Patient with atrial fibrillation posted for non cardiac surgery
Reading File
Finding Sources
Finding Sources
Searching PubMed
"atrial fibrillation" AND "noncardiac surgery" AND perioperative management
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Here is a comprehensive, textbook-based clinical guide for managing a patient with atrial fibrillation (AF) posted for non-cardiac surgery.
Atrial Fibrillation - Non-Cardiac Surgery: Perioperative Management
AF is the most frequently encountered perioperative cardiac arrhythmia. Its presence signals elevated baseline risk and demands systematic evaluation across four domains: preoperative assessment, rate/rhythm control, anticoagulation management, and intraoperative/postoperative care.
1. Preoperative Assessment
AF as a risk marker: Preexisting AF is an independent marker of elevated perioperative risk. In large prospective cohort data, preexisting AF was associated with increased postoperative cardiovascular events including stroke, cardiovascular death, myocardial injury, heart failure, and cardiac arrest.
Key preoperative evaluation points:
- Identify and manage underlying conditions: ischemic heart disease, valvular disease, heart failure, hypertension, thyroid disease
- Assess current rate/rhythm control strategy and adequacy
- Determine anticoagulation status and type (VKA vs. DOAC)
- Establish the CHA₂DS₂-VASc score to quantify thromboembolic risk
- Assess functional status and surgical urgency
Rapid ventricular rate (>100 bpm): Must be controlled before any elective surgery. Rate control to <100 bpm is the threshold for safe surgery.
Slow ventricular rate without rate-controlling drugs: Suggests sick sinus syndrome - inquire about syncope or presyncope.
2. Rate and Rhythm Control
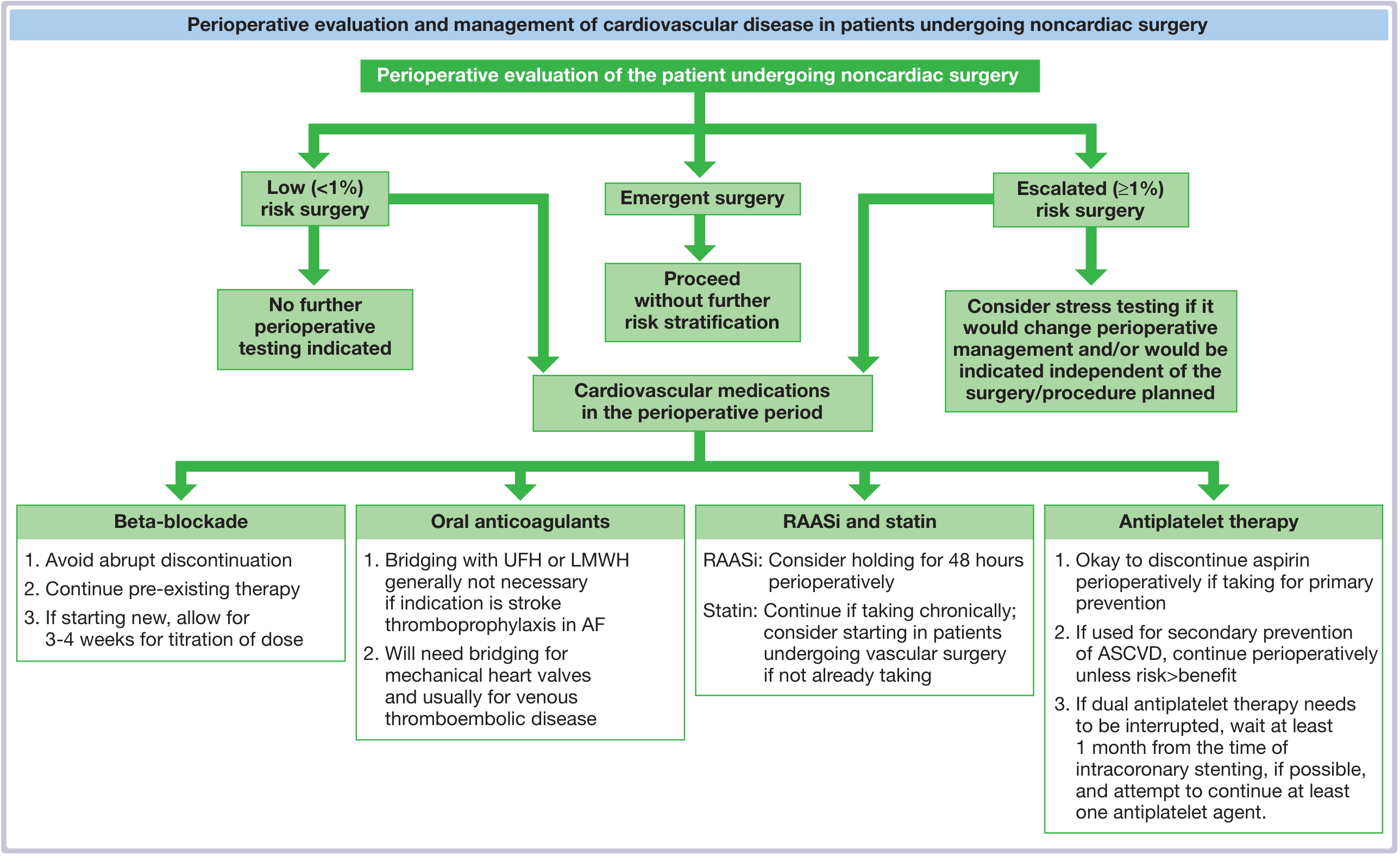
- Continue all existing rate-controlling medications: beta-blockers, digoxin, calcium channel blockers (diltiazem/verapamil), and antiarrhythmic drugs perioperatively - abrupt discontinuation risks rebound tachycardia
- Rhythm control is generally not required before noncardiac surgery if rate is adequately controlled
- Stable chronic AF with adequate rate control does not require any additional rhythm intervention before elective surgery
3. Anticoagulation Management - The Core Decision
This is the most complex and consequential perioperative decision. The calculus involves balancing bleeding risk of surgery vs. thromboembolic risk from interrupting anticoagulation.
Step 1: Determine if interruption is needed
| Situation | Decision |
|---|---|
| Minimal bleeding risk procedures (cataract surgery, minor dental, pacemaker/ICD implant) | Continue anticoagulation uninterrupted |
| Significant bleeding risk | Temporarily discontinue |
| Neuraxial anesthesia planned | Must discontinue DOACs regardless |
Step 2: Timing of discontinuation
Warfarin (VKA):
- Stop 5 days before elective surgery
- Longer period if INR >3.0
- Recheck INR within 24 hours before surgery
- If INR ≥ 1.5 on the day of surgery, consider low-dose oral vitamin K (1-2 mg) or FFP depending on urgency
Direct Oral Anticoagulants (DOACs - PAUSE regimen):
| Drug | Low Bleeding Risk Procedure | High Bleeding Risk Procedure |
|---|---|---|
| Dabigatran (eGFR ≥50) | Hold 1 day before | Hold 2 days before |
| Dabigatran (eGFR <50) | Hold 2 days before | Hold 4 days before |
| Rivaroxaban / Apixaban / Edoxaban | Hold 1 day before | Hold 2 days before |
- Longer interruption needed for: eGFR <30 mL/min, hepatic impairment, drugs inhibiting CYP3A4 or P-glycoprotein pathways
- Routine DOAC drug levels are not required, but may be checked in high-risk cases
Step 3: Bridging anticoagulation decision
Key evidence - the BRIDGE Trial (2015, NEJM):
- RCT of 1,884 AF patients with warfarin interrupted for elective procedures
- Placebo (no bridging) was noninferior to LMWH bridging for arterial thromboembolism prevention
- Bridging group had significantly higher major bleeding rates
- Conclusion: For most AF patients, bridging is unnecessary and harmful
When bridging IS indicated:
- Mechanical prosthetic heart valves (especially mitral position)
- Very high thromboembolic risk: CHA₂DS₂-VASc ≥7-8
- Recent ischemic stroke or TIA (within 3-6 months)
- Acute arterial embolism
- VTE at high risk for recurrence
When NOT to bridge (standard nonvalvular AF):
- CHA₂DS₂-VASc score ≤6 with no recent stroke/TIA
- Supported by BRIDGE trial data and endorsed by ACC/AHA and ACCP guidelines
Bridging protocol (when indicated):
- Initiate IV UFH or subcutaneous LMWH when INR becomes subtherapeutic
- Stop UFH 4-6 hours before surgery
- Stop LMWH 24 hours before surgery
- Resume LMWH 24 hours after minor/low-bleeding-risk surgery
- Resume LMWH 48-72 hours after major/high-bleeding-risk surgery
Resume warfarin within 24 hours postoperatively (takes 4-5 days to reach therapeutic levels).
Step 4: Very high-risk patients - delay elective surgery
Patients with:
- Recent ischemic stroke
- AF with CHA₂DS₂-VASc >1 (males) or >2 (females) on inadequate anticoagulation
...should not undergo elective operations until thromboembolic risk is optimized.
4. Intraoperative Considerations
- Hemodynamic goals: Maintain adequate ventricular rate (60-100 bpm); avoid tachycardia (worsens diastolic filling), hypotension, and hypovolemia
- Monitor: Continuous ECG, pulse oximetry; watch for rate-related ischemia if rapid AF develops
- New-onset rapid AF intraoperatively: Address precipitating factors first (hypoxia, hypercarbia, pain, electrolyte disturbances, light anesthesia, bleeding)
- Cardioversion may be required if hemodynamically unstable with new-onset AF
- Regional vs. general anesthesia: Regional techniques are generally safe but DOAC discontinuation timelines above must be respected before neuraxial blocks
5. Postoperative Management
- Postoperative AF following noncardiothoracic surgery warrants anticoagulation until spontaneous conversion or formal anticoagulation decision is made
- Restart anticoagulation as soon as surgical hemostasis allows - typically within 24-48 hours
- DOACs can be restarted immediately once bleeding risk is acceptable (rapid onset means no bridging needed on restart)
- Continue rate-controlling medications postoperatively
- Monitor closely for stroke symptoms in the perioperative window
Summary Table
| Issue | Key Action |
|---|---|
| Rate >100 bpm preop | Control before elective surgery |
| Existing rate meds | Continue all perioperatively |
| Warfarin interruption | Stop 5 days before surgery |
| DOAC interruption | 1-2 days (low risk) / 2 days (high risk) |
| Bridging for nonvalvular AF | Generally NOT indicated (BRIDGE trial) |
| Bridging for mechanical valves / CHA₂DS₂-VASc ≥7-8 | Consider bridging |
| Minimal bleeding risk surgery | May continue anticoagulation uninterrupted |
| INR ≥1.5 before surgery | Low-dose oral vitamin K or FFP |
| Resume warfarin postop | Within 24 hours |
| Resume DOAC postop | When hemostasis secured (24-48 hrs) |
Sources:
- Fuster and Hurst's The Heart, 15th Edition - Chapter 72 (Perioperative Cardiovascular Evaluation)
- Miller's Anesthesia, 10e - Chapter 28 (Preexisting AF, anticoagulation tables)
- Barash, Cullen, and Stoelting's Clinical Anesthesia, 9e - Anticoagulation section
- Sabiston Textbook of Surgery - Perioperative Anticoagulation
- Washington Manual of Medical Therapeutics - Anticoagulant Bridging
- BRIDGE Trial: Douketis et al., NEJM 2015;373:823-833
This is a shared conversation. Sign in to Orris to start your own chat.