Carcinoma cervix detailed description in post graduate level from barek and novak and new updates
Reading File
Finding Sources
Finding Sources
Searching PubMed
"cervical cancer" AND management
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Searching PubMed
"cervical cancer" AND ("immunotherapy" OR "pembrolizumab")
Loading Image
Loading Image
I now have comprehensive material from Berek & Novak's Gynecology plus current trial data. Let me compose the full postgraduate-level response.
Carcinoma of the Cervix - Postgraduate Level
Source: Berek & Novak's Gynecology (16th ed.) + Current Evidence (2024-2025)
1. EPIDEMIOLOGY AND RISK FACTORS
Invasive carcinoma of the cervix is considered a preventable disease because it has a long preinvasive state, screening programs exist, and treatment of preinvasive lesions is effective. The CDC reported approximately 12,578 new cases with 4,115 deaths annually in the United States. The worldwide incidence is declining and cervical cancer is being diagnosed at earlier stages, improving survival. The mean age at diagnosis is 47 years, with a bimodal distribution peaking at 35-39 years and 60-64 years. The lifetime probability of developing cervical cancer is approximately 1:128.
Approximately 30% of cervical cancer cases in developed nations occur in women who have never had a Papanicolaou (Pap) test; in developing countries, this approaches 60%.
Risk Factors:
-
Young age at first intercourse (< 16 years)
-
Multiple sexual partners
-
Cigarette smoking
-
Race/ethnicity
-
High parity
-
Low socioeconomic status
-
Chronic immune suppression (including HIV/AIDS - cervical cancer is an AIDS-defining illness)
-
HPV infection (the fundamental causal agent)
-
Berek & Novak's Gynecology, p. 2217
2. PATHOGENESIS - HPV AND MOLECULAR MECHANISMS
The initiating event in cervical dysplasia and carcinogenesis is infection with human papillomavirus (HPV). HPV was detected in up to 99% of women with squamous cervical carcinoma. HPV is the causative agent in both squamous cell carcinoma and adenocarcinoma, though the respective tumors may use different carcinogenic pathways.
There are more than 100 HPV types; >30 can infect the lower genital tract. 15 subtypes are designated high-risk, with HPV 16 and 18 accounting for up to 70% of all cervical carcinomas.
Molecular mechanism:
- HPV E6 protein binds and degrades p53 tumor suppressor → prevents cell cycle arrest and apoptosis when damaged DNA is present
- HPV E7 protein binds and inactivates Rb (retinoblastoma protein) → disrupts transcription factor E2F → unregulated cellular proliferation
- Both steps are required for malignant transformation of cervical epithelial cells
- Cofactors include herpes simplex virus and Chlamydia trachomatis
HPV Vaccines:
| Vaccine | Subtypes Covered | Efficacy |
|---|---|---|
| Cervarix (bivalent) | 16, 18 | 97-100% for CIN2/3 in naive women |
| Gardasil (quadrivalent) | 6, 11, 16, 18 | 97-100% in naive; 44% in previously infected |
| Gardasil-9 (9-valent) | 6, 11, 16, 18, 31, 33, 45, 52, 58 | Non-inferior to quadrivalent for shared types |
- Berek & Novak's Gynecology, p. 2217-2218
3. PATHOLOGY
3.1 Histologic Types
Squamous Cell Carcinoma (65-80%)
The most common type. Originates at the squamocolumnar junction (transformation zone). Subtypes include large-cell keratinizing, large-cell non-keratinizing, and small-cell types.
Adenocarcinoma (20-25%)
Incidence is increasing, particularly in younger women. Originates from endocervical glandular epithelium. A subtype - adenosquamous carcinoma - has mixed features and may carry a worse prognosis. Adenocarcinoma does not have a specific colposcopic appearance and may develop within the endocervix, making traditional screening less reliable.
Other rare types: Small cell neuroendocrine, clear cell, papillary serous, glassy cell.
3.2 Histologic Appearance of Early Invasion
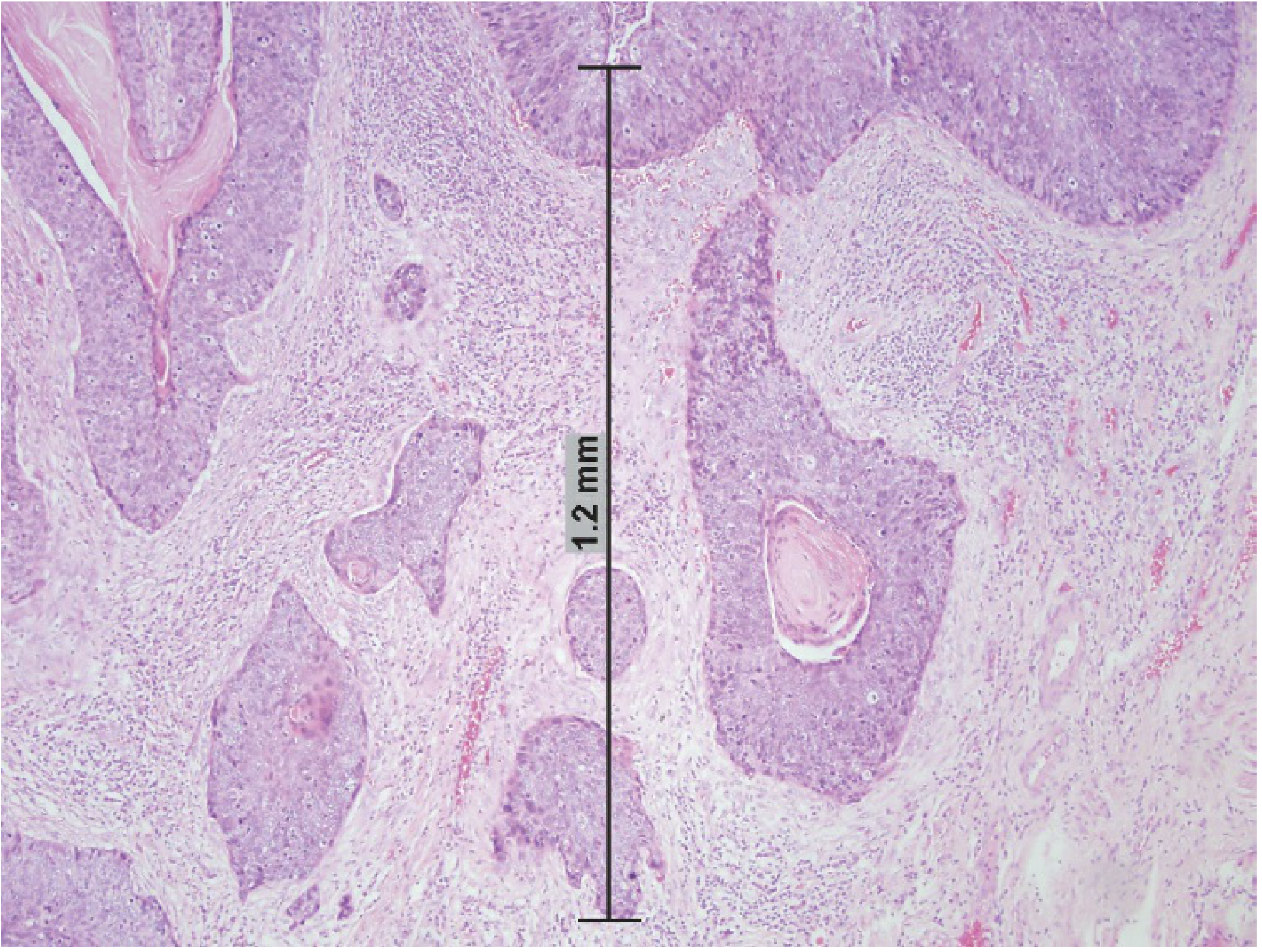
Histology: FIGO Stage IA1 squamous carcinoma with 1.2 mm measured depth of invasion, keratin pearl formation, desmoplastic stromal reaction, and surrounding chronic inflammatory infiltrate (Berek & Novak's, Fig. 38-2)
Early invasion appears as a protrusion of malignant cells from the stromal-epithelial junction - cells appear better differentiated than adjacent noninvasive cells, with:
- Abundant pink cytoplasm
- Hyperchromatic nuclei
- Small-to-medium nucleoli
- Tongue-like processes into the stroma
- Desmoplasia (fibroblast proliferation) in stroma
- Band-like infiltrate of chronic inflammatory cells
Important: Uneven tissue shrinkage by fixative creates artifactual spaces between tumor nests and stroma simulating lymphovascular invasion. True LVSI requires endothelial lining. Lesions with < 3 mm invasion rarely have LVSI; those between 3-5 mm have positive pelvic nodes in 3-8% of cases.
- Berek & Novak's Gynecology, p. 2222
4. CLINICAL FEATURES
4.1 Symptoms
- Abnormal vaginal bleeding - the most common presenting symptom; post-coital, intermenstrual, or postmenopausal bleeding
- Watery, blood-tinged vaginal discharge (may be malodorous with necrosis)
- Pelvic or back pain - indicates advanced disease with parametrial or pelvic sidewall involvement
- Leg edema - lymphatic or venous obstruction from pelvic disease
- Urinary symptoms - hematuria, frequency, or obstruction (advanced disease)
- Rectal symptoms - tenesmus, hematochezia (advanced disease)
- Early-stage disease may be completely asymptomatic, found only on routine screening
4.2 Colposcopic Appearance
- Atypical vessels: punctation, mosaic pattern, coarse irregular vessels are characteristic
- Irregular surface contour: ulceration (loss of desmosomes), papillary growth pattern
- Color change: yellow-orange rather than the normal pink squamous or red endocervical epithelium; due to increased vascularity, surface necrosis, or keratin production
- All papillary cervical growths must be biopsied to exclude invasive disease
5. STAGING - FIGO 2018 (REVISED)
A major change in the 2018 revision is that imaging and pathologic findings may now be used to assign stage (particularly for Stage IIIC). The notation "r" (imaging) or "p" (pathologic) is added to IIIC designations.
FIGO 2018 Staging Table
| Stage | Definition |
|---|---|
| IA | Invasive carcinoma diagnosed only by microscopy; deepest invasion ≤5 mm |
| IA1 | Stromal invasion ≤3.0 mm depth, extension ≤7.0 mm |
| IA2 | Stromal invasion >3.0 mm and ≤5.0 mm, extension ≤7.0 mm |
| IB | Clinically visible lesions or preclinical > IA |
| IB1 | Stromal invasion ≥5 mm and < 2 cm |
| IB2 | ≥2 cm and < 4 cm |
| IB3 | ≥4 cm |
| IIA | Beyond uterus, no parametrial invasion |
| IIA1 | < 4 cm |
| IIA2 | ≥ 4 cm |
| IIB | With parametrial invasion |
| IIIA | Involves lower third of vagina, no pelvic wall extension |
| IIIB | Extends to pelvic wall and/or hydronephrosis/non-functioning kidney |
| IIIC1 | Pelvic lymph node metastasis (IIIC1r or IIIC1p) |
| IIIC2 | Para-aortic lymph node metastasis (IIIC2r or IIIC2p) |
| IVA | Spread to adjacent organs (bladder/rectal mucosa) |
| IVB | Distant metastases |
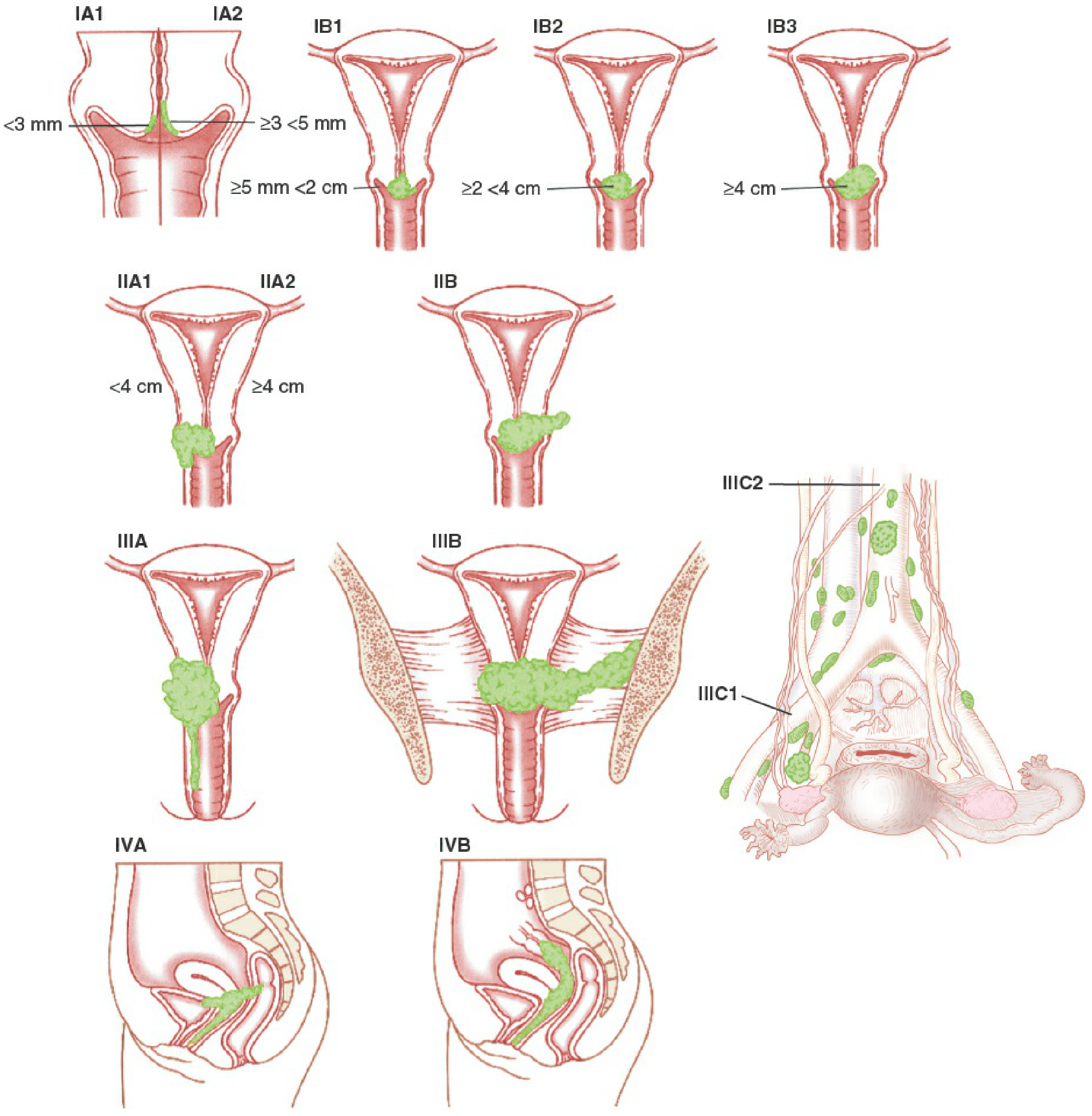
FIGO 2018 Cervical Cancer Staging (Berek & Novak's, Fig. 38-3)
Key additions in 2018:
-
New IB substages (IB1, IB2, IB3)
-
Stage IIIC introduced for lymph node metastasis regardless of primary tumor size
-
Allowance of imaging and pathology to upstage
-
Hydronephrosis alone (even without pelvic wall involvement) still constitutes Stage IIIB unless due to another cause
-
Berek & Novak's Gynecology, p. 2225-2229 (Bhatla N, Berek JS et al. FIGO 2019)
6. IMAGING AND STAGING WORKUP
| Modality | Sensitivity | Specificity | Notes |
|---|---|---|---|
| Lymphangiography | 79% | 73% | False positive 20-40%, largely abandoned |
| CT | 34% | 97% | Accuracy 80-85%; poor for early LN disease |
| MRI | Superior to CT | Equivalent to CT | Best for parametrial involvement on T2W images |
| Ultrasound | 19% | 99% | High false-negative rate |
| PET scan | 75% | 98% | Best for extrapelvic/para-aortic disease |
| PET/CT | Superior to PET alone | Particularly for pelvic adenopathy |
A meta-analysis of 72 studies found PET superior to both CT and MRI for lymph node metastasis detection (PET 75%/98% vs. CT 58%/92% vs. MRI 56%/93%).
MRI on T2-weighted images provides the best assessment of parametrial involvement. FIGO 2018 now allows these imaging findings to guide staging.
- Berek & Novak's Gynecology, p. 2225-2226
7. PROGNOSTIC FACTORS
7.1 Intermediate-Risk Factors (after radical hysterectomy)
- Large tumor size
- Deep cervical stromal invasion (middle or deep one-third)
- Lymphovascular space invasion (LVSI)
7.2 High-Risk Factors
- Positive or close surgical margins
- Positive lymph nodes
- Microscopic parametrial involvement
Patients with intermediate-risk factors have a 30% recurrence risk within 3 years; with high-risk factors, this rises to 40%.
7.3 Survival by Factor
| Factor | 5-Year Survival |
|---|---|
| Lesion < 2 cm | ~90% |
| Lesion > 2 cm | ~60% |
| Lesion > 4 cm | ~40% |
| Depth of invasion < 1 cm | ~90% |
| Depth of invasion > 1 cm | 63-78% |
| Parametrium negative | ~95% |
| Parametrium positive | ~69% |
| Parametrium + positive nodes | 39-42% |
| Negative lymph nodes | 85-90% |
| Positive lymph nodes | 20-74% (varies by location) |
| Common iliac nodes positive | ~25% |
| Only pelvic nodes positive | ~65% |
Lymph node status is the single most independent predictor of survival.
- Berek & Novak's Gynecology, p. 2251-2252
8. MANAGEMENT BY STAGE
Management Table (Berek & Novak Table 38-4)
| Stage | Disease | Primary Treatment |
|---|---|---|
| IA1 (no LVSI) | < 3 mm | Conization or extrafascial hysterectomy |
| IA1 (+ LVSI) | < 3 mm + LVSI | Modified radical trachelectomy or hysterectomy + pelvic LND or SLN |
| IA2 | ≥3 to < 5 mm | Modified radical trachelectomy or hysterectomy + pelvic LND or SLN |
| IB1 | ≥5 mm to < 2 cm | Radical/modified radical trachelectomy or hysterectomy + pelvic LND or SLN |
| IB2 | 2-4 cm | Radical hysterectomy + pelvic LND |
| IB3 | ≥4 cm | Chemoradiation (pelvic field) |
| IIA1 | < 4 cm + upper vagina | Radical hysterectomy + pelvic LND or chemoradiation |
| IIA2 | ≥4 cm + upper vagina | Chemoradiation (pelvic field) |
| IIB | Parametria involved | Chemoradiation (pelvic field) |
| IIIA | Lower vagina | Chemoradiation (pelvic field) |
| IIIB | Pelvic wall/hydronephrosis | Chemoradiation (pelvic ± extended field) |
| IIIC1 | Pelvic LN+ | Chemoradiation (pelvic ± extended field) |
| IIIC2 | Para-aortic LN+ | Chemoradiation (extended field + systemic chemotherapy) |
| IVA | Adjacent pelvic organs | Chemoradiation ± pelvic exenteration |
| IVB | Distant organs | Systemic chemotherapy ± radiation |
8.1 Stage IA1 (< 3 mm, no LVSI)
- Less than 1% incidence of pelvic lymph node metastasis
- Therapeutic conization is adequate if fertility preservation desired; margins and post-conization ECC must be negative
- Extrafascial hysterectomy without lymphadenectomy for women who don't desire fertility
- If LVSI is present: modified radical hysterectomy + pelvic lymphadenectomy
8.2 Stage IA2 (3-5 mm invasion)
- Pelvic node metastasis rate: 3-8% → lymphadenectomy or SLN mapping required
- Modified radical hysterectomy (Type II) with pelvic LND
- Radical trachelectomy if fertility preservation desired
8.3 Stages IB1-IIA1 (small operable)
- Type III Radical (Wertheim) Hysterectomy + bilateral pelvic lymphadenectomy is standard
- Radical trachelectomy for fertility preservation in tumors ≤2 cm
- Chemoradiation is equally effective - equivalent OS but different morbidity profiles
- Adjuvant therapy indicated after surgery if intermediate or high-risk pathologic factors found
8.4 Locally Advanced (IB3, IIA2, IIB-IVA)
- Concurrent cisplatin-based chemoradiation is the standard of care
- Cisplatin 40 mg/m² weekly during external beam radiation
- External beam pelvic radiation (45-50 Gy) + intracavitary brachytherapy boost
- Para-aortic extended field radiation for IIIC2 disease
8.5 Barrel-Shaped Cervix (>6 cm)
-
17.5% central failure rate with radiation alone
-
Option: External radiation (4000 cGy) + single intracavitary treatment → extrafascial hysterectomy 2-3 months later
-
Central failure rate with combined approach: ~2%
-
Berek & Novak's Gynecology, p. 2266-2272
9. RADICAL HYSTERECTOMY - SURGICAL ANATOMY
The Wertheim/Type III radical hysterectomy involves:
- Removal of uterus, upper third of vagina, parametria, and uterosacral ligaments
- Bilateral pelvic lymphadenectomy (obturator, external iliac, internal iliac, common iliac)
- Development of paravesical and pararectal spaces:
- Paravesical space - bordered by obliterated umbilical artery medially, obturator internus laterally, cardinal ligament posteriorly, pubic symphysis anteriorly
- Pararectal space - bordered by rectum medially, cardinal ligament anteriorly, hypogastric artery laterally, sacrum posteriorly
- Ureteral dissection out of the vesicouterine ligament tunnel ("unroofing the ureter")
- Mobilization of bladder off the upper third of the vagina (critical early step)
Para-aortic lymph node evaluation - performed prior to radical hysterectomy; positive nodes on frozen section may redirect treatment to chemoradiation.
Nerve-sparing radical hysterectomy - preserves autonomic pelvic nerves; associated with improved bladder function and sexual function with no compromise in oncologic outcomes (meta-analysis confirmed). Berek & Novak's, p. 2285
10. SPECIAL CLINICAL SITUATIONS
10.1 Cervical Cancer During Pregnancy
- Management depends on gestational age and stage at diagnosis
- Early-stage disease (IA-IB1) in first/second trimester: may delay treatment to achieve fetal viability
- Radical hysterectomy can be performed during pregnancy
- Late second trimester or third trimester: delay treatment until fetal maturity, then classical cesarean section + radical hysterectomy
10.2 Cancer of the Cervical Stump (after supracervical hysterectomy)
- Rare; diagnosis and treatment are more complex due to altered anatomy
- Radiation therapy is preferred; surgery is technically difficult
- 5-year survival rates are similar to intact uterus cases when matched by stage
10.3 Barrel-Shaped Cervix
- As described in section 8.5 - combined chemoradiation + adjuvant extrafascial hysterectomy considered
10.4 Cervical Carcinoma After Extrafascial Hysterectomy
- Incidental finding after simple hysterectomy for presumed benign disease
- Management depends on stage: radiation or chemoradiation is usually required
- Survival after radiotherapy: 95-100% for microscopic disease, 82-84% for macroscopic disease with free margins, 20-47% with obvious residual cancer
11. RECURRENT CERVICAL CANCER
11.1 Site-Based Treatment
- Post-surgery recurrence → radiation therapy (external ± intracavitary); 25% 5-year survival
- Post-radiation central recurrence → surgical therapy (pelvic exenteration) is preferred curative option
11.2 Pelvic Exenteration
Three types:
- Anterior exenteration - removal of bladder, vagina, cervix, uterus
- Posterior exenteration - removal of rectum, vagina, cervix, uterus
- Total exenteration - removal of bladder + rectum + vagina + cervix + uterus (supralevator spares rectum; infralevator includes perineum)
Preoperative contraindications (the "triad of doom"):
- Unilateral leg edema
- Sciatic pain
- Ureteral obstruction These suggest pelvic sidewall fixation and are contraindications to exenteration.
Absolute contraindications: Metastatic disease beyond the pelvis, pelvic sidewall fixation, bilateral hydroureter.
11.3 Chemotherapy for Recurrent Disease
Recurrent cervical cancer is not curable with chemotherapy; it is palliative only.
| Regimen | Notes |
|---|---|
| Cisplatin + paclitaxel | Response rates up to 45%; most partial responses |
| Carboplatin + paclitaxel | Equally effective, less toxic than cisplatin doublet |
| Carboplatin + paclitaxel + bevacizumab | Improved survival but more toxic (GOG 240) |
- Berek & Novak's Gynecology, p. 2275-2278
12. ACUTE COMPLICATIONS AND EMERGENCIES
12.1 Acute Hemorrhage
- Biopsy to confirm neoplasia
- Vaginal pack with Monsel's solution (ferric subsulfate)
- External radiation therapy: 8-10 daily fractions at 180-200 cGy/day
- Broad-spectrum antibiotics to reduce infection
- Vascular embolization under fluoroscopy if severe
12.2 Ureteral Obstruction
- Bilateral obstruction with uremia: place percutaneous or transvesical ureteral catheters, then chemoradiation with curative intent
- Metastatic disease: stenting + palliative measures; median survival ~17 months with aggressive management
13. NEW UPDATES (2024-2025)
13.1 Immunotherapy - Major Paradigm Shift
KEYNOTE-826 (Pembrolizumab + Chemotherapy ± Bevacizumab for Persistent/Recurrent/Metastatic Disease)
- Pembrolizumab + chemotherapy ± bevacizumab significantly improved OS and PFS vs. chemotherapy ± bevacizumab in patients with PD-L1 CPS ≥1
- Now a standard first-line option for recurrent/metastatic disease
- [PMID: 38095881 - JAMA Oncol 2024]
KEYNOTE-A18 / ENGOT-cx11 / GOG-3047 (Pembrolizumab + Chemoradiation for Locally Advanced Disease)
- Pembrolizumab added to chemoradiation then continued as maintenance
- Phase III RCT in high-risk locally advanced cervical cancer (stages IIB-IVA, or IB2-IIA2 with node involvement)
- Significant improvement in PFS (HR 0.70, p=0.0020) reported in the Lancet 2024
- Overall survival benefit confirmed in updated Lancet Oct 2024 analysis [PMID: 39288779]
- This represents a major change from prior standard of care (cisplatin-chemoradiation alone)
EMPOWER-Cervical 1 / GOG-3016 (Cemiplimab for Recurrent Cervical Cancer)
- Cemiplimab vs. investigator's choice chemotherapy in recurrent disease
- Final OS analysis (2025): cemiplimab showed survival benefit in PD-L1+ tumors
- [PMID: 39798514 - Eur J Cancer 2025]
13.2 Sentinel Lymph Node Mapping
- Increasingly incorporated into management of early-stage (IA2-IB2) cervical cancer
- Technique: cervical injection of radiotracer and/or blue dye; sentinel nodes mapped bilaterally
- Can identify unexpected nodal drainage patterns
- Pathologic ultrastaging of sentinel nodes (serial sectioning + IHC) detects micrometastases missed by standard sectioning
- Recommended as alternative to full pelvic lymphadenectomy in selected cases (reflected in Berek & Novak Table 38-4)
13.3 Fertility-Sparing Surgery Updates
- Radical trachelectomy (vaginal or abdominal) is standard for IB1 tumors ≤2 cm
- Simple trachelectomy may be adequate for tumors < 2 cm with favorable features (ongoing trials)
- Neoadjuvant chemotherapy followed by fertility-sparing surgery is investigational
13.4 Bevacizumab in First-Line (LACC)
- GOG 240 established bevacizumab + cisplatin + paclitaxel as standard for recurrent/metastatic disease - confirmed in 2024 KEYNOTE-826 subanalysis
13.5 HPV Vaccination - Updated Evidence
- A 2025 Cochrane network meta-analysis (PMID: 41276263) confirmed HPV vaccination efficacy for cervical cancer prevention across 9-valent, quadrivalent, and bivalent vaccines
- 9-valent vaccine (Gardasil-9) is the current preferred vaccine in most countries
- WHO recommends a single-dose schedule for girls aged 9-14 years as an alternative to the 2-dose schedule (updated 2022/2024 guidance)
14. FOLLOW-UP AFTER PRIMARY TREATMENT
- Years 1-2: Every 3-4 months clinical examination
- Years 3-5: Every 6 months
- After 5 years: Annually
- Pap smear/vaginal vault cytology at each visit (sensitivity limited after radiation)
- CT or PET/CT for suspected recurrence
- MRI preferred for local recurrence assessment
- Most recurrences occur within 2 years (>80%)
SUMMARY TABLE - KEY NUMBERS
| Parameter | Value |
|---|---|
| HPV in cervical SCC | Up to 99% |
| HPV 16/18 in cervical Ca | ~70% |
| IA1 LN metastasis rate | < 1% |
| IA2 LN metastasis rate | 3-8% |
| IB LN metastasis rate | 15-20% |
| 5-yr survival, negative nodes | 85-90% |
| 5-yr survival, positive nodes | 20-74% |
| 5-yr survival Stage IA | 95-99% |
| 5-yr survival Stage IB | 80-90% |
| 5-yr survival Stage IIB | 65-75% |
| 5-yr survival Stage IIIB | 30-40% |
| 5-yr survival Stage IVA | 15-20% |
Sources:
- Berek JS, Hacker NF. Berek & Novak's Gynecology, 16th ed. Chapter 38: Cervical Cancer. Wolters Kluwer. (p. 2217-2280)
- Bhatla N, Berek JS, et al. Revised FIGO staging for carcinoma of the cervix uteri. Int J Gynecol Obstet 2019.
- Lorusso D et al. KEYNOTE-A18/ENGOT-cx11/GOG-3047. Lancet 2024 [PMID: 38521086, 39288779]
- Tewari KS et al. KEYNOTE-826 subgroup analyses. JAMA Oncol 2024 [PMID: 38095881]
- Oaknin A et al. EMPOWER-Cervical 1 final OS. Eur J Cancer 2025 [PMID: 39798514]
- Bergman H et al. HPV vaccination Cochrane network meta-analysis. Cochrane Database Syst Rev 2025 [PMID: 41276263]
This is a shared conversation. Sign in to Orris to start your own chat.