Explain histology of tonsils
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have comprehensive histology content and excellent micrographs. Here is the complete answer:
Histology of the Tonsils
Overview and Waldeyer's Ring
The tonsils are masses of lymphoid tissue strategically positioned at the entrance to the oropharynx. Together, the palatine tonsils, pharyngeal tonsil (adenoids), lingual tonsil, and smaller intervening lymphoid collections form Waldeyer's ring - a continuous collar of immune tissue guarding the common entry to both the respiratory and digestive tracts. Like other lymphatic aggregations, tonsils lack afferent lymphatic vessels but do possess efferent lymphatics.
1. Surface Epithelium
- The palatine tonsil is covered by non-keratinized stratified squamous epithelium (SSE), which is continuous with the oropharyngeal mucosa.
- A defining histological feature is the infiltration of this epithelium by lymphocytes - often so dense that the epithelial-connective tissue boundary is completely obscured on H&E sections.
- Where infiltration is less marked, the basal cells (BC) of the stratified squamous epithelium are clearly recognizable, along with a thin band of collagen fibers (CF) at the epithelial-lamina propria interface.
- In heavily infiltrated zones, lymphoid nodules literally grow into the epithelium, leaving only isolated islands of epithelial cells (Ep) within a sea of lymphocytes, and the collagen band appears fragmented.
Low-magnification H&E overview (x47) - Palatine tonsil:
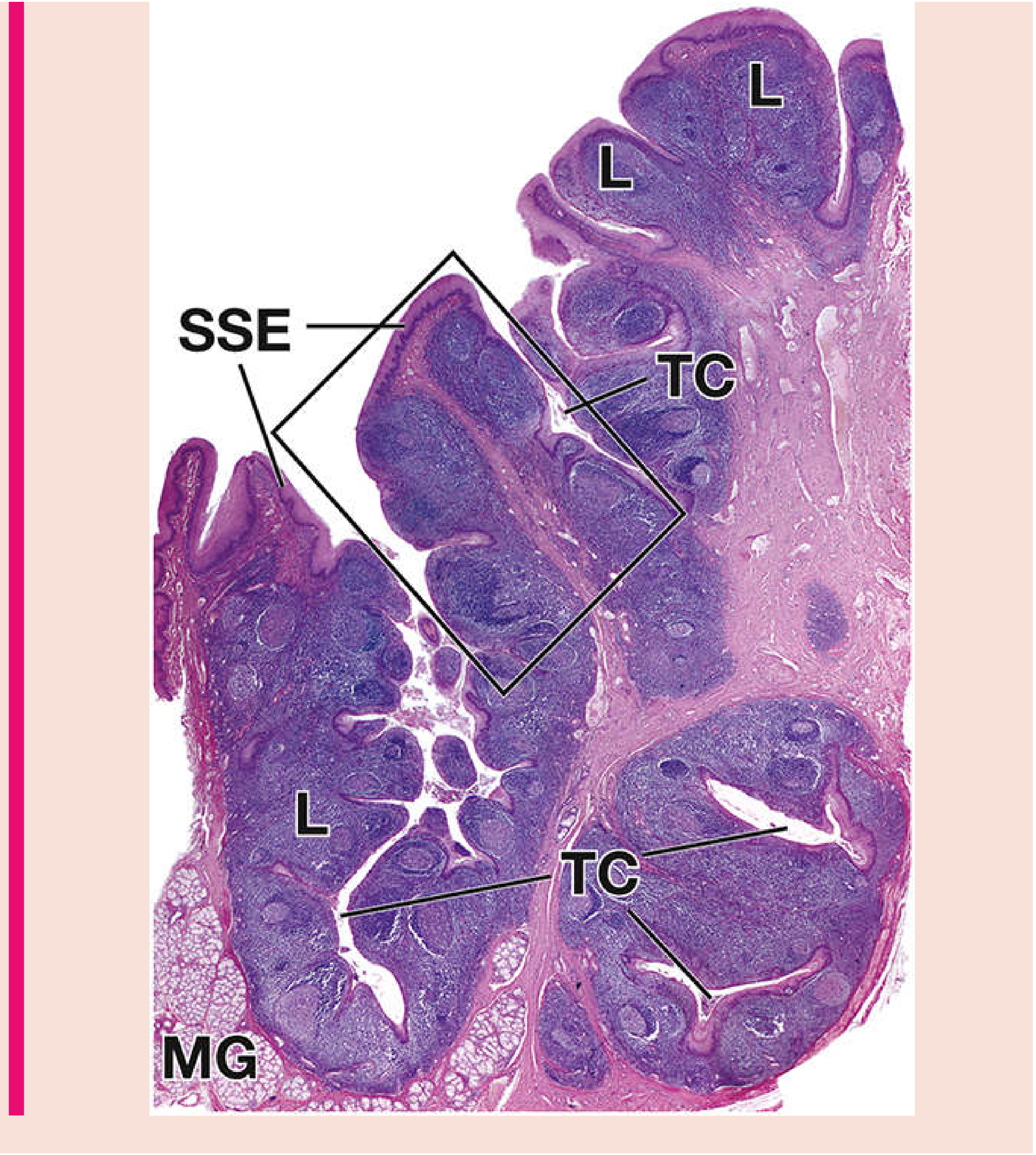
SSE = stratified squamous epithelium; TC = tonsillar crypts; L = lymphatic tissue; MG = mucus-secreting glands. (Histology: A Text and Atlas, Plate 14.1)
2. Tonsillar Crypts
- The surface epithelium dips deep into the underlying connective tissue, forming 10-15 blind-ending, often highly branched crypts that penetrate the full thickness of the tonsil.
- The crypt walls are lined by the same stratified squamous epithelium and are closely associated with underlying lymphoid nodules.
- Crypts serve as antigen-sampling sites - their epithelium is in intimate contact with mucosal lymphocytes, facilitating immune surveillance.
- The base of crypts may contain mucus-secreting glands (MG), visible at low magnification.
- Clinically, crypts can trap debris and bacteria, predisposing to recurrent tonsillitis.
3. Lymphoid Nodules and Germinal Centers
This is the dominant structural feature of the tonsil parenchyma:
- The bulk of the tonsil consists of numerous lymphatic nodules packed within the lamina propria/mucosa.
- Because of their density, adjacent nodules tend to merge with one another.
- Many nodules contain well-developed germinal centers (GC) - lighter-staining central zones visible on H&E. These are sites of B-cell proliferation, somatic hypermutation, and affinity maturation following antigen stimulation.
- The germinal center is surrounded by a darker mantle zone of naive B lymphocytes.
- The overall architecture differs from a lymph node - there is no distinct cortex-medulla organization and no capsule separating lobules.
Medium and high magnification H&E (x47 and x365):
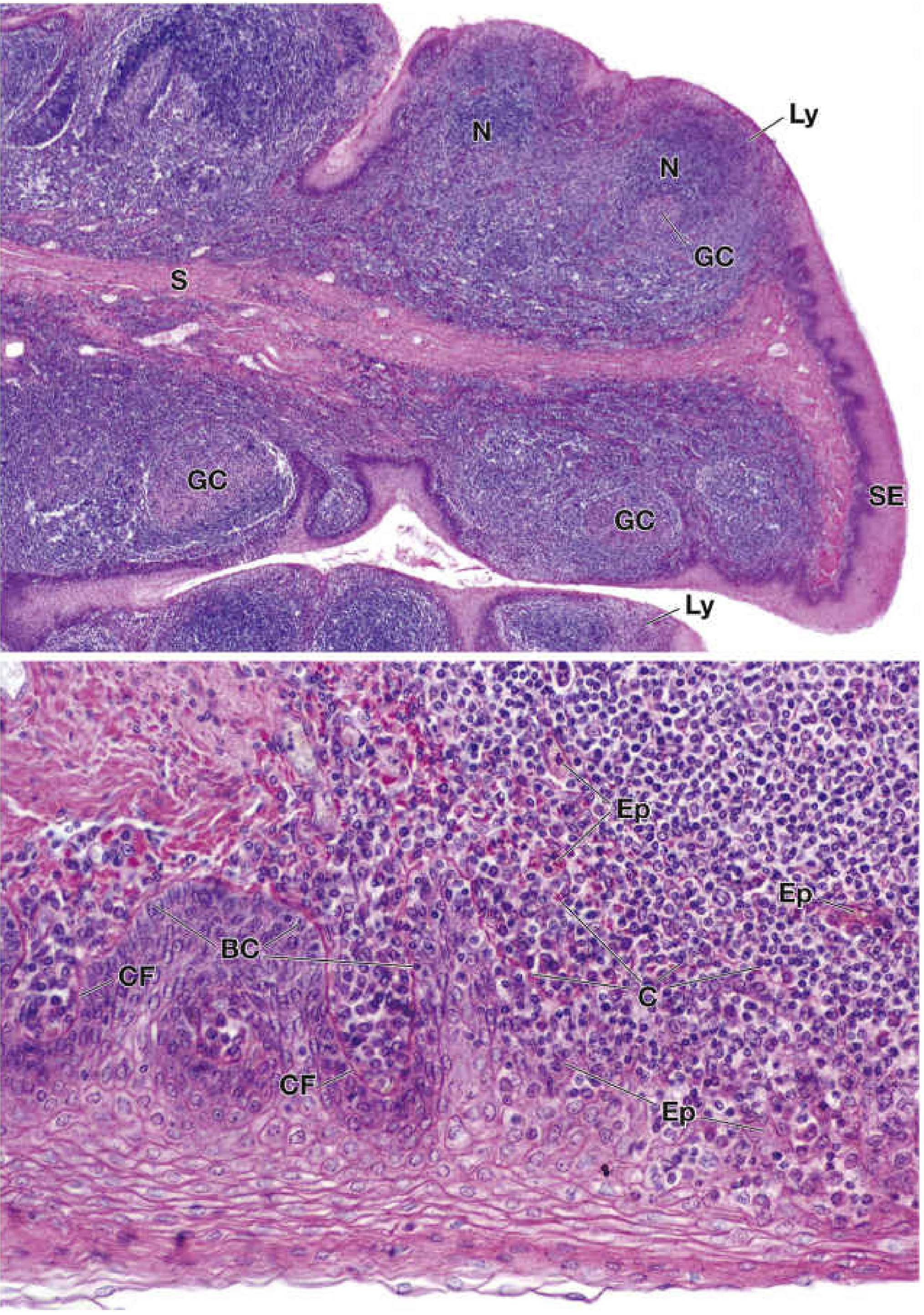
Top panel (x47): N = nodules; GC = germinal centers; SE = surface epithelium; Ly = lymphocytes invading epithelium; S = submucosa. Bottom panel (x365): BC = basal cells; CF = collagen fibers at epithelial boundary; Ep = islands of epithelial cells within lymphoid tissue; C = disrupted collagen. (Histology: A Text and Atlas, Plate 14.1)
4. Submucosa and Capsule
- Beneath the lymphoid nodules lies the submucosa (S), consisting of dense irregular connective tissue that is continuous with the connective tissue of the tonsillar bed.
- The deep (lateral) surface of the palatine tonsil is bounded by a fibrous hemicapsule, which separates the tonsil from the superior constrictor muscle and allows the surgical plane of cleavage during tonsillectomy.
- Unlike lymph nodes, the tonsil does not have a complete fibrous capsule on its mucosal side.
- Trabeculae extend inward from this hemicapsule, incompletely dividing the lymphoid tissue.
5. Associated Glands
- Minor mucous salivary glands are present in the connective tissue beneath and around the crypts.
- These are seromucinous glands whose secretions drain into the crypts, contributing to local mucosal defense.
6. Vascular Supply (Histologically Relevant)
- Blood vessels enter via the hemicapsule.
- The external palatine (paratonsillar) vein descends lateral to the hemicapsule - surgically important as a source of post-tonsillectomy hemorrhage.
7. Comparison: Three Tonsil Types
| Feature | Palatine Tonsil | Pharyngeal Tonsil (Adenoid) | Lingual Tonsil |
|---|---|---|---|
| Epithelium | Non-keratinized stratified squamous | Pseudostratified ciliated columnar (respiratory) | Stratified squamous |
| Crypts | Deep, branching | Shallow folds/furrows (not true crypts) | Shallow crypts |
| Capsule | Hemicapsule (lateral only) | Thin capsule | No distinct capsule |
| Location | Tonsillar fossa | Roof of nasopharynx | Base of tongue |
Key Histological Landmarks Summary
| Structure | What You See on H&E |
|---|---|
| Surface epithelium | Stratified squamous; often obscured by lymphocytes |
| Tonsillar crypts | Epithelium-lined invaginations penetrating full thickness |
| Lymphatic nodules | Dense dark-staining masses, closely packed |
| Germinal centers | Pale eosinophilic central zones within nodules |
| Submucosa | Dense connective tissue deep to nodules |
| Hemicapsule | Fibrous layer on the lateral/deep surface only |
| Mucous glands | At crypt bases and in submucosa |
Sources: Histology: A Text and Atlas with Correlated Cell and Molecular Biology (Plate 14.1); Scott-Brown's Otorhinolaryngology Head & Neck Surgery
This is a shared conversation. Sign in to Orris to start your own chat.