Aspirin induced peptic ulcer disease
"aspirin" AND "peptic ulcer" AND "gastroprotection"
Aspirin-Induced Peptic Ulcer Disease
Overview
Mechanism of Mucosal Injury
1. Systemic (Pharmacological) Mechanism - COX-1 Inhibition
- Stimulating mucus and bicarbonate secretion
- Maintaining mucosal blood flow
- Promoting epithelial restitution
2. Topical (Local) Mechanism
COX-1 vs. COX-2
| Isoform | Expression | Role |
|---|---|---|
| COX-1 | Constitutive (platelets, gastric mucosa) | Cytoprotective prostaglandins, TXA2 |
| COX-2 | Inducible (inflammation, endothelium) | Pro-inflammatory PGs, prostacyclin |
Epidemiology and Risk
- Asymptomatic peptic ulceration develops in 10-20% of people taking frequent NSAIDs/aspirin
- Ulcer-related complications (bleeding, perforation) develop in 1-2% per year - Katzung's Basic and Clinical Pharmacology 16th Ed., p. 2330
- The overall risk of major bleeding with aspirin is 1-3% per year - Harrison's 22E, p. 2546
- Bleeding risk increases 2-3 fold with dual antiplatelet therapy (e.g., aspirin + clopidogrel) or aspirin + anticoagulant
- Chronic NSAID/aspirin users, typically elderly patients, often present with bleeding or perforation without prior symptoms - Sleisenger and Fordtran's, p. 943
Risk Factors for Aspirin-Induced Ulcer Complications
| Risk Factor | Notes |
|---|---|
| Age > 65 years | Severity, case fatality, and poor functional outcome increase significantly after age 75 |
| Prior PUD or ulcer bleeding | Highest risk category |
| Concomitant corticosteroids | Multiplicatively increases NSAID risk |
| Concomitant anticoagulants | Increases bleeding risk 2-3x |
| Dual antiplatelet therapy | Clopidogrel + aspirin |
| High NSAID dose | Dose-related toxicity |
| H. pylori co-infection | Synergistic - H. pylori infection increases ulcer risk in aspirin users |
H. pylori and Aspirin: A Synergistic Risk
Clinical Features
- Epigastric pain (often worse at night, relieved by food/antacids)
- Dyspepsia, bloating, fullness
- Many patients - especially elderly chronic users - are asymptomatic until complications arise
- Complications: Upper GI bleeding (melena, hematemesis), perforation, gastric outlet obstruction
Diagnosis
- EGD (esophagogastroduodenoscopy) is the gold standard - more sensitive and specific than barium studies
- Biopsy from gastric ulcers to exclude malignancy
- Test for H. pylori in all patients (CLO test, urea breath test, fecal antigen)
- Rockall score used to stratify rebleeding and mortality risk
Management
Acute Treatment
- Discontinue aspirin if possible - allows more reliable healing
- PPI therapy is first-line:
- Heals >90% of duodenal ulcers within 4 weeks
- Heals ~90% of gastric ulcers within 6-8 weeks
- In patients who must continue aspirin/NSAID, PPIs more reliably promote healing than H2 blockers
- H2-receptor antagonists - effective if aspirin is stopped, less effective if it must be continued
- Rebleeding risk: For high-risk stigmata (visible vessel, adherent clot), give PPI bolus (e.g., esomeprazole 80 mg IV) followed by continuous infusion (8 mg/hour) for 3-5 days - Katzung 16th Ed., p. 2335
When Aspirin Cannot Be Stopped (Cardiovascular Indication)
- Continue lowest effective aspirin dose (75-100 mg daily)
- Add a once-daily PPI - effectively reduces incidence of ulcers and complications
- Eradicate H. pylori if present
- Do not substitute enteric-coated aspirin thinking it protects against GI bleeding - it does not
Prevention Strategies
Low GI Risk
- Age < 65, no prior PUD, no concomitant risk factors
- Aspirin alone at lowest effective dose
Intermediate GI Risk (1-2 risk factors)
- Age ≥ 65, or chronic/high-dose therapy, or concurrent aspirin with NSAID
- Traditional NSAID/aspirin + PPI or misoprostol
High GI Risk (> 2 risk factors or prior complicated ulcer)
- Requiring low-dose aspirin: Avoid all other NSAIDs; use PPI or misoprostol
- Not requiring aspirin: Avoid NSAIDs if possible; if mandatory, use COX-2 inhibitor + PPI
Important caveats:
- Sucralfate and enteric-coated aspirin are ineffective for preventing NSAID/aspirin-associated gastric ulcers
- COX-2 inhibitors lose their GI protection benefit when aspirin is co-administered (since concurrent aspirin requires COX-1 to be inhibited anyway)
- For patients on aspirin + clopidogrel, use a PPI (prefer pantoprazole over omeprazole to minimize CYP2C19 interaction with clopidogrel, though the COGENT trial showed omeprazole reduced GI events by 66% without a significant cardiovascular signal)
- Misoprostol (prostaglandin E1 analogue, 200 mcg QID) has similar efficacy to PPIs but requires four-times-daily dosing and frequently causes diarrhea - limiting clinical use
Summary Table
| Aspect | Key Point |
|---|---|
| Primary mechanism | COX-1 inhibition → loss of cytoprotective PGE2/PGI2 |
| Aspirin dose and GI risk | Dose-related; even 75 mg has GI risk |
| Enteric coating | Reduces topical damage only - does NOT prevent systemic GI bleeding |
| Treatment (aspirin stopped) | PPI or H2 blocker |
| Treatment (aspirin continued) | PPI (more effective than H2 blocker) |
| Prevention first-line | Lowest effective aspirin dose + once-daily PPI |
| H. pylori | Synergistic risk - test and eradicate in all aspirin/NSAID users |
| Most dangerous group | Elderly, asymptomatic until bleeding/perforation |
Generate a comparison poster: aspirin vs. COX-2 selective inhibitors for GI safety
Medical comparison poster: Aspirin vs. COX-2 Selective Inhibitors for GI Safety. Clean clinical infographic style with two clearly divided columns. Left column labeled "Aspirin (Non-selective COX inhibitor)" with red accent color, right column labeled "COX-2 Selective Inhibitors (e.g. Celecoxib)" with blue/teal accent color. Top section: Mechanism of Action - Left: Irreversibly inhibits both COX-1 and COX-2. COX-1 inhibition depletes cytoprotective prostaglandins PGE2 and PGI2 in gastric mucosa. Diagram showing COX-1 blocked leading to reduced mucus, reduced bicarbonate, reduced mucosal blood flow. Right: Selectively inhibits COX-2 only. COX-1 remains active, preserving gastric mucosal protection. Middle section titled "GI Safety Profile" with comparison rows: - Gastric/Duodenal Ulcer Risk: Aspirin: 10-20% asymptomatic ulceration with regular use | COX-2: Ulcer rate reduced by ~74% vs non-selective NSAIDs - GI Bleeding Risk: Aspirin: 1-3% per year major bleeding | COX-2: Significantly reduced GI bleeding risk - Enteric Coating Effect: Aspirin: Reduces topical injury only; does NOT prevent systemic GI bleeding | COX-2: N/A - Effect with concurrent Aspirin: Aspirin: Compounded risk | COX-2: GI protection is ELIMINATED when co-administered with low-dose aspirin - H. pylori interaction: Both: Synergistic risk - eradicate before/during therapy Bottom section "Prevention & Clinical Notes": - Aspirin: Use lowest effective dose (75-100mg); add PPI for intermediate/high GI risk patients; test and treat H. pylori - COX-2: Preferred over non-selective NSAIDs for GI protection; add PPI in high-risk patients; NOT protective if aspirin also prescribed - Warning box: COX-2 inhibitors carry INCREASED cardiovascular thrombotic risk with long-term use Footer: "Both drug classes require individualized risk assessment balancing GI vs. cardiovascular safety" Professional medical poster, dark navy background with white text and colored accent boxes, clear icons for stomach/GI tract, bold headers, evidence-based data points
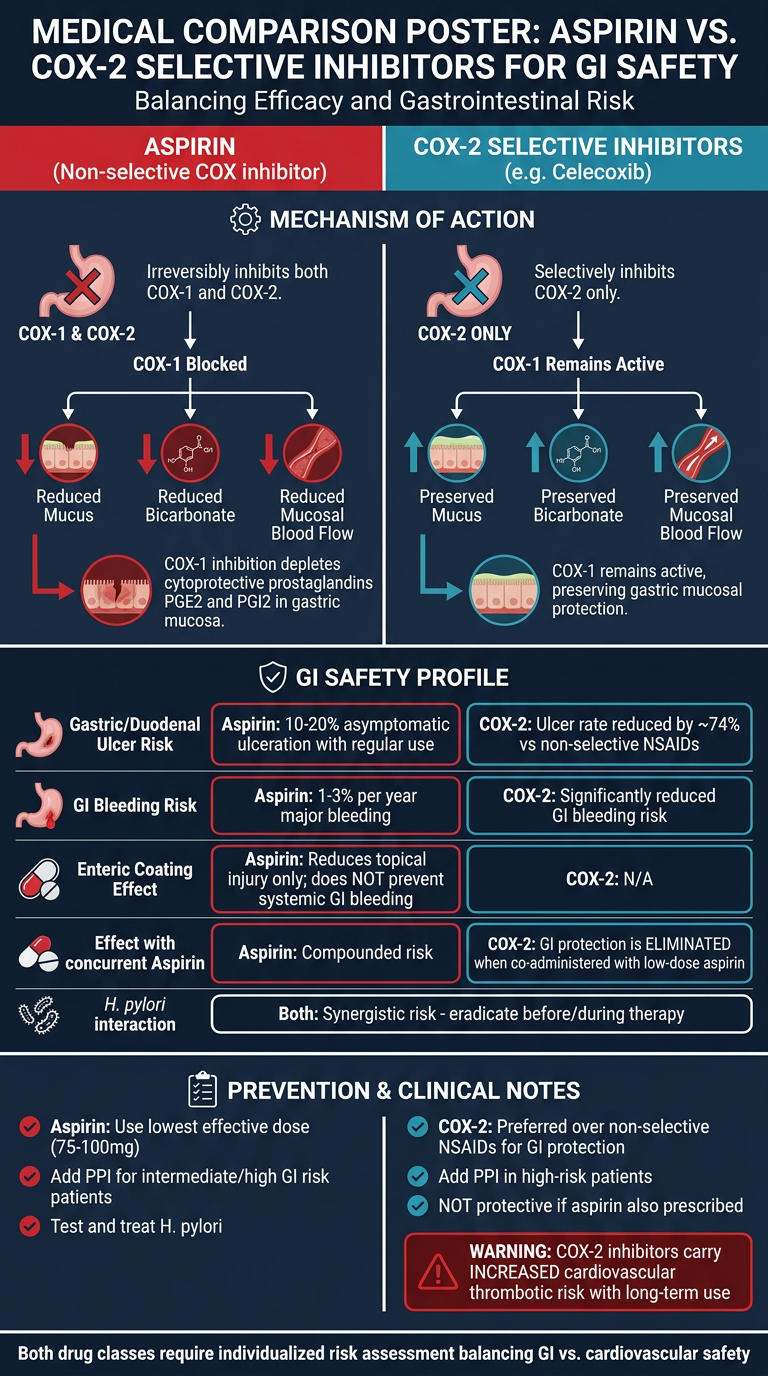
- Aspirin causes asymptomatic ulceration in 10-20% of regular users and major GI bleeding in 1-3% per year
- COX-2 inhibitors reduce ulcer rates by ~74% vs. non-selective NSAIDs
- Critical caveat: The GI benefit of COX-2 inhibitors is completely lost when co-prescribed with low-dose aspirin, since aspirin still inhibits COX-1
- Enteric-coated aspirin only reduces topical mucosal damage - it does not prevent systemic GI bleeding
- H. pylori co-infection is synergistic with both drug classes - always test and eradicate
- Both require PPI co-prescribing in high-risk patients