produced and drained:
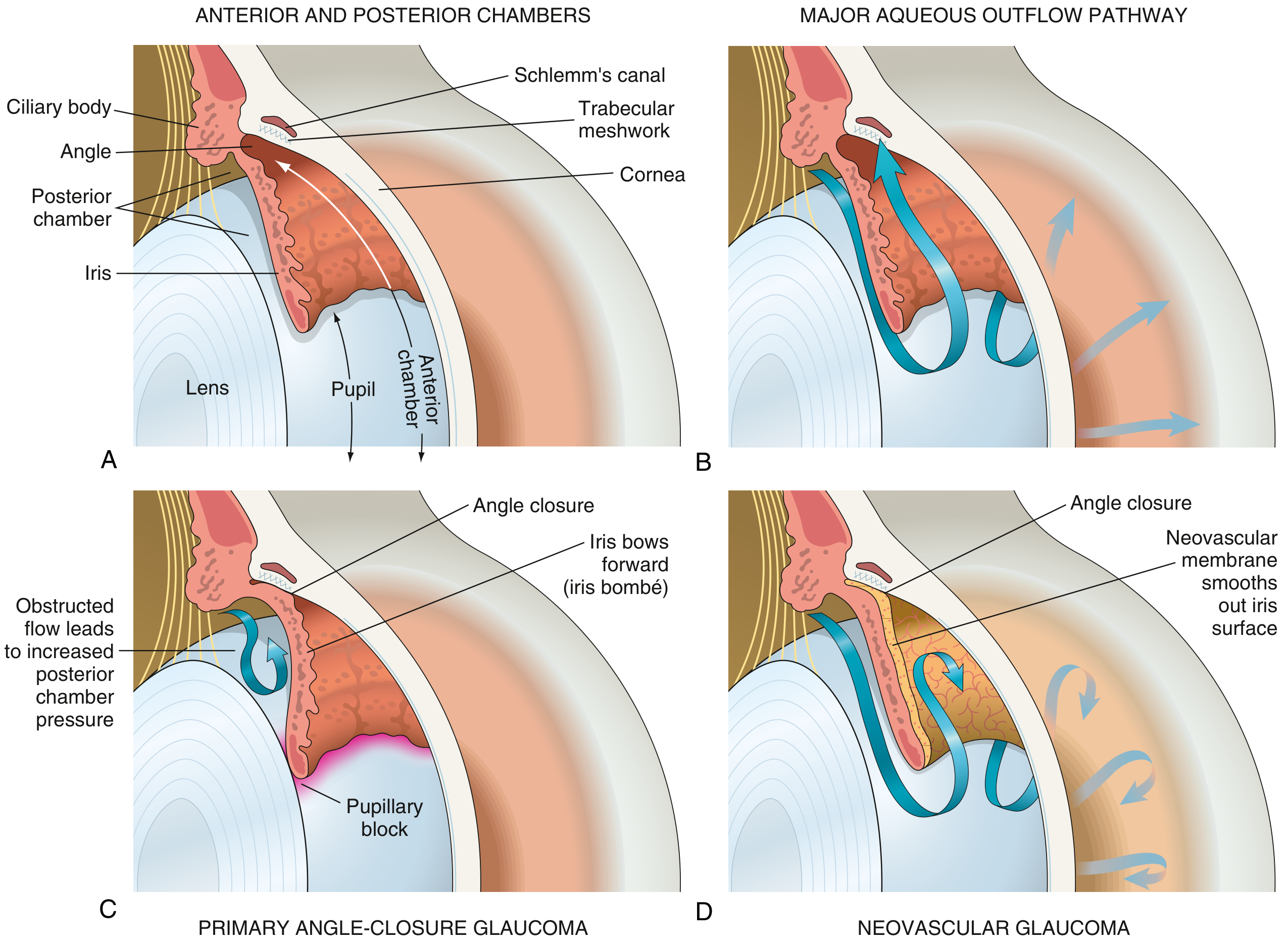
Fig. 21.38 - Robbins & Kumar Basic Pathology: (A) Eye anatomy, (B) Normal aqueous flow, (C) Angle-closure with iris bombé, (D) Neovascular glaucoma
Production: Aqueous humor is produced by the non-pigmented ciliary epithelium of the pars plicata of the ciliary body (posterior chamber). It flows through the pupil into the anterior chamber.
Drainage (two pathways):
- Trabecular (conventional) pathway (~70-90%): through the trabecular meshwork → Schlemm's canal → episcleral veins. This is the pressure-sensitive pathway.
- Uveoscleral (unconventional) pathway (~10-30%): across the ciliary body face into the supraciliary and suprachoroidal spaces
If drainage does not match production, IOP rises. Normal IOP is defined statistically as ≤21 mmHg (population mean + 2 SD). However, no IOP is fully protective, and some patients develop glaucoma despite statistically normal IOP (normal-tension glaucoma, NTG).
(Robbins & Kumar Basic Pathology; Goodman & Gilman's)
3. Classification
GLAUCOMA
├── PRIMARY
│ ├── Primary Open-Angle Glaucoma (POAG) — most common
│ ├── Primary Angle-Closure Glaucoma (PACG)
│ └── Normal-Tension Glaucoma (NTG)
├── SECONDARY
│ ├── Secondary Open-Angle (pseudoexfoliation, pigmentary, steroid-induced,
│ │ neovascular after retinal ischemia, traumatic)
│ └── Secondary Angle-Closure (neovascular, inflammatory, phacomorphic,
│ phacolytic, malignant glaucoma)
└── CONGENITAL / DEVELOPMENTAL
├── Primary congenital (buphthalmos)
└── Associated (Sturge-Weber, NF1, aniridia)
4. Pathogenesis of Optic Nerve Damage
The primary site of damage is the lamina cribrosa, where axons of the optic nerve exit the eye. Two mechanisms operate, often together:
- Direct mechanical damage - elevated IOP compresses axons passing through the lamina cribrosa, causing physical deformation of the laminar plates and impeding axoplasmic flow
- Ischemic damage - compression of blood vessels supplying the optic nerve head reduces perfusion (ocular perfusion pressure = mean arterial pressure - IOP)
Cellular cascade:
- Retinal ganglion cell (RGC) death occurs via apoptosis (programmed cell death), not necrosis
- The triggering event involves calcium ion influx into the cell body and increased intracellular nitric oxide
- Glutamine metabolism is intrinsically involved
- A secondary cascade follows: astrocyte and glial cell proliferation, extracellular matrix alterations at the lamina cribrosa, and optic nerve head remodelling
- Loss of axons leads to enlargement of the optic cup - recorded clinically as an increased cup-to-disc (C:D) ratio
(Kanski's Clinical Ophthalmology)
5. Primary Open-Angle Glaucoma (POAG)
The most common type, especially in the elderly. Defined by an open, anatomically normal-appearing anterior chamber angle with evidence of trabecular dysfunction causing outflow resistance.
Clinical features
- Asymptomatic until late - peripheral visual fields may be reduced considerably before the patient notes any functional loss
- First symptoms: difficulty reading, reduced contrast sensitivity, or glare
- Most cases detected during routine eye examination - elevated IOP or high C:D ratio
Diagnosis requires all of:
- Elevated IOP (or progressive nerve damage despite normal IOP in NTG)
- Characteristic optic disc changes (see below)
- Visual field defects on automated perimetry
- Open angle on gonioscopy
Optic disc changes in glaucoma
Four morphological patterns are described:
| Pattern | Features | Associated VF Loss |
|---|---|---|
| Focal ischaemic | Localized superior/inferior notching of neuroretinal rim | Localized defects threatening fixation early |
| Myopic disc | Tilted oblique disc, temporal crescent of parapapillary atrophy | Dense superior/inferior scotomas |
| Sclerotic | Shallow saucerized cup, gently sloping NRR | Peripheral VF loss; older patients |
| Concentrically enlarging | Uniform NRR thinning | Diffuse VF loss; high IOP at presentation |
Other signs of glaucomatous damage:
- Disc haemorrhages (splinter haemorrhages extending from the NRR onto the retina, most commonly inferotemporally) - these are a risk factor for progression
- RNFL defects (wedge-shaped defects on red-free photography) - these precede optic disc and visual field changes
Visual field defects (automated perimetry)
- Test area most commonly used: 24-2 or 30-2 pattern (30° radius from fixation)
- 10-2 for central field monitoring in advanced disease
- Classic patterns: nasal step, arcuate (Bjerrum) scotoma, paracentral scotoma, and ultimately tunnel vision
Genetics
- Mutations in MYOCILIN (MYOC) - most common, accounts for ~4% of POAG
- Other genes: OPTN (optineurin), NTF4, WDR36
- If a single family member develops glaucoma before age 35, the chances of a MYOC mutation may be as high as 33%
- Polygenic risk scores (PRS) are now being developed to predict susceptibility
(Kanski's Clinical Ophthalmology, 10th ed.)
6. Primary Angle-Closure Glaucoma (PACG)
Mechanism (pupillary block)
Risk factors stem from the anatomical configuration of the anterior chamber:
- Hyperopia - shortened anterior-posterior axis, shallow anterior chamber
- As the crystalline lens enlarges with age, the iris is displaced anteriorly
- Posterior iris surface comes in tight contact with the anterior lens surface
- Aqueous accumulates in the posterior chamber → iris bombé (forward bowing of peripheral iris)
- Peripheral iris occludes the trabecular meshwork → sudden IOP rise
Acute angle-closure attack
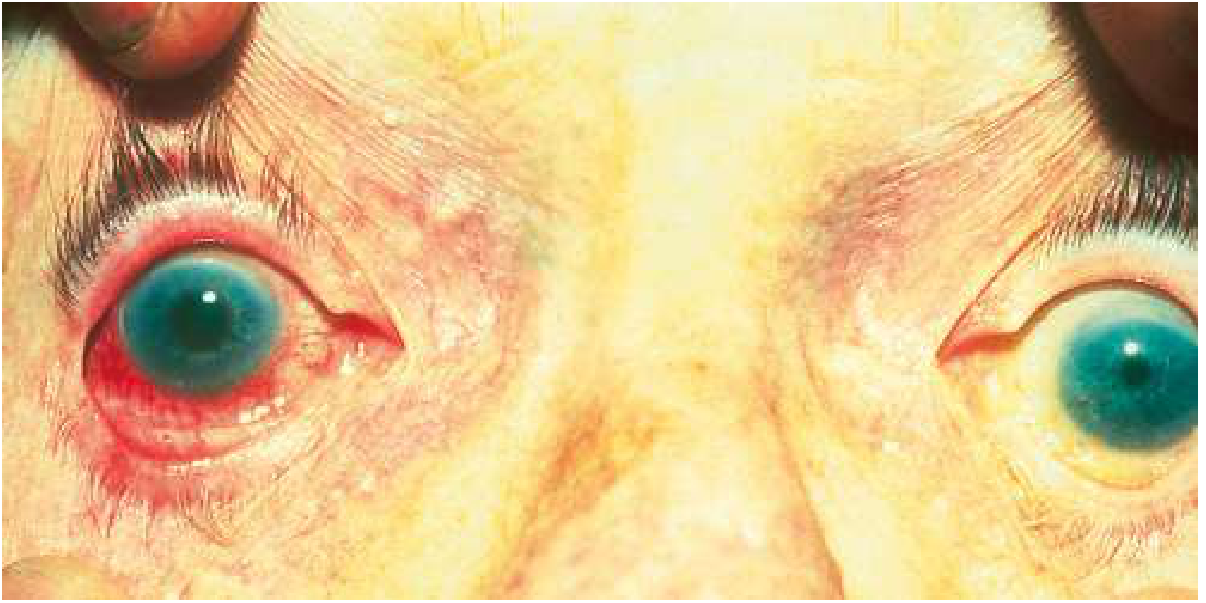
Acute angle-closure glaucoma: The right eye is red with a nonreactive, mid-dilated pupil compared to the normal left eye.
Clinical triad:
- Severe eye pain (may radiate and be poorly localized), headache, nausea/vomiting (can mimic acute abdomen)
- Blurred vision with halos around lights
- Red eye with mid-dilated, non-reactive pupil, corneal oedema (cloudy cornea), shallow anterior chamber
IOP can exceed 60 mmHg - nearly equaling diastolic arterial pressure.
Precipitants: Pharmacologic pupillary dilation, dim lighting (physiological dilation), sympathomimetic or anticholinergic drugs
Immediate management:
- Topical IOP-lowering drops: beta-blocker (timolol 0.5%), alpha-agonist (apraclonidine), pilocarpine
- Systemic: acetazolamide 250-500 mg IV (or oral if IV unavailable)
- Hyperosmotic agents (mannitol IV) in severe cases
- Laser peripheral iridotomy (LPI) - definitive treatment; creates a fistula bypassing pupillary block
- Prophylactic LPI to the fellow eye (high risk of attack)
- Lens extraction is an additional option (age-related lens growth contributes to angle closure)
(Goldman-Cecil Medicine; Kanski's Clinical Ophthalmology)
7. Normal-Tension Glaucoma (NTG)
- Progressive glaucomatous optic neuropathy with IOP consistently ≤21 mmHg
- Mechanism: vascular insufficiency, increased susceptibility of the optic nerve to ischemia, autoimmune processes
- More common in Japanese patients and in women
- Associated with vasospastic conditions (Raynaud's, migraine), systemic hypotension
- Management: IOP reduction (prostaglandins preferred) and addressing vascular risk factors
8. Secondary Glaucomas
Pseudoexfoliation Glaucoma
- Most common form of secondary open-angle glaucoma globally
- Fibrillin gene mutation → abnormal fibrillogranular material deposits on the lens capsule, iris, trabecular meshwork
- Especially prominent in Scandinavians and Arabs
- Higher IOP spikes, more difficult to control
- Treatment as for POAG but often requires surgery sooner
Pigmentary Glaucoma
- Pigment granules from the iris pigment epithelium deposit in the trabecular meshwork
- Young myopic males; Krukenberg spindle on corneal endothelium
- Scheie line on trabecular meshwork; iris transillumination defects
Neovascular Glaucoma
- New vessels (driven by VEGF upregulation from chronic retinal ischemia, e.g., PDR, CRVO) grow over the iris surface and angle
- Myofibroblasts in the neovascular membrane contract, creating peripheral anterior synechiae (PAS), obliterating the angle
- Causes: diabetic retinopathy, central retinal vein occlusion, ocular ischemic syndrome
- Very difficult to manage; anti-VEGF injections + aggressive IOP lowering
Steroid-Induced Glaucoma
- Secondary open-angle glaucoma from topical, periocular, inhaled, or systemic glucocorticoids
- Without a family history of glaucoma: ~5% of normal individuals show marked IOP rise
- With a positive family history: up to 90% may develop moderate-to-marked IOP elevation
- Risk is reduced but not eliminated with loteprednol (a soft steroid)
(Goodman & Gilman's; Robbins & Kumar)
9. Gonioscopy and Angle Assessment
Gonioscopy is mandatory in all glaucoma patients to classify angle anatomy:
Shaffer grading system:
| Grade | Angle | Clinical significance |
|---|---|---|
| 4 | 35-45° | Wide open, closure impossible |
| 3 | 25-35° | Open, closure unlikely |
| 2 | 20° | Narrow, possible closure |
| 1 | <10° | Very narrow, high closure risk |
| 0 | 0° | Closed; synechiae present |
Van Herick test (slit lamp estimation): compares anterior chamber depth to corneal thickness at the limbus.
10. Investigations
| Investigation | Purpose |
|---|---|
| Goldmann applanation tonometry | Gold standard for IOP measurement |
| Pachymetry (CCT measurement) | Corrects IOP for corneal thickness; thin cornea = underestimated IOP |
| Automated perimetry (Humphrey) | Visual field assessment (24-2 routine; 10-2 for advanced) |
| OCT (posterior segment) | RNFL thickness, macular ganglion cell complex |
| OCT anterior segment | Angle anatomy in PACG |
| Ultrasound biomicroscopy (UBM) | Behind-iris anatomy (ciliary body, lens) |
| Optic disc photography / HRT | Baseline documentation, progression monitoring |
| Gonioscopy | Direct angle visualisation |
11. Medical Treatment
Drug Classes and Mechanisms
| Drug Class | Examples | Mechanism | Key Side Effects |
|---|---|---|---|
| Prostaglandin analogues | Latanoprost 0.005%, travoprost 0.004%, bimatoprost, tafluprost | Increase uveoscleral outflow | Iris/periocular pigmentation, hypertrichosis, CME (aphakic) |
| Beta-blockers | Timolol 0.5% (non-selective), betaxolol (selective β1) | Decrease aqueous production | Bradycardia, bronchospasm, fatigue. CI: asthma, COPD, heart block |
| Alpha-2 agonists | Brimonidine 0.2%, apraclonidine | Decrease production + increase uveoscleral outflow | Allergy, drowsiness, dry mouth. CI in infants (apnoea) |
| Carbonic anhydrase inhibitors | Dorzolamide (topical), brinzolamide, acetazolamide (systemic) | Decrease aqueous production | Topical: stinging, metallic taste. Systemic: metabolic acidosis, renal calculi, paraesthesiae, sulfonamide allergy |
| Rho-kinase (ROCK) inhibitors | Netarsudil 0.02% | Increase trabecular outflow; decrease episcleral venous pressure | Conjunctival hyperemia, subconjunctival haemorrhage, cornea verticillata |
| Miotics (cholinergics) | Pilocarpine 1-4% | Increase trabecular outflow (ciliary muscle contraction opens meshwork) | Brow ache, miosis, myopia, retinal detachment risk |
| Combination | Latanoprost + netarsudil (Rocklatan), timolol + dorzolamide, timolol + brimonidine | Dual mechanism | Combined profiles |
First-line therapy: Prostaglandin analogues (once daily, maximum IOP reduction ~25-35%) or selective laser trabeculoplasty (SLT).
(Goodman & Gilman's; Goldman-Cecil Medicine)
Recent evidence (2025): A network meta-analysis (PMID 40701331, Ophthalmology 2025) found prostaglandin analogues remain the most effective single agents, with combination therapy providing additive reduction.
12. Laser Treatment
Selective Laser Trabeculoplasty (SLT)
- Uses 532 nm Nd:YAG laser, selectively targets pigmented trabecular meshwork cells
- Increases trabecular outflow via macrophage and cytokine-mediated remodelling
- Can be considered first-line therapy - repeatable, no medication side effects
- Recent meta-analysis (PMID 39018052, J Glaucoma 2024) confirms SLT is equivalent to medical therapy in reducing IOP at 36 months
Argon Laser Trabeculoplasty (ALT)
- Older technique; creates thermal burns on trabecular meshwork; limited repeatability
Laser Peripheral Iridotomy (LPI)
- Nd:YAG laser creates a hole in peripheral iris
- Definitive treatment for angle-closure; prophylactic in the fellow eye
Diode Laser Cyclodestruction (cycloablation)
- Reduces aqueous production by ablating ciliary body
- Reserved for refractory glaucoma or eyes with poor visual potential
13. Surgical Treatment
Trabeculectomy
- Gold standard filtering surgery
- Creates a fistula (bleb) from anterior chamber to subconjunctival space
- Augmented with mitomycin C (MMC) or 5-fluorouracil (5-FU) to reduce bleb scarring
- Complications: hypotony, bleb leak, endophthalmitis, cataract
Glaucoma Drainage Devices (Tube-Shunts)
- Ahmed, Baerveldt, Molteno implants
- Tube drains aqueous to an equatorial reservoir
- Used in failed trabeculectomy, neovascular glaucoma, uveitic glaucoma
- A 2025 meta-analysis (PMID 39394492) found the PreserFlo MicroShunt has comparable IOP reduction to trabeculectomy with fewer early hypotony complications
Minimally Invasive Glaucoma Surgery (MIGS)
- iStent, Hydrus, KDB goniotomy, OMNI, XEN gel stent
- Lower risk profile; suitable for mild-to-moderate glaucoma combined with cataract surgery
- Less IOP reduction than trabeculectomy but better safety
14. Monitoring and Progression
Target IOP: Set individually based on:
- Baseline IOP, extent of damage, age, life expectancy
- A 20-30% reduction from baseline is typically the starting target
- May need to be lowered further if progression continues
Progression assessment:
- Visual field: Event-based (comparing to baseline) or trend-based analysis
- RNFL OCT: Objective, detects change before field loss
- Disc photography: Document structural changes
Ocular Hypertension Treatment Study (OHTS): Untreated OHT had a 9.5% cumulative 5-year risk of developing POAG. Treatment reducing IOP by ≥20% lowered this to 4.4%.
15. Special Situations
Congenital/Developmental Glaucoma
- Primary congenital: Trabeculodysgenesis; presents at birth or within first year; buphthalmos (ox eye), Haab's striae, photophobia, epiphora
- Surgery (goniotomy or trabeculotomy) is first-line, not medical treatment
- Sturge-Weber syndrome: Glaucoma in ~30% ipsilateral to facial haemangioma; glaucoma drainage devices offer best IOP control
- Aniridia (PAX6 gene): Glaucoma drainage devices are treatment of choice
Glaucoma in Pregnancy
- Beta-blockers: may cross placenta; neonatal bradycardia
- Brimonidine: avoid (crosses blood-brain barrier, causes neonatal apnoea)
- Carbonic anhydrase inhibitors: teratogenic (avoid in first trimester)
- Prostaglandins: avoid (uterotonic)
- Safest option: topical beta-blocker (with nasolacrimal occlusion) under specialist supervision; surgery preferred over systemic CAIs
Normal-Tension vs. High-Tension POAG
- Both treated by IOP reduction - IOP lowering is beneficial even in NTG
- In NTG, prostaglandins + addressing vascular risk factors (nocturnal hypotension, vasospasm)
Summary: The Glaucoma "Big Picture"
Impaired aqueous outflow (or ↑ production)
↓
Elevated IOP
↓
Mechanical + ischemic injury at lamina cribrosa
↓
Retinal ganglion cell apoptosis
↓
RNFL thinning → optic disc cupping → visual field loss
↓
Blindness (if untreated)
GOAL: Lower IOP to a target that halts or slows progression
throughout the patient's lifetime
Sources:
- Kanski's Clinical Ophthalmology: A Systematic Approach, 10th ed. (Chapters 11 and related)
- Robbins & Kumar Basic Pathology, p. 868-870
- Goodman & Gilman's The Pharmacological Basis of Therapeutics, Chapter 74
- Goldman-Cecil Medicine, Chapter 391
- PMID 39018052 - SLT vs. Medical Therapy meta-analysis (J Glaucoma, 2024)
- PMID 39394492 - PreserFlo vs. Trabeculectomy meta-analysis (2025)
- PMID 40701331 - Glaucoma medication network meta-analysis (Ophthalmology, 2025)
Ece
Asking for Preferences
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.