ascitis tapping
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Here is a comprehensive guide to Ascites Tapping (Abdominal Paracentesis):
Abdominal Paracentesis (Ascitic Tap)
Paracentesis is the procedure of inserting a needle or catheter into the peritoneal cavity to remove ascitic fluid for diagnostic analysis or therapeutic relief.
Types
| Type | Volume Removed | Purpose |
|---|---|---|
| Diagnostic | Small (~20-50 mL) | Fluid analysis - new-onset ascites, suspected SBP |
| Therapeutic (LVP) | >5 L (up to 10-12 L) | Relieve cardiorespiratory symptoms from tense ascites |
Indications
- New onset ascites (diagnostic workup)
- Suspected spontaneous bacterial peritonitis (SBP)
- To relieve cardiorespiratory and GI manifestations of tense ascites (therapeutic)
Contraindications
- Uncorrected coagulopathy with clinically evident fibrinolysis or DIC
- Bowel dilation or obstruction
- Pregnancy (technique must be modified - supraumbilical or US-guided approach)
- Abdominal hematoma, engorged veins, or superficial infection at the intended puncture site
Note: Routine coagulopathy (elevated PT, low platelets) is NOT a contraindication unless there is clinical evidence of active fibrinolysis or DIC. Studies show no increased bleeding risk with platelets >19,000/mm³ or PT <40 seconds.
Equipment
- Antiseptic solution + sterile drape
- Local anesthetic (lidocaine)
- 18-22 gauge needle (diagnostic) / 15-gauge steel or over-the-needle catheter (therapeutic)
- 20-50 mL syringe
- Vacuum bottles or drainage bag (for LVP)
- Blood culture bottles (for culture at bedside)
Site of Entry
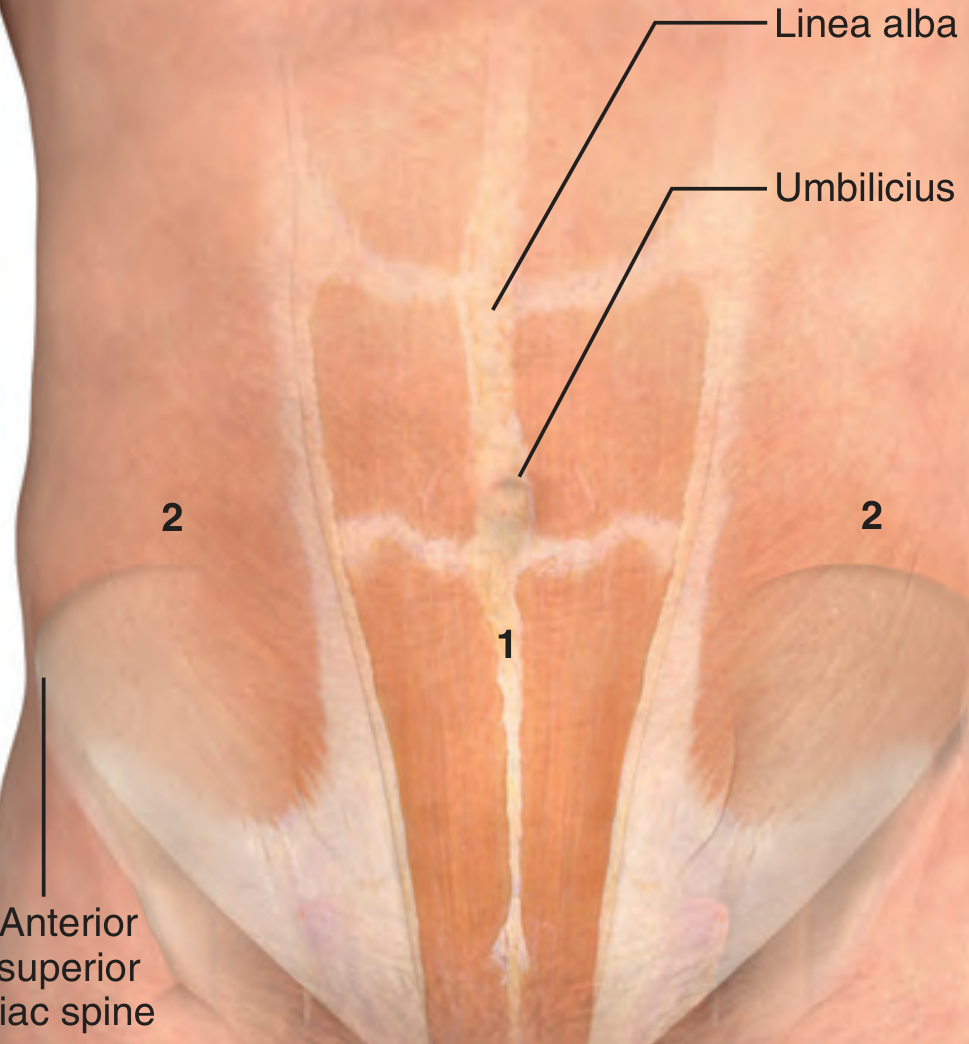
Two preferred sites:
- Midline (primary) - 2 cm below umbilicus along the linea alba (avascular, fibrous)
- Left/right lower quadrant (alternative) - 4-5 cm cephalad and medial to the anterior superior iliac spine, lateral to the rectus sheath (to avoid the inferior epigastric artery)
- Avoid midline if there is scarring, collateral veins, or previous complications at that site
- Left lower quadrant is generally preferred over right (less risk of cecal perforation)
Technique
Pre-procedure:
- Patient voids before the procedure
- Position: supine (large ascites) or lateral decubitus (smaller amounts)
- Clean the site with antiseptic; apply sterile drape; infiltrate local anesthetic
Needle insertion:
Standard method - Insert needle perpendicular to the skin (70-90° angle), advance in 5-mm increments while aspirating until fluid returns.
Z-tract method (preferred to prevent leaks):
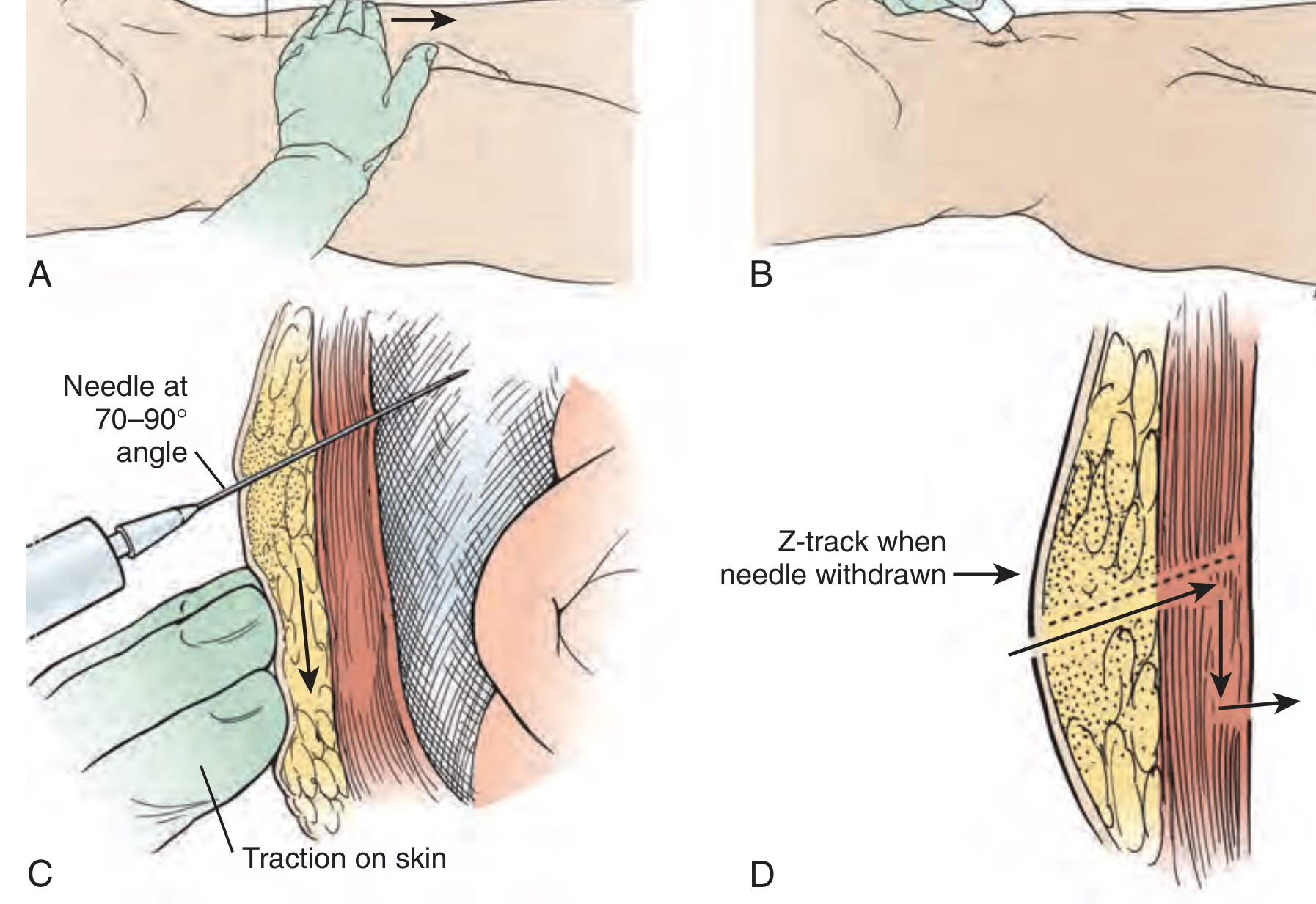
- With the non-needle hand, pull the skin ~2 cm caudally
- Insert the needle slowly while traction is maintained
- Once fluid flows, release the skin - the needle will angle caudally
- On withdrawal, displaced skin seals the tract, preventing persistent leaks
During drainage:
- Avoid continuous suction (attracts bowel/omentum, causing occlusion)
- If flow stops, gently rotate the needle and advance 1-2 mm
- Stabilize the needle once fluid is flowing freely
Post-procedure:
- Remove needle; apply adhesive bandage
- For persistent fluid leak: pressure bandage or cyanoacrylate adhesive; position the site non-dependently and apply pressure for 10 minutes first
Ultrasound Guidance
US-guided paracentesis is recommended for:
- Suspected adhesions or bowel obstruction
- Small or loculated fluid collections
- Patients at higher risk (prior abdominal surgery)
Scan using a low-frequency probe; confirm the largest safe fluid pocket, absence of overlying bowel (bowel floats; air causes scatter artifact), and adequate bladder emptying. Mark the skin and perform the procedure promptly (fluid shifts over time).
Volume of Fluid Removed
- Diagnostic tap: 20-50 mL sufficient
- Therapeutic LVP: Remove as much as possible without excessive manipulation; 5-6 L is routine and well tolerated; up to 10-12 L can be removed safely in most patients with chronic ascites
- For LVP >5 L: administer albumin infusion (6-8 g per litre removed) to prevent paracentesis-induced circulatory dysfunction (PICD)
Fluid Analysis (Send Routinely)
| Test | Use |
|---|---|
| Cell count + differential | SBP: PMN >250/μL diagnostic |
| Albumin | Calculate SAAG (>1.1 g/dL = portal hypertension, >95% accuracy) |
| Culture (blood culture bottles at bedside) | Most sensitive method for infection |
| Cytology | Malignant ascites workup |
| Triglyceride | Chylous ascites |
| Tuberculosis smear + culture | Immunocompromised/endemic regions |
Optional: total protein, glucose, LDH, amylase, Gram stain
Unhelpful routinely: pH, lactate, cholesterol, fibronectin
Serum-Ascites Albumin Gradient (SAAG)
SAAG = Serum albumin - Ascites albumin
- >1.1 g/dL → Portal hypertension (cirrhosis, CHF, Budd-Chiari, constrictive pericarditis)
- <1.1 g/dL → Non-portal hypertension cause (malignancy, TB, nephrotic syndrome, pancreatitis)
Complications
Systemic:
- Hyponatremia
- Renal dysfunction
- Hepatic encephalopathy
- Hemodynamic compromise (PICD after LVP)
- Significant bleeding, death (rare)
Local:
- Persistent ascitic fluid leak at wound site
- Abdominal wall hematoma
- Localized infection
Intraperitoneal:
- Perforation of vessels or viscera
- Generalized peritonitis
- Abdominal wall abscess
Causes of Ascites (for Context)
- Elevated hydrostatic pressure: Cirrhosis, CHF, constrictive pericarditis, IVC obstruction, Budd-Chiari syndrome
- Decreased osmotic pressure: Nephrotic syndrome, protein-losing enteropathy, malnutrition
- Fluid production exceeding resorption: Bacterial/TB/parasitic infections, neoplasms, hemorrhagic pancreatitis
Sources: Roberts and Hedges' Clinical Procedures in Emergency Medicine; Pfenninger and Fowler's Procedures for Primary Care, 3rd ed.
What ascitic fluid findings suggest malignant ascites vs portal hypertension?
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Excellent data gathered. Here is the complete comparison:
Ascitic Fluid Findings: Malignant Ascites vs Portal Hypertension
The Core Test: SAAG (Serum-Ascites Albumin Gradient)
SAAG = Serum albumin - Ascitic fluid albumin (both measured on the same day)
| SAAG | Interpretation |
|---|---|
| ≥ 1.1 g/dL (High gradient) | Portal hypertension - >97% specificity |
| < 1.1 g/dL (Low gradient) | Non-portal cause: malignancy, TB, nephrotic syndrome, pancreatitis |
The SAAG reflects hepatic sinusoidal pressure via Starling forces. In cirrhosis, "capillarization of sinusoids" reduces sinusoidal permeability to macromolecules, resulting in protein-poor ascites with a high SAAG.
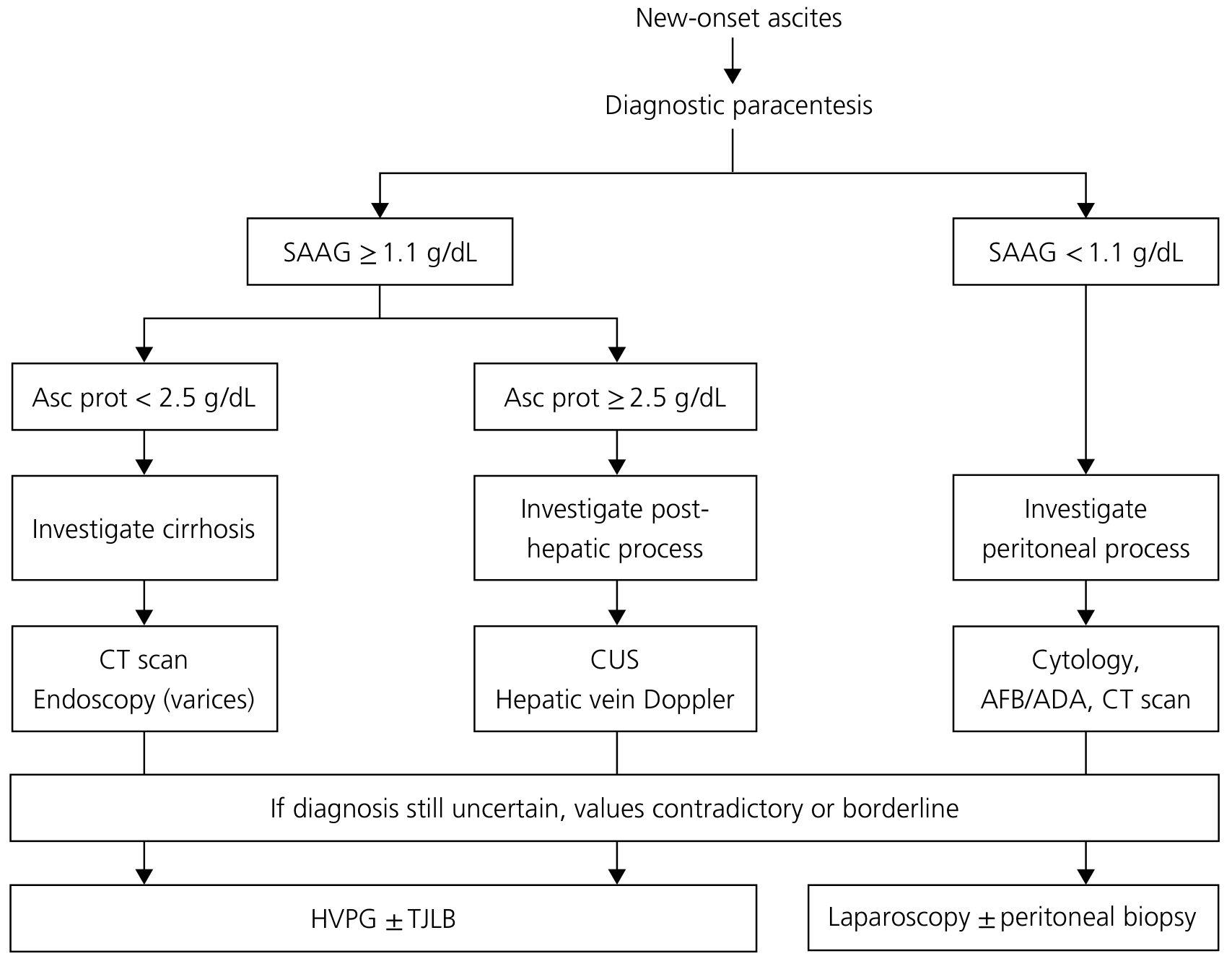
Diagnostic Algorithm
Detailed Comparison Table
| Parameter | Portal Hypertension (Cirrhosis) | Malignant Ascites (Peritoneal Carcinomatosis) | Cardiac Ascites |
|---|---|---|---|
| SAAG | ≥ 1.1 g/dL | < 1.1 g/dL | ≥ 1.1 g/dL |
| Total protein | Low < 2.5 g/dL | High > 2.5 g/dL | High ≥ 2.5 g/dL |
| Appearance | Clear, straw-yellow | Often bloody or turbid | Clear |
| WBC differential | Predominantly lymphocytes | Variable; can be mixed | Lymphocytes |
| PMN count | < 250/μL (if no SBP) | < 250/μL (unless co-infection) | < 250/μL |
| LDH (ascites:serum ratio) | ~0.4 (low) | ~1.0 or higher | Low |
| Glucose | Normal (~serum level) | Reduced (consumed by tumor cells) | Normal |
| Cytology | Negative | Positive in ~100% of peritoneal carcinomatosis (lower yield for liver metastases) | Negative |
| Red blood cells | Rare (unless HCC or varix rupture) | High - hemoperitoneum does not clot | Rare |
Key Differentiating Points in Detail
1. SAAG - The Most Reliable Test
- Portal hypertension (cirrhosis, Budd-Chiari, cardiac): SAAG ≥ 1.1 g/dL
- Malignancy, TB, pancreatitis, nephrotic syndrome: SAAG < 1.1 g/dL
- Important caveat: If the patient has both cirrhosis AND liver metastases (massive hepatic involvement/pseudocirrhosis), the SAAG can paradoxically be ≥ 1.1 g/dL due to portal hypertension from tumour-induced changes - this represents ~one-third of malignant ascites cases
2. Total Protein - Separates Cirrhosis from Cardiac/Malignant
- Cirrhosis: protein < 2.5 g/dL (fibrosed sinusoids limit protein leakage)
- Cardiac ascites: protein ≥ 2.5 g/dL with SAAG ≥ 1.1 g/dL (normal "leaky" sinusoids congested by back-pressure)
- Malignant/TB ascites: protein ≥ 2.5 g/dL with SAAG < 1.1 g/dL (leakage from inflamed/obstructed peritoneal lymphatics)
- Protein < 1.0-1.5 g/dL in cirrhosis = higher SBP risk
3. Cytology - Diagnostic for Malignancy
- Sensitivity approaches 100% for peritoneal carcinomatosis
- Much lower sensitivity for malignancy causing ascites via liver metastases or lymphatic obstruction (not peritoneal seeding)
- Yield improves with larger submitted volume
- If cytology is negative but clinical suspicion remains high (low SAAG + high protein + no infection): next step is laparoscopy with peritoneal biopsy
4. Glucose & LDH
- In malignancy: glucose is reduced (tumor cell consumption); LDH ratio ascites:serum ≈ 1.0 (vs ~0.4 in uncomplicated cirrhosis)
- These same criteria (glucose < 50 mg/dL + LDH > serum ULN + protein > 1 g/dL) also suggest secondary bacterial peritonitis from bowel perforation - must be interpreted with clinical context
5. Gross Appearance
| Appearance | Suggests |
|---|---|
| Clear, pale straw-yellow | Uncomplicated cirrhotic ascites |
| Bloody (does not clot) | Hemoperitoneum - malignancy (HCC, peritoneal carcinomatosis) |
| Bloody (clots) | Traumatic tap |
| Milky/chylous | Lymphatic obstruction - lymphoma, post-surgery |
| Cloudy/purulent | SBP or secondary bacterial peritonitis |
| Tea/black | Hemorrhagic pancreatitis |
| Bile-green | Gallbladder/intestinal perforation |
6. Cell Count Differential
- PMN predominance (≥ 250/μL): bacterial peritonitis (SBP or secondary)
- Lymphocyte predominance: tuberculous peritonitis, malignancy (lymphoma)
- For bloody ascites: subtract 1 PMN per 250 RBC to correct the count
Important Caveats & Pitfalls
- SAAG accuracy is reduced if samples are not taken simultaneously, if serum albumin is very low, or if ascites is chylous (falsely high SAAG)
- Serum hyperglobulinemia (>5 g/dL) narrows the albumin gradient falsely; correct with: SAAG × (0.16 × serum globulin + 2.5)
- CA-125 is elevated in ALL causes of ascites (not specific for ovarian cancer in this context) - do not use to diagnose malignant ascites
- CEA, fibronectin, cholesterol are nonspecific and unhelpful in distinguishing malignant ascites
- CT findings that suggest malignant ascites: fluid in the omental bursa, peritoneal thickening/enhancement, increased fluid density, loss of bowel loop mobility
Quick Summary: The 2-Step Rule
Step 1 - SAAG: ≥ 1.1 → portal hypertension pathway | < 1.1 → peritoneal process (malignancy/TB)Step 2 - Ascites Protein: If SAAG ≥ 1.1 → protein < 2.5 = cirrhosis; protein ≥ 2.5 = cardiac/Budd-Chiari. If SAAG < 1.1 → send cytology, AFB/ADA; consider CT and laparoscopy
Sources: Yamada's Textbook of Gastroenterology, 7th ed.; Frameworks for Internal Medicine; Harrison's Principles of Internal Medicine, 22nd ed. (2025); The Washington Manual of Medical Therapeutics; Bailey and Love's Short Practice of Surgery, 28th ed.
This is a shared conversation. Sign in to Orris to start your own chat.