Detail about lymph nodes and metastasis of unknown origin from stell n marans textbook
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive content. Let me compile the full answer.
Note on source: Stell & Maran's Head and Neck Surgery is not among the textbooks in this library. The information below is drawn from the closest equivalent authoritative ENT references available — Cummings Otolaryngology: Head and Neck Surgery and Goldman-Cecil Medicine — which cover this topic comprehensively and are the standard references for this content.
Lymph Nodes and Metastasis of Unknown Primary (MUP) — Head & Neck
1. Definition
An unknown primary (also called carcinoma of unknown primary, CUP) in the neck is a squamous cell carcinoma (SCC) identified within the cervical lymphatic structures without an identifiable primary tumor site. The patient typically presents with a neck mass that is histologically proven to be metastatic SCC, despite exhaustive workup failing to reveal the source.
2. Initial Evaluation
Clinical presentation
- Neck mass, usually painless, is the presenting feature
- Diagnosed histologically by fine needle aspiration (FNA) biopsy
- FNA tissue should be sampled for p16 immunohistochemistry or HPV testing — positivity strongly suggests an oropharyngeal (tonsillar or base of tongue) primary, and less commonly nasopharyngeal
History and examination
- A thorough head and neck examination of the entire upper aerodigestive tract is mandatory
- Smoking and alcohol history are relevant (traditional SCC risk) — but HPV-positive tumors increasingly occur in non-smokers
Endoscopy
- Operative endoscopy with directed biopsies of the most common occult primary sites:
- Nasopharynx
- Base of tongue
- Palatine tonsil
- Piriform sinus
- The primary is usually found at this step; if excisional biopsy was performed first, intraoperative directed biopsies of these sites should be done simultaneously
3. Role of Lymph Node Level in Localizing the Primary
The level of the metastatic cervical lymph node directs the clinician to the most likely primary site, based on well-established lymphatic drainage routes:
| Node Level | Likely Primary Site |
|---|---|
| Level I | Oral cavity |
| Level II, III | Oral cavity, oropharynx, hypopharynx, larynx |
| Level IV | Hypopharynx, larynx, subglottis |
| Level V | Nasopharynx (especially posterior triangle) |
| Supraclavicular | Esophagus, lung, abdominal/pelvic primaries |
This anatomic mapping is foundational — the level of the neck mass is the first clue to occult primary location.
4. Imaging
When clinical examination and endoscopy fail to reveal the primary:
- CT and MRI are used first
- ¹⁸F-FDG PET/CT (fused) is the most useful modality: in 190 patients with unknown primary lesions, PET/CT showed a sensitivity of 62% and specificity of 81.9% in identifying the primary site
- PET/CT can identify a primary head and neck lesion in approximately 25% of endoscopy-negative patients
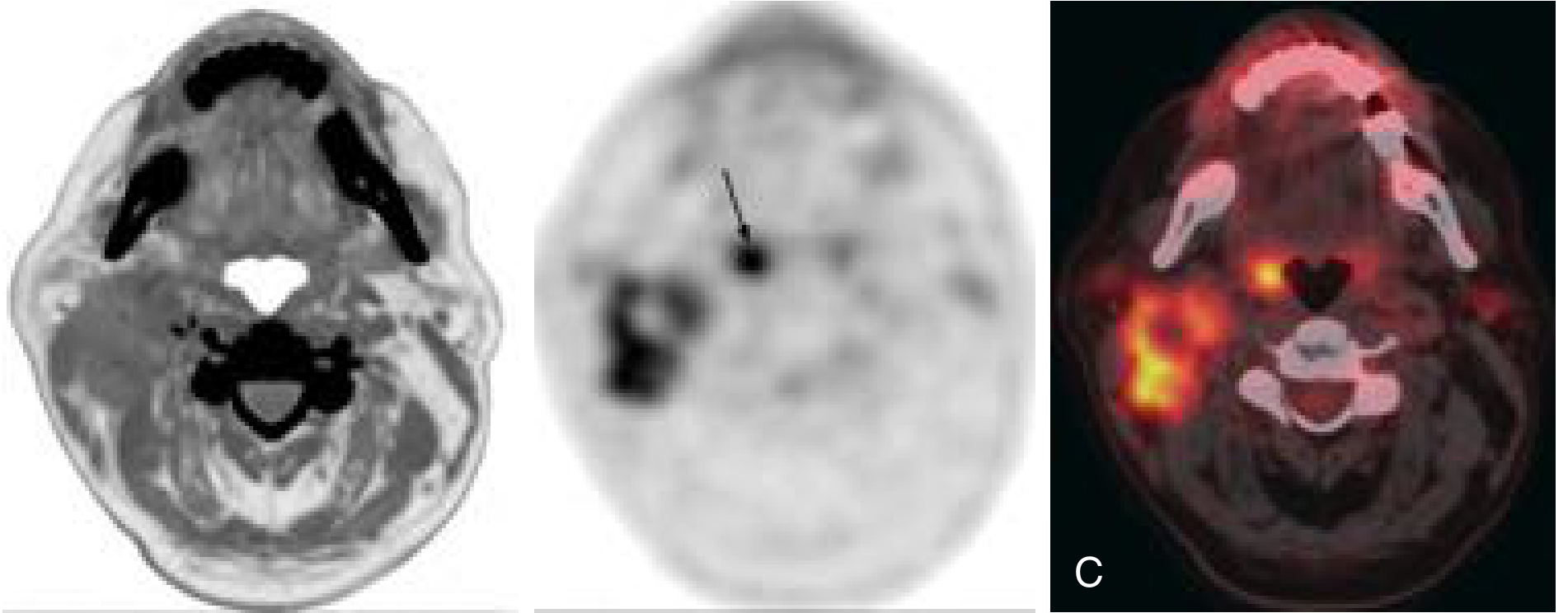
Fig. 115.7: Unknown primary. (A) Non-enhanced axial CT from PET/CT showing large heterogeneous Level II lymph nodes. (B) Corresponding ¹⁸F-FDG PET showing increased metabolic activity in nodes and another focus (arrow). (C) Fused PET/CT clearly demonstrates high metabolic activity in the right palatine tonsil and metastatic nodes. — Cummings Otolaryngology
5. HPV-Positive Unknown Primary: Modern Surgical Workup
With the rise of HPV-driven oropharyngeal cancer, a structured approach (Hatten protocol) has emerged for HPV/p16-positive unknown primaries:
- If HPV positive with no primary on exam or imaging → Direct laryngoscopy
- If still no primary → Ipsilateral palatine tonsillectomy with frozen section
- Positive for SCC → treat with staged TORS + neck dissection or definitive chemoradiation
- If tonsillectomy negative → Ipsilateral base-of-tongue resection (TORS) — diagnostic and therapeutic
Using this regimented approach, 80–90% of unknown primaries are ultimately identified.
6. Management by Histology
Squamous Cell Carcinoma (most common)
- Neck dissection should not be undertaken until all efforts to identify the primary are exhausted (treatment depends on primary location)
- Once workup is complete:
- Concurrent chemoradiotherapy — standard for locally advanced SCC of unknown primary
- 5-year disease-free survival: 50–60%
- Adverse prognostic features:
- Node >2 cm
- Multiple involved lymph nodes
Melanoma of Unknown Primary
- Accounts for 2–3% of all melanoma presentations
- Possible mechanisms: small primary missed, immune regression, or origin from ectopic melanocytes in a lymph node
- Better prognosis than stage-matched melanoma with a known primary (improved immune response)
- Treatment: comprehensive neck dissection + adjuvant radiation and/or immunotherapy
- Ongoing dermatologic surveillance is mandatory
7. Regional Metastases from Other Sites
When FNA shows histologies other than SCC, consider:
| Histology / Staining Clue | Suspected Primary |
|---|---|
| Adenocarcinoma + thyroglobulin / PAX8 / TTF-1 positive | Thyroid carcinoma |
| Adenocarcinoma + negative thyroid markers, Level I–III | Salivary gland neoplasm |
| Adenocarcinoma, Level IV–V | Infraclavicular primary (lung, esophagus, kidney, ovary, cervix, prostate) |
| Elevated PSA / blastic bone mets | Prostate cancer |
8. Distant Metastases to the Neck
Common distant primary sites that metastasize to the neck include:
- Lung, esophagus (supraclavicular nodes)
- Kidney, ovary, cervix, prostate
Hundreds of neoplasms can metastasize to the neck; the Level IV–V / supraclavicular location should always prompt consideration of subdiaphragmatic or thoracic primaries.
9. Cancer of Unknown Primary — Broader Subsets (Goldman-Cecil Framework)
| Histology | Clinical Setting | Management |
|---|---|---|
| Adenocarcinoma | Women with isolated axillary adenopathy | Treat as Stage II breast cancer |
| Adenocarcinoma / poorly differentiated | Women with peritoneal carcinomatosis | Treat as Stage III ovarian cancer |
| Adenocarcinoma | Men with elevated PSA or blastic bone mets | Treat as advanced prostate cancer |
| Adenocarcinoma / poorly differentiated | Single metastatic lesion | Definitive local therapy ± chemotherapy |
| Adenocarcinoma | Colon cancer profile (CK20+, CK7−, CDX-2+) | Treat as metastatic colorectal cancer |
| SCC | Cervical adenopathy | Treat as locally advanced H&N cancer |
| SCC | Inguinal adenopathy (perineal/anorectal) | Inguinal dissection ± RT; platinum-5-FU chemoRT |
| Poorly differentiated carcinoma | Young men, mediastinal/retroperitoneal | Treat as extragonadal germ cell tumor (BEP) |
| Poorly differentiated carcinoma | Neuroendocrine features | Treat as neuroendocrine carcinoma |
Sources:
- Cummings Otolaryngology: Head and Neck Surgery, Chapter 115 (Malignant Neoplasms of the Neck / Unknown Primary / Metastatic Lesions), pp. 2229–2231
- Goldman-Cecil Medicine, Chapter 164 (Cancer of Unknown Primary Origin) / Chapter 176 (Cervical Adenopathy), pp. 1889–1890
In detail about lymph nodes...anatomy physiology
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive content from multiple textbooks. Let me compile the full, detailed answer.
Lymph Nodes — Detailed Anatomy & Physiology
1. Overview and General Features
Lymph nodes are small, bean-shaped, encapsulated secondary lymphoid organs interposed along lymphatic vessels throughout the body. They range from approximately 1 mm to 1–2 cm in their longest dimension. A total of 400–450 lymph nodes are distributed throughout the body, concentrated in the:
- Axillae (armpits)
- Inguinal (groin) regions
- Cervical (neck) regions
- Thorax, abdomen, and visceral mesenteries
They serve as in-line filters of lymph before it merges with the bloodstream. All lymph is filtered by at least one lymph node, which also adds antibodies to it.
Primary functions:
- Filter lymph and trap microorganisms, foreign particles, and tumor cells
- Provide enclosed environments for antigen presentation
- Generate adaptive immune responses (B- and T-cell activation, antibody production)
2. Gross Anatomy
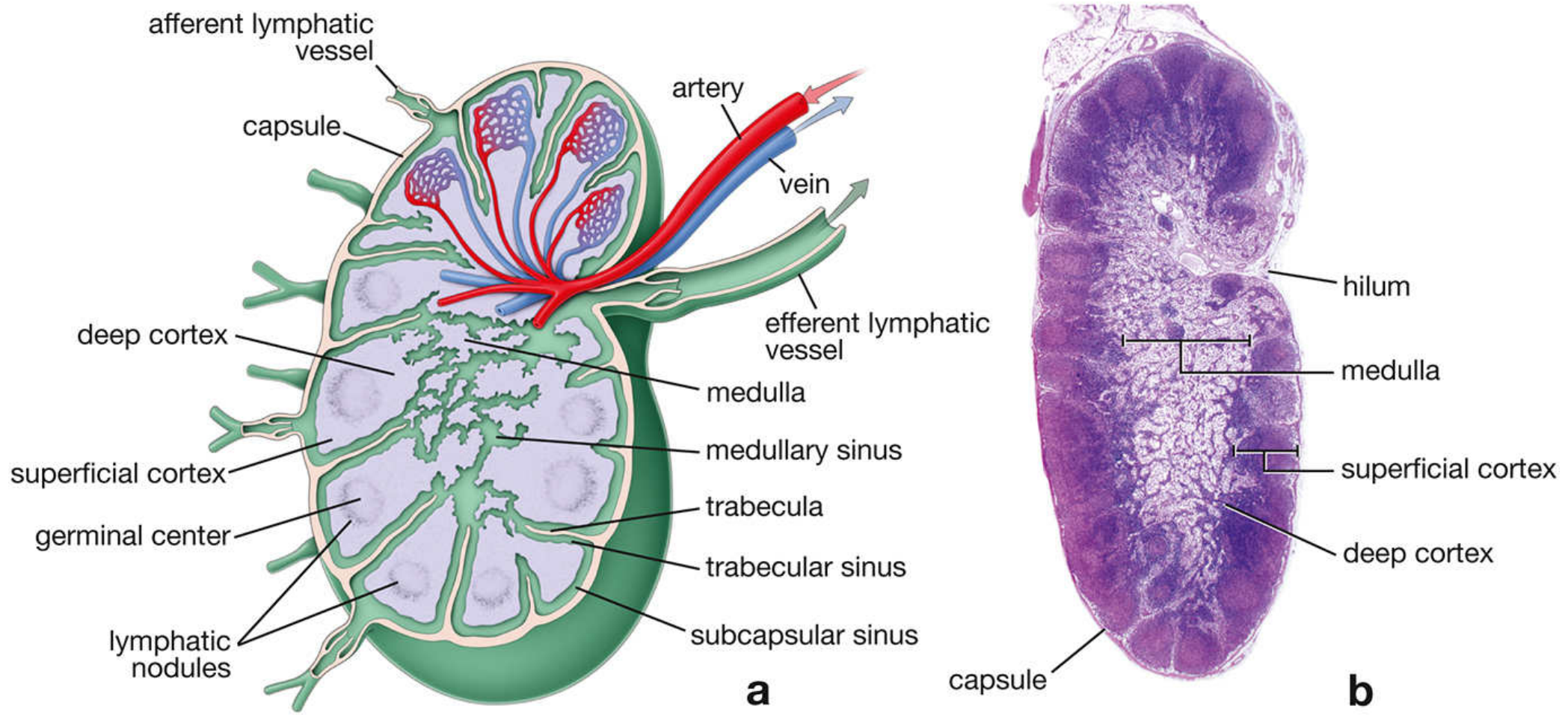
Each lymph node has:
- A convex surface where multiple afferent lymphatics enter
- A concave depression (hilum) where a single efferent lymphatic exits, along with the artery, vein, and nerve
Lymph flow is unidirectional, ensured by valves in the lymphatic vessels — afferent → subcapsular sinus → trabecular sinuses → medullary sinuses → efferent.
3. Supporting Framework
| Component | Composition | Function |
|---|---|---|
| Capsule | Dense connective tissue | Surrounds and protects the node |
| Trabeculae | Dense CT extensions from capsule | Internal scaffolding; carry blood vessels |
| Reticular tissue | Reticular cells + type III collagen (reticulin) fibers | Fine supportive meshwork throughout parenchyma |
Reticular cells are fibroblast-like cells that synthesize reticulin fibers, wrap their processes around them, and produce chemokines that attract lymphocytes and dendritic cells.
4. Histological Regions
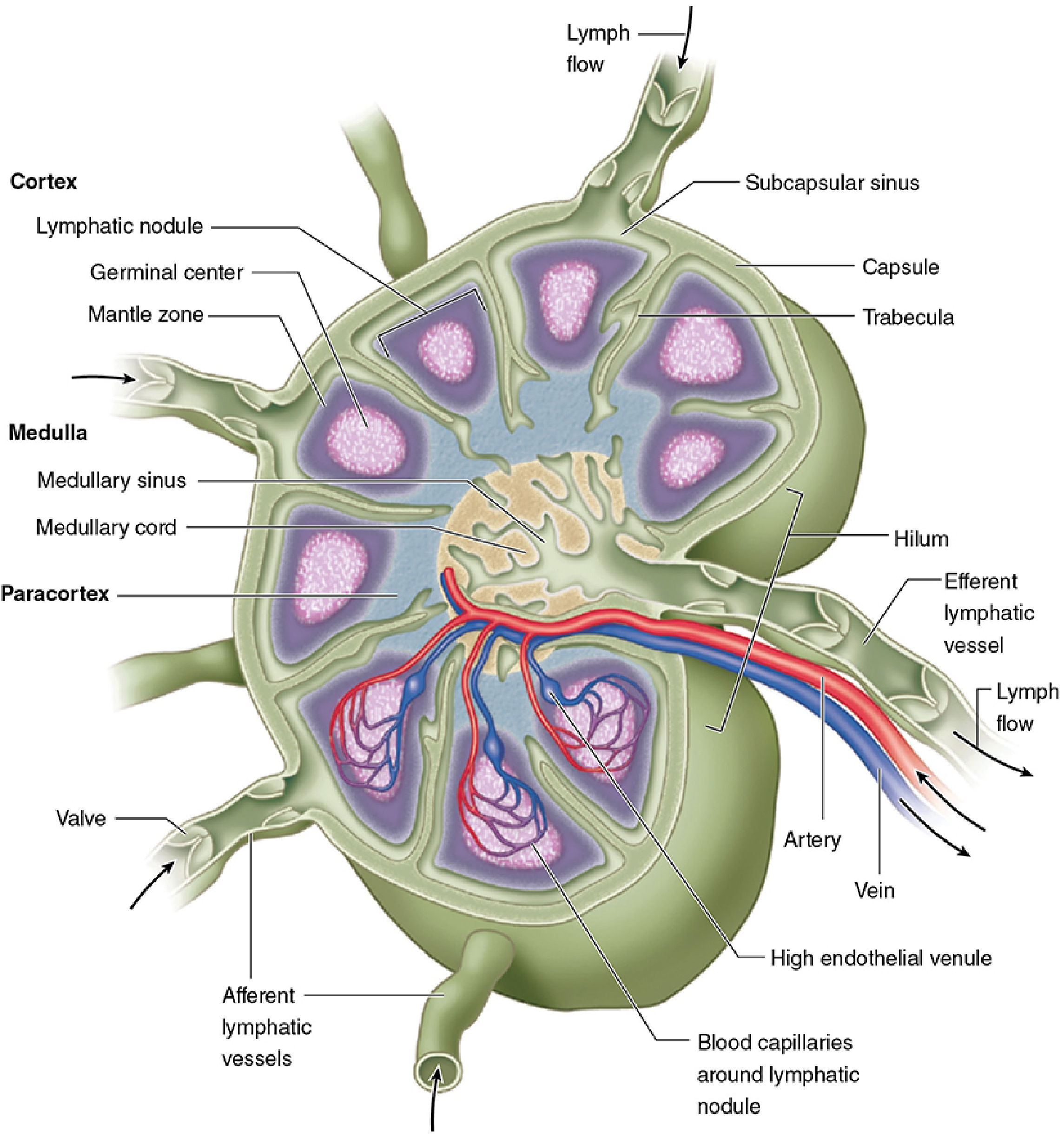
The lymph node parenchyma is organized into three major regions:
A. Cortex (Superficial / Nodular Cortex)
- The outermost zone, directly beneath the capsule
- Contains lymphoid nodules — the hallmark of the cortex:
- Primary nodules: dense, uniform small lymphocytes; no germinal center (resting state)
- Secondary nodules: contain a germinal center (pale-staining center surrounded by a dark mantle zone) — indicate active humoral immune response
- Predominantly B-cell zone — B cells and follicular dendritic cells (FDCs) dominate
- Subcapsular (cortical) sinus: space immediately beneath the capsule; receives lymph from afferent lymphatics; lined by discontinuous endothelium perforated by reticulin fibers
- Trabecular (cortical) sinuses: branch internally from the subcapsular sinus alongside trabeculae; lymph percolates from these into surrounding lymphoid tissue
B. Paracortex (Deep Cortex)
- Zone between superficial cortex and medulla
- No lymphoid nodules — distinguishes it from the cortex
- Predominantly T-cell zone — T lymphocytes dominate, especially CD4⁺ T helper cells
- Also called thymus-dependent cortex — neonatal thymectomy causes a poorly developed paracortex
- Contains High Endothelial Venules (HEVs) — the critical entry point for circulating lymphocytes from blood (see below)
- Dendritic cells (DCs) are concentrated here to present antigens to T cells
C. Medulla
Contains two components:
| Structure | Contents | Function |
|---|---|---|
| Medullary cords | T and B lymphocytes, plasma cells, macrophages, DCs | Antibody secretion; immune effector activity |
| Medullary sinuses | Macrophages, reticular cell meshwork, occasional neutrophils | Final filtration of lymph; convergence toward hilum |
- Medullary sinuses are continuous with cortical sinuses and converge at the hilum to drain into the single efferent lymphatic vessel
- The reticular meshwork within medullary sinuses forms a final filter for particulate matter
5. Cells of the Lymph Node
| Cell Type | Location | Key Function |
|---|---|---|
| B lymphocytes | Germinal centers, mantle zone, medullary cords | Antibody production; humoral immunity |
| T lymphocytes | Paracortex (deep cortex) | Cell-mediated immunity; help to B cells |
| Plasma cells | Medullary cords | Secrete antibodies (non-IgA) |
| Follicular Dendritic Cells (FDCs) | Germinal centers | Trap antigen–antibody complexes on surface for weeks–years; sustain B-cell selection |
| Dendritic cells (DCs) | Paracortex | Antigen presentation to T cells via MHC I and II; most efficient APCs |
| Macrophages | Medullary sinuses, subcapsular sinus | Phagocytosis; antigen presentation; remove apoptotic B cells from germinal centers |
| Reticular cells | Throughout stroma | Structural support; chemokine production |
6. High Endothelial Venules (HEVs)
HEVs are specialized postcapillary venules located in the paracortex. They are the primary route (≈90%) by which circulating lymphocytes enter the lymph node from the blood.
Mechanism of lymphocyte trafficking through HEVs:
- HEV endothelial cells are unusually cuboidal/enlarged (unlike flat venular endothelium)
- They express specific apical surface glycoproteins (addressins)
- L-selectin on lymphocytes recognizes sugar-rich ligands on HEV endothelial surfaces → lymphocytes slow and tether ("rolling")
- Integrins on lymphocytes bind adhesion molecules on HEVs → firm adhesion
- Lymphocytes undergo diapedesis (squeeze between endothelial cells) → enter the paracortex
This selective trafficking ensures naïve lymphocytes continuously sample lymph nodes for their cognate antigen.
7. Lymph Flow Through the Node
Afferent lymphatics (multiple, convex surface)
↓
Subcapsular sinus (beneath capsule)
↓
Trabecular (cortical) sinuses (alongside trabeculae)
↓
Medullary sinuses (between medullary cords)
↓
Efferent lymphatic (single, at hilum)
As lymph percolates through this system, it is exposed to APCs, macrophages, and lymphocytes — allowing antigen capture, processing, and immune activation at every level.
8. Blood Supply
- Artery enters at the hilum → branches along trabeculae → forms capillaries around nodules → HEVs in paracortex → post-capillary venules → vein exits at hilum
- HEVs represent the critical microvascular specialization for lymphocyte homing
9. Cervical Lymph Node Classification (Head & Neck)
The traditional head and neck classification includes 10 groups, condensed into Levels I–VII for clinical use:
| Level | Name | Location | Key Landmarks |
|---|---|---|---|
| Ia | Submental | Medial to anterior belly of digastric | |
| Ib | Submandibular | Lateral to digastric, around submandibular gland | |
| IIa/IIb | Upper internal jugular (jugulodigastric) | Skull base → inferior hyoid body | IIa: anterior to IJV; IIb: posterior/separate from IJV |
| III | Middle internal jugular | Inferior hyoid → inferior cricoid | |
| IV | Lower internal jugular | Inferior cricoid → clavicle | |
| Va/Vb | Spinal accessory / Transverse cervical | Posterior to SCM | Va: above cricoid; Vb: below cricoid |
| VI | Upper visceral (anterior compartment) | Between carotid arteries, hyoid → manubrium | Includes Delphian, pretracheal, paratracheal nodes |
| VII | Superior mediastinal | Below manubrium → innominate vein |
Nodes not included in the level classification: retropharyngeal, supraclavicular, and parotid nodes.
10. Physiological Functions
A. Filtration
- Lymph passing through the subcapsular and medullary sinuses is phagocytosed by macrophages
- Particulate matter (bacteria, debris, tumor cells) is trapped and degraded
- This prevents systemic dissemination of local infection
B. Antigen Presentation and Immune Activation
- Dendritic cells (most efficient APCs) capture antigen in peripheral tissues, migrate via afferent lymphatics, and present processed peptides on MHC II to naïve CD4⁺ T cells in the paracortex
- B-cell activation occurs when antigen in the cortex is recognized by B cells → germinal center reaction
C. Germinal Center Reaction (B-cell physiology)
- Antigen-specific B cells encounter antigen (± T-cell help) → enter follicle
- Clonal expansion within the germinal center
- Somatic hypermutation of immunoglobulin V genes → generates B cells with diverse affinities
- Affinity maturation — only high-affinity clones survive (selected by FDCs retaining antigen)
- Class-switch recombination → IgM → IgG, IgA, IgE
- B cells differentiate into long-lived plasma cells (migrate to medullary cords or bone marrow) or memory B cells
D. T-Cell Priming
- Naïve T cells enter via HEVs → scan paracortical DCs → if cognate antigen is found:
- CD4⁺ cells differentiate into Th1, Th2, Th17, or T_fh (follicular helper) cells
- CD8⁺ cells differentiate into cytotoxic T lymphocytes (CTLs)
- Activated T cells exit via the efferent lymphatic → thoracic duct → bloodstream → target tissues
E. Lymph Node Enlargement (Lymphadenopathy)
Enlargement results from:
- Reactive/Inflammatory: cellular proliferation in response to antigen (most common in children/young adults)
- Neoplastic infiltration: primary (lymphoma) or secondary (metastatic carcinoma)
- Deposition: foreign substances, storage diseases
Reactive nodes on imaging: typically <10 mm, central hilar enhancement, sharp margins, not clustered. Malignant nodes: >10 mm short axis, loss of fatty hilum, necrosis, extracapsular extension.
Sources:
- Histology: A Text and Atlas with Correlated Cell and Molecular Biology (Ross & Pawlina), pp. 1209–1220
- Junqueira's Basic Histology: Text and Atlas, 17e, pp. 704–710
- Cummings Otolaryngology: Head and Neck Surgery — Lymph Node Anatomy and Classification, pp. 183–185
- Goldman-Cecil Medicine — Lymphadenopathy, p. 1771
This is a shared conversation. Sign in to Orris to start your own chat.