Tumor like condition of the liver
Reading File
Finding Sources
Finding Sources
Searching PubMed
"liver" AND "tumor-like conditions" OR "hepatic pseudotumor"
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive information from multiple authoritative textbooks (Robbins Pathology, Schwartz's Surgery, Bailey & Love's, Sleisenger & Fordtran's, and Yamada's Gastroenterology). Let me compose the complete response.
Tumor-Like Conditions of the Liver
"Tumor-like conditions" of the liver refers to a group of non-neoplastic or benign proliferative hepatic lesions that clinically and/or radiologically mimic true liver tumors. They are important because failing to distinguish them from malignancies can lead to unnecessary surgery or, conversely, missing a serious diagnosis.
Classification Overview
| Category | Lesions |
|---|---|
| Vascular | Cavernous Hemangioma, Peliosis Hepatis |
| Hyperplastic/Hamartomatous | Focal Nodular Hyperplasia (FNH), Bile Duct Hamartoma, Mesenchymal Hamartoma |
| Cystic | Simple (Congenital) Hepatic Cyst, Polycystic Liver Disease, Caroli's Disease |
| Benign Neoplasm (often misclassified) | Hepatocellular Adenoma |
| Infectious/Inflammatory | Hepatic Abscess, Hydatid Cyst (Echinococcosis) |
1. Cavernous Hemangioma
The most common benign liver lesion, occurring in 2-20% of the population with a female predominance.
Pathology:
- Composed of multiple large vascular channels of varying sizes, lined by a single layer of flat endothelium, supported by fibrous septa
- Usually solitary; multiple in ~10% of cases
- Reddish-purple or bluish masses, well-circumscribed but rarely encapsulated
- Larger lesions (>5 cm) are called "giant cavernous hemangiomas" and can reach 27 cm
Clinical features:
- The vast majority are small and asymptomatic, found incidentally on imaging
- Giant hemangiomas may cause upper abdominal pain (from partial infarction or pressure on adjacent structures), nausea, early satiety
- Kasabach-Merritt syndrome: thrombocytopenia due to platelet sequestration - seen in infants, rare in adults
- Malignant transformation has NOT been reported
Imaging:
- Ultrasound: echogenic, uniform mass in posterior right lobe, typically <3 cm
- CT (contrast): peripheral nodular enhancement progressing centripetally ("fill-in pattern") - pathognomonic
- MRI: hypointense on T1, strikingly hyperintense on T2; gadolinium shows peripheral nodular enhancement
Caution: Percutaneous biopsy should NOT be performed if hemangioma is suspected due to risk of severe hemorrhage.
Management: Incidental finding - reassure and observe. Surgical resection (enucleation or formal resection) only if significantly symptomatic.
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease, p. 1864-1865
- Bailey and Love's Short Practice of Surgery, p. 1234
2. Focal Nodular Hyperplasia (FNH)
The second most common benign liver tumor after hemangioma, with a prevalence of ~0.9%, predominantly in young to middle-aged women (male:female = 1:8).
Pathogenesis: Believed to be a hyperplastic response to an anomalous, pre-existing arterial malformation - not a true neoplasm.
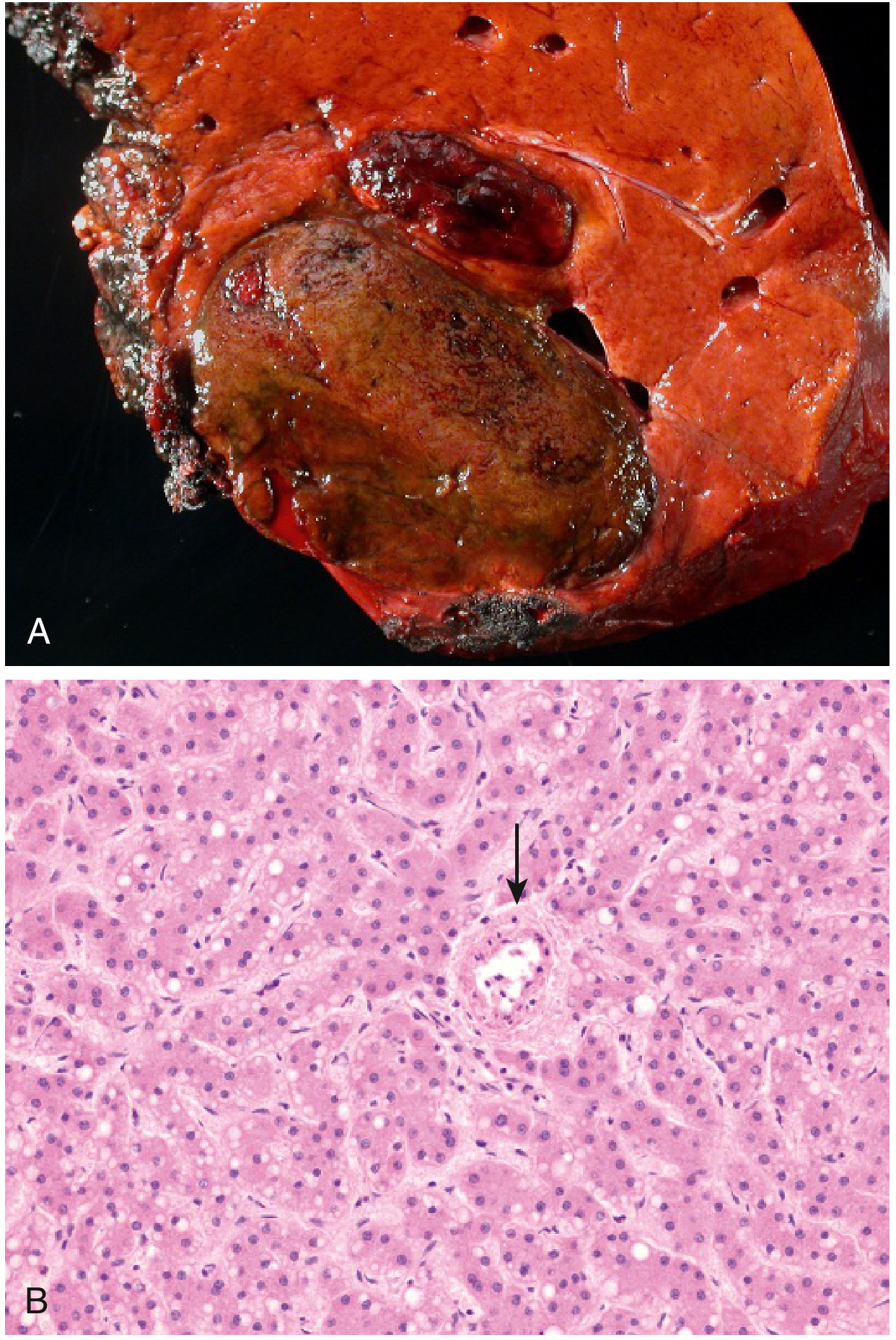
Gross Pathology:
- Well-demarcated, poorly encapsulated nodule, often several centimeters in diameter
- Characteristic central stellate (star-shaped) scar with fibrous septa radiating to the periphery (see image below)

Microscopy:
- Contains both hepatocytes AND Kupffer cells
- Central scar contains large abnormal vessels and ductular reactions along the spokes
- Lacks normal portal areas and terminal hepatic veins
- No capsule
Imaging:
- Hypervascular on arterial phase CT, isodense to liver on venous phase, with visible central scar
- MRI (liver-specific agents like gadoxetate): FNH takes up contrast in the hepatobiliary phase, distinguishing it from adenoma and metastases
Key clinical points:
- No malignant potential
- Does NOT typically rupture spontaneously
- No association with underlying liver disease
- Mild association with oral contraceptives (weaker than adenoma)
Management: Once confirmed, no treatment or follow-up required. Resect only if symptomatic or if adenoma/HCC cannot be excluded. Stop OCP use.
- Robbins & Kumar Basic Pathology, p. 625
- Schwartz's Principles of Surgery, p. 1402
3. Hepatocellular Adenoma
A benign neoplasm, but clinically significant due to risk of rupture and malignant transformation.
Who gets it:
- Predominantly reproductive-age women (typically >30 years)
- Historically linked to oral contraceptive (OCP) use; with lower-dose estrogen formulations, the major risk factor has shifted to obesity and metabolic syndrome
- Driver mutations described include gain-of-function mutations in β-catenin (associated with malignant transformation risk)
Gross pathology:
- Soft, encapsulated, tan to light brown
- Usually solitary (multiple = hepatic adenomatosis)
Microscopy:
- Sheets of normal-appearing to atypical hepatocytes
- No portal tracts, no bile ducts, no Kupffer cells
- Prominent thick-walled arteries at the periphery
- No true lobular architecture
Complications:
- Rupture with intraperitoneal hemorrhage: occurs in 10-25% of cases, can be life-threatening
- Malignant transformation to HCC: up to 10% risk, especially with β-catenin mutations and in men
- Risk of both complications increases with lesion size (>4-5 cm)
- Documented high maternal and fetal mortality if rupture occurs during pregnancy
Imaging:
- CT: sharply defined borders, hypervascular on arterial phase, hypo- or isodense on venous phase
- MRI: hyperintense on T1 (fat/glycogen content), early enhancement with gadolinium
- Liver-specific MRI agents (gadoxetate/Eovist): adenoma does NOT enhance in hepatobiliary phase (distinguishes from FNH)
Management:
-
Discontinue OCP/estrogen
-
Surgical resection recommended for lesions >4-5 cm due to rupture and malignancy risk
-
Smaller lesions may regress after stopping OCP
-
Robbins & Kumar Basic Pathology, p. 626
-
Schwartz's Principles of Surgery, p. 1403
4. Hepatic Cysts
Simple (Congenital) Cysts:
- Most common liver lesion overall; prevalence 5-14% of population, higher in women
- Thin-walled, contain serous fluid; no communication with biliary tree
- Usually asymptomatic; incidental finding on imaging
- No malignant potential; resection only if symptomatic
Polycystic Liver Disease (PCLD):
- Autosomal dominant; associated with polycystic kidney disease
- Can cause severe symptoms from mass effect
- Severe cases: hepatic resection or liver transplantation
Caroli's Disease:
- Congenital ductal plate malformation causing segmental cystic dilatation of intrahepatic biliary radicals
- Associated with biliary lithiasis, cholangitis, biliary abscess
- ~7% develop cholangiocarcinoma
- Diagnosed by MRCP/ERCP; treatment is biliary drainage
Hydatid Cyst (Echinococcus granulosus):
-
Parasitic infection; can form large cystic masses mimicking tumors
-
"Daughter cysts" on imaging are characteristic
-
Schwartz's Principles of Surgery, p. 1402-1403
5. Bile Duct Hamartoma (Von Meyenburg Complexes)
- Small lesions (2-4 mm), typically visualized on liver surface at laparotomy
- Firm, smooth, whitish-yellow in appearance
- Can be extremely difficult to differentiate from small metastatic deposits - excisional biopsy often required
Key Differentiating Features at a Glance
| Feature | Hemangioma | FNH | Adenoma |
|---|---|---|---|
| Sex predilection | F > M | Women (young-middle) | Women of reproductive age |
| OCP association | None | Weak | Strong (historically) |
| Kupffer cells | No | Yes | No |
| Portal tracts | No | No (but ductular reaction) | No |
| Central scar | No | Yes (stellate) | No |
| Capsule | No | No | Yes (pseudo-capsule) |
| Malignant potential | None | None | Up to 10% |
| Rupture risk | Rare | Very rare | 10-25% |
| Management | Observe | Observe | Resect if >4-5 cm |
| CT (arterial) | Peripheral nodular enhancement | Intense homogeneous | Hypervascular |
| MRI T2 | Very bright | Iso/hyperintense | Hyperintense (T1 also) |
Recent Literature Note
A 2025 review (PMID 38874132) in Diagnostic and Interventional Radiology specifically addresses tumor-like conditions that mimic liver tumors, highlighting the role of modern MRI in differentiating these entities from true malignancies - consistent with the textbook guidance above.
This is a shared conversation. Sign in to Orris to start your own chat.