Hypercalemia treatment
Reading File
Finding Sources
Searching PubMed
"hyperkalemia" AND "treatment"
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive overview of hyperkalemia treatment, organized by urgency.
Hyperkalemia Treatment
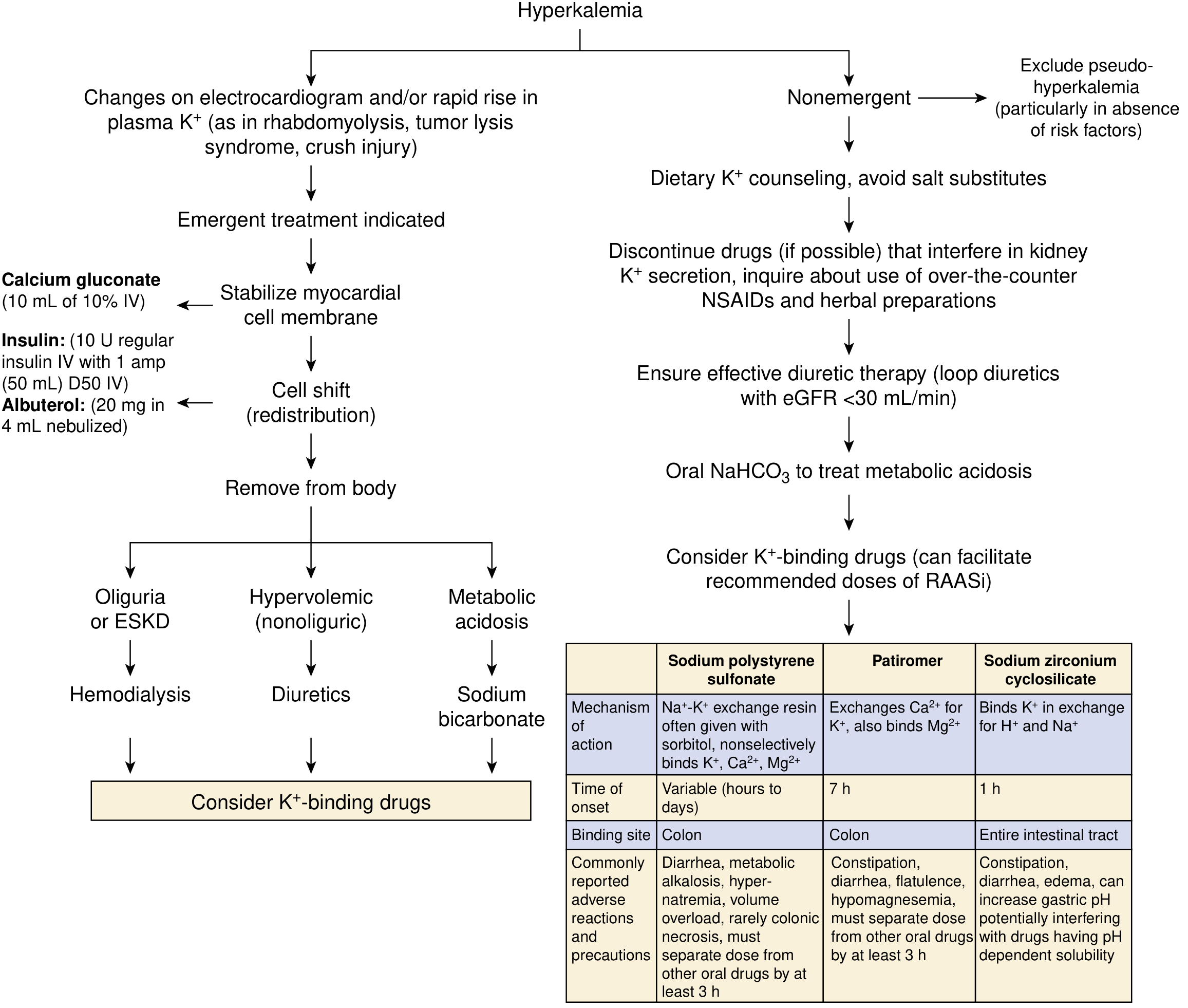
Step 1 — Stabilize the Cardiac Membrane
Indication: K⁺ > 6–6.5 mEq/L or any ECG changes (peaked T waves, widened QRS, loss of P waves)
| Agent | Dose | Onset | Notes |
|---|---|---|---|
| Calcium gluconate 10% | 10 mL IV over 1–3 min | Immediate | Repeat in 3–5 min if no ECG improvement. Does NOT lower K⁺. |
| Calcium chloride 10% | 3–5 mL IV | Immediate | More elemental Ca²⁺; avoid peripheral IV (risk of skin necrosis). Caution with digoxin (potentiates toxicity). |
First, stop all IV potassium infusions.
Step 2 — Shift K⁺ into Cells (Temporizing)
These lower plasma K⁺ within minutes to 1 hour but do not remove K⁺ from the body.
Insulin + Glucose
- Regular insulin 10 units IV + D50W 50 mL (1 amp) bolus, followed by D5W 100 mL/hr infusion to prevent late hypoglycemia
- Onset: ~15 minutes; peak at ~60 minutes
- Monitor glucose closely — hypoglycemia is common, especially in CKD (insulin half-life prolonged)
- If blood glucose >300 mg/dL (diabetics), insulin can be given without dextrose
- ⚠️ Never give dextrose alone — paradoxical K⁺ rise can occur if endogenous insulin is absent
Beta-2 Agonist (Albuterol)
- 20 mg nebulized over 10 minutes (use concentrated 5 mg/mL form)
- Onset: ~30 minutes
- Effect is additive to insulin
- IV albuterol (0.5 mg) available in Europe; not in the US
Sodium Bicarbonate
- 50–100 mEq IV over 10–20 minutes
- Effective primarily in patients with metabolic acidosis (serum HCO₃⁻ <10 mmol/L) or those with residual kidney function
- Does not enhance the potassium-lowering effect of insulin or albuterol
- Minimal benefit in anuric patients (e.g., ESKD on dialysis)
Step 3 — Remove K⁺ from the Body (Definitive)
Diuretics
- Loop diuretics (furosemide) + thiazides: effective if adequate kidney function is present
- Forced diuresis is a first-line definitive option in acute hyperkalemia with intact renal function
Dialysis
- Hemodialysis: most effective and fastest method of K⁺ removal; indicated in anuric patients (severe AKI, ESKD)
- Can seldom be initiated fast enough to replace emergency temporizing measures
Potassium Binders (oral/rectal — delayed onset; not for emergencies alone)
| Agent | Mechanism | Onset | Dose | Use |
|---|---|---|---|---|
| Sodium polystyrene sulfonate (SPS/Kayexalate) | Na⁺-K⁺ exchange resin (colon) | Hours to days | 50 g PO in sorbitol or PR retention enema | Avoid in abnormal bowel function (FDA black box: colonic necrosis risk) |
| Patiromer (Veltassa) | Ca²⁺-K⁺ exchange polymer (colon) | ~7 hours | Start 8.4 g once daily; titrate weekly | Approved for chronic hyperkalemia; monitor Mg²⁺; space 3 hr from other meds |
| Sodium zirconium cyclosilicate (Lokelma) | Binds K⁺ in exchange for H⁺/Na⁺ (entire GI tract) | ~1 hour | 10 g TID × 48 hr, then maintenance | Approved for chronic hyperkalemia; can raise gastric pH |
Non-Emergent / Chronic Management
- Dietary K⁺ counseling; avoid salt substitutes (contain KCl)
- Discontinue offending drugs (ACE inhibitors, ARBs, K⁺-sparing diuretics, NSAIDs, trimethoprim)
- Optimize loop diuretic therapy (especially with eGFR <30 mL/min)
- Oral NaHCO₃ for chronic metabolic acidosis
- K⁺ binders (patiromer or ZS-9) to facilitate continued RAAS inhibitor therapy in CKD/heart failure
Key Pitfalls
- Succinylcholine is contraindicated in hyperkalemic patients (further raises K⁺)
- Potassium-containing IV fluids (e.g., LR) should be avoided
- SPS should not be used for urgent treatment (too slow)
- Calcium potentiates digoxin toxicity — use with caution in patients on digoxin
Recent Evidence
Two recent systematic reviews (2025) are relevant:
- A network meta-analysis in Drugs (PMID 40542996) confirms that novel K⁺ binders (patiromer, ZS-9) reduce hyperkalemia and allow optimization of RAAS inhibitor therapy in CKD/heart failure.
- A systematic review in Resuscitation (PMID 39761907) evaluated pharmacological interventions for acute hyperkalemia treatment — results largely support the current standard approach (calcium, insulin/glucose, albuterol).
Sources: National Kidney Foundation Primer on Kidney Diseases 8e; Morgan and Mikhail's Clinical Anesthesiology 7e; Sabiston Textbook of Surgery 11e
This is a shared conversation. Sign in to Orris to start your own chat.