Reading File
Asking for Preferences
Teach me these topics
Running Command
python -m markitdown "/home/daytona/workspace/attachments/b17440b4-55b7-4b48-9b7…
Running Command
cd /home/daytona/workspace && python3 -c " from pptx import Presentation import …
Running Command
ls /home/daytona/skills/pptx/scripts/ && echo "---" && which python3 && python3 …
Running Command
ls /home/daytona/skills/pptx/scripts/office/ && cat /home/daytona/skills/pptx/sc…
Running Command
cd /home/daytona/skills/pptx && python3 scripts/office/unpack.py "/home/daytona/…
Running Command
cd /home/daytona/workspace && python3 -c " import zipfile, os def extract_text_…
I have all the content. Now let me teach you both topics in a structured, clear way.
Module 2 - Topic 3: Muscles of the Thorax
1. Intrinsic Thoracic Muscles
These muscles live entirely within the thoracic wall. Their primary job is moving the ribs during breathing.
| Muscle | Notes |
|---|---|
| External intercostals | Elevate ribs during inspiration |
| Internal intercostals | Depress ribs during forced expiration |
| Subcostal muscles | Deep to internal intercostals; depress ribs |
| Transversus thoracis | Depresses costal cartilages |
2. Extrinsic (Axioappendicular) Muscles
These originate from the thorax but act on the upper limb - or vice versa. They are also called axioappendicular muscles because they connect the axial skeleton to the appendicular (limb) skeleton.
Key muscles:
Pectoralis Major
- Large fan-shaped muscle covering the anterior chest
- Adducts and medially rotates the arm
Pectoralis Minor
- Lies deep to pectoralis major
- Originates: ribs 3-5
- Inserts: coracoid process of scapula
- Also acts as a secondary respiratory muscle - assists elevation of ribs 3-5
- Clinical: Poland syndrome = congenital absence of pectoralis muscles, associated with brachydactyly (short fingers) and sometimes dextrocardia (heart on right side)
Serratus Anterior
- Originates: ribs 1-8/9 (lateral surface)
- Inserts: medial border of scapula (anterior/costal surface)
- Action: protracts and rotates the scapula upward (essential for raising arm above 90°)
- Clinical: Long thoracic nerve (C5-C7) innervates it. Damage causes Winged Scapula - the medial border of the scapula sticks out like a wing because it can no longer be held flat against the thorax.
3. Scalene Muscles
Three muscles (anterior, middle, posterior) that connect the cervical vertebrae to the first two ribs.
- Primarily: flex and rotate the neck
- Secondary respiratory role: elevate ribs 1-2 during forced inspiration
4. The Diaphragm
The most important respiratory muscle. A dome-shaped musculotendinous sheet separating the thoracic and abdominal cavities.
Attachments (origins):
- Ligamentum arcuatum medianum - bridges the two crura over the aorta
- Ligamentum arcuatum medialis - over the psoas major muscle
- Ligamentum arcuatum lateralis - over the quadratus lumborum muscle
- Also attaches to the xiphoid process and lower 6 costal cartilages
Three major openings (and what passes through each):
| Opening | Level | Structures |
|---|---|---|
| Aortic hiatus | T12 | Aorta, thoracic duct, azygos vein |
| Esophageal hiatus | T10 | Esophagus, vagus nerves |
| Caval opening | T8 | Inferior vena cava, right phrenic nerve |
Mnemonic: "I 8 (ate) 10 eggs AT 12" - IVC at T8, Esophagus at T10, Aorta at T12
Clinical - Congenital Diaphragmatic Hernia (CDH):
- Failure of the diaphragm to fully form during development
- Most common: Bochdalek hernia (posterolateral defect, usually left side)
- Abdominal organs herniate into the thorax, compressing the developing lungs - causes pulmonary hypoplasia
- Medical emergency in newborns
5. Respiratory Muscles Summary
Primary muscles (active in quiet breathing):
- Diaphragm - the main workhorse
- Intercostal muscles (external, internal, subcostal)
Secondary/accessory muscles (active in forced breathing):
| Muscle | Ribs assisted |
|---|---|
| Scalenes | 1-2 |
| Pectoralis minor | 3-5 |
| Anterior/posterior serratus | 6-8 |
| Latissimus dorsi | 9-10 |
| Quadratus lumborum | 11-12 |
Module 2 - Topic 4: Muscles of the Abdomen
1. Layers of the Anterior Abdominal Wall
From superficial to deep (memorize this order):
- Skin and subcutaneous tissue
- Superficial fascia - two layers:
- Camper's fascia (fatty layer) - continuous with superficial fat everywhere
- Scarpa's fascia (membranous layer) - fuses with fascia lata of the thigh below inguinal ligament
- External oblique muscle
- Internal oblique muscle
- Transversus abdominis muscle
- Transversalis fascia (deep fascia)
- Preperitoneal adipose tissue
- Parietal peritoneum
2. Congenital Defects of the Anterior Wall
| Feature | Gastroschisis | Omphalocele |
|---|---|---|
| Location | Para-umbilical (usually right side) | At the umbilicus (midline) |
| Covering sac | No - organs exposed | Yes - covered by a sac |
| Associations | Usually isolated | Associated with genetic syndromes |
3. The Four Anterior Abdominal Muscles
Rectus Abdominis
- Runs vertically, flanking the midline (linea alba)
- Origin: pubic crest, pubic tubercle, pubic symphysis
- Insertion: cartilage of 5th, 6th, 7th ribs and xiphoid process
- Action: flexes trunk, compresses abdomen, increases intra-abdominal pressure (coughing, Valsalva maneuver)
- The "6-pack" muscle - divided by tendinous intersections
Pyramidalis
- Small triangular muscle anterior to the lower rectus abdominis
- Origin: pubis
- Insertion: linea alba
- Action: tenses the linea alba
- Often absent (absent in ~20% of people)
External Oblique
- Most superficial of the lateral muscles
- Origin: 5th-12th ribs (outer surfaces)
- Insertion: lateral fibers - iliac crest; medial fibers form the external oblique aponeurosis
- Action: ipsilateral lateral flexion, contralateral rotation of trunk
- Think: "hands in pockets" orientation of fibers (diagonal, downward-forward)
- Its lower free border folds on itself to form the inguinal ligament
Internal Oblique
- Middle lateral muscle (between external oblique and transversus abdominis)
- Origin: lateral 2/3 of inguinal ligament, iliac crest, thoracolumbar fascia
- Insertion: lower costal cartilages; forms internal oblique aponeurosis contributing to rectus sheath; medial fibers fuse with transversus abdominis to form the conjoint tendon
- Action: ipsilateral lateral flexion AND ipsilateral rotation (opposite to external oblique for rotation)
Transversus Abdominis
- Deepest of the lateral muscles; fibers run horizontally
- Origin: lateral 1/3 of inguinal ligament, iliac crest, thoracolumbar fascia, lower 6 costal cartilages
- Insertion: upper fibers form aponeurosis contributing to rectus sheath; lower fibers join internal oblique to form the conjoint tendon
- Action: maintains abdominal wall tone and increases intra-abdominal pressure (no rotation)
4. Rectus Sheath
The rectus abdominis is enclosed in a fibrous tunnel formed by the aponeuroses of the three lateral muscles.
Above the arcuate line (upper 2/3 of abdomen):
- Anterior layer = external oblique aponeurosis + anterior lamina of internal oblique
- Posterior layer = transversus abdominis aponeurosis + posterior lamina of internal oblique
Below the arcuate line (lower 1/3):
- ALL three aponeuroses pass anterior to the rectus abdominis
- There is no posterior layer below the arcuate line
- The rectus is in direct contact with the transversalis fascia and peritoneum
The lateral edge of the rectus sheath = linea semilunaris (visible as a curved groove on the abdomen in muscular individuals).
5. Hernias of the Abdominal Wall
| Hernia | Location | Notes |
|---|---|---|
| Umbilical | Midline, at the umbilicus | Very common in infants; usually closes spontaneously |
| Epigastric | Linea alba, between xiphoid and umbilicus | Through a weakness in the linea alba |
| Incisional | Through a previous surgical scar | Post-operative complication |
| Spigelian | Along the semilunar line, near the arcuate line | Below the umbilicus |
| Grynfeltt hernia | Superior lumbar triangle (bounded by 12th rib, erector spinae, internal oblique) | Rare |
| Petit hernia | Inferior lumbar triangle (bounded by iliac crest, latissimus dorsi, external oblique) | Rare |
6. Inguinal Region
Inguinal Ligament
- Fibrous band from ASIS (anterosuperior iliac spine) to the pubic tubercle
- Formed by the folded lower free border of the external oblique aponeurosis
- The internal oblique and transversus abdominis originate from its lateral end
- Conjoint tendon = fusion of medial internal oblique + lower transversus abdominis fibers; reinforces the posterior wall of the inguinal canal medially
Inguinal Canal
A passage through the lower abdominal wall, ~4 cm long.
Contents:
- Males: spermatic cord
- Females: round ligament of the uterus
Walls:
| Wall | Structure |
|---|---|
| Anterior | External oblique aponeurosis + internal oblique (laterally) |
| Posterior | Transversalis fascia (laterally) + conjoint tendon (medially) |
| Roof (superior) | Internal oblique + transversus abdominis |
| Floor (inferior) | Inguinal ligament + lacunar ligament (medially) |
Rings:
- Deep (internal) ring: opening in the transversalis fascia, bounded superolaterally by transversalis fascia, inferomedially by inferior epigastric vessels
- Superficial (external) ring: triangular opening in the external oblique aponeurosis, at the medial aspect
Hesselbach's (Inguinal) Triangle
The weak area of the posterior inguinal wall where direct hernias push through.
Borders:
- Medially: rectus abdominis
- Laterally: inferior epigastric vessels
- Inferiorly: inguinal ligament
Inguinal Hernias
| Type | Path | Clinical Clue |
|---|---|---|
| Indirect | Through the deep inguinal ring, travels the full length of the inguinal canal | More common, especially in males; can enter the scrotum; lateral to inferior epigastric vessels |
| Direct | Pushes directly through the posterior wall of the canal (through Hesselbach's triangle) | Medial to inferior epigastric vessels; usually in older males due to weakened abdominal wall |
7. Umbilical Folds and Fossae (Internal View)
Looking at the inside of the anterior abdominal wall, you see 5 peritoneal folds converging toward the umbilicus:
| Fold | Structure Underneath | Significance |
|---|---|---|
| Median umbilical fold (1, midline) | Median umbilical ligament = obliterated urachus | Remnant of embryonic connection to bladder |
| Medial umbilical folds (2, one each side) | Medial umbilical ligaments = obliterated umbilical arteries | Fetal circulation remnants |
| Lateral umbilical folds (2, one each side) | Inferior epigastric artery and vein | Still functional blood vessels |
The fossae (depressions between folds):
- Supravesical fossa - between median and medial folds (size changes with bladder filling)
- Medial inguinal fossa (Hesselbach's triangle) - medial to lateral fold - site of direct inguinal hernia
- Lateral inguinal fossa - lateral to lateral fold - site of indirect inguinal hernia
8. Posterior Abdominal Muscles
| Muscle | Origin | Insertion | Action |
|---|---|---|---|
| Psoas major | T12-L4 vertebral bodies | Lesser trochanter of femur (with iliacus = iliopsoas) | Flexes thigh/trunk |
| Iliacus | Iliac fossa | Lesser trochanter (with psoas = iliopsoas) | Flexes thigh |
| Psoas minor | T12-L1 vertebrae | Pecten pubis, iliopubic ramus | Weak trunk flexion |
| Quadratus lumborum | Iliac crest | 12th rib, L1-L4 vertebrae | Lateral flexion of trunk; fixes 12th rib during breathing |
Quick Review - Key Clinical Pearls
- Winged scapula = serratus anterior palsy (long thoracic nerve damage)
- Poland syndrome = absent pectoralis + brachydactyly
- Congenital diaphragmatic hernia = organs in thorax, pulmonary hypoplasia
- Gastroschisis = no sac, para-umbilical; Omphalocele = has sac, at umbilicus
- Arcuate line = where posterior rectus sheath ends; below it, no posterior sheath
- Direct hernia = through Hesselbach's triangle, medial to epigastric vessels
- Indirect hernia = through deep inguinal ring, lateral to epigastric vessels
- Median fold = urachus; Medial folds = obliterated umbilical arteries; Lateral folds = inferior epigastric vessels (active!)
In detail
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have thorough textbook content and diagrams. Here is the complete, detailed lesson on both topics.
📘 Module 2 - Topic 3: Muscles of the Thorax (Detailed)
PART 1: Intrinsic Thoracic Wall Muscles
These muscles are native to the thoracic cage. Their fibers run between the ribs and their primary role is structural support and rib movement during breathing.
1. Intercostal Muscles
There are three layers in every intercostal space, named by depth:
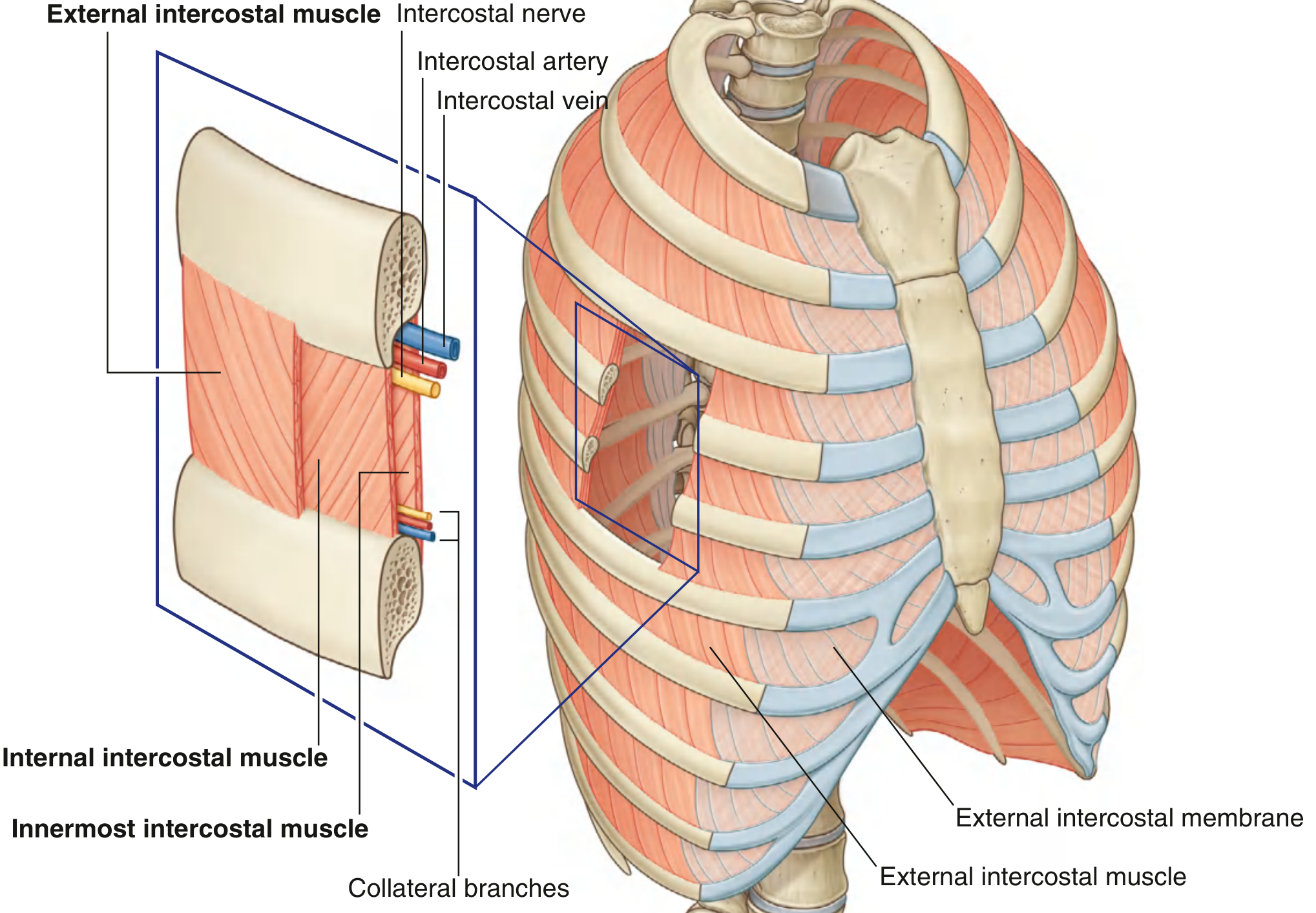
A. External Intercostal Muscles (most superficial)
- Attachment: From the inferior margin (lateral edge of costal groove) of the rib above → superior margin of the rib below
- Fiber direction: Obliquely anteroinferiorly (think: hands in front pockets - the direction fibers slope)
- Extent: From the tubercles of the ribs posteriorly all the way to the costal cartilages anteriorly. Beyond the cartilages, the muscle is replaced by a thin sheet of connective tissue = external intercostal membrane
- Function: Most active during inspiration - they elevate the ribs
- Innervation: Intercostal nerves T1-T11
B. Internal Intercostal Muscles (middle layer)
- Attachment: From the lateral edge of the costal groove of the rib above → superior margin of the rib below (deeper than external attachment)
- Fiber direction: Obliquely posteroinferiorly - opposite to external intercostals (the two sets cross each other like an "X")
- Extent: From the parasternal region (between costal cartilages) to the angle of the ribs posteriorly. Medial to the angle, replaced by the internal intercostal membrane
- Function: Most active during forced expiration - they depress the ribs
- Innervation: Intercostal nerves T1-T11
C. Innermost Intercostal Muscles (deepest layer)
- Fiber direction: Same as internal intercostals (posteroinferiorly)
- Extent: Most evident in the lateral thoracic wall; from the medial edge of the costal groove to the deep surface of the rib below
- Key anatomical point: The neurovascular bundle (intercostal vein, artery, nerve - VAN from top to bottom) travels in the costal groove in the plane BETWEEN the internal and innermost intercostals
- Function: Acts with internal intercostals (expiration)
- Innervation: Intercostal nerves T1-T11
Clinical pearl - Pleural tap (thoracentesis): Always insert the needle just above the upper border of the lower rib to avoid the neurovascular bundle that runs in the costal groove (inferior margin of each rib).
D. Subcostal Muscles
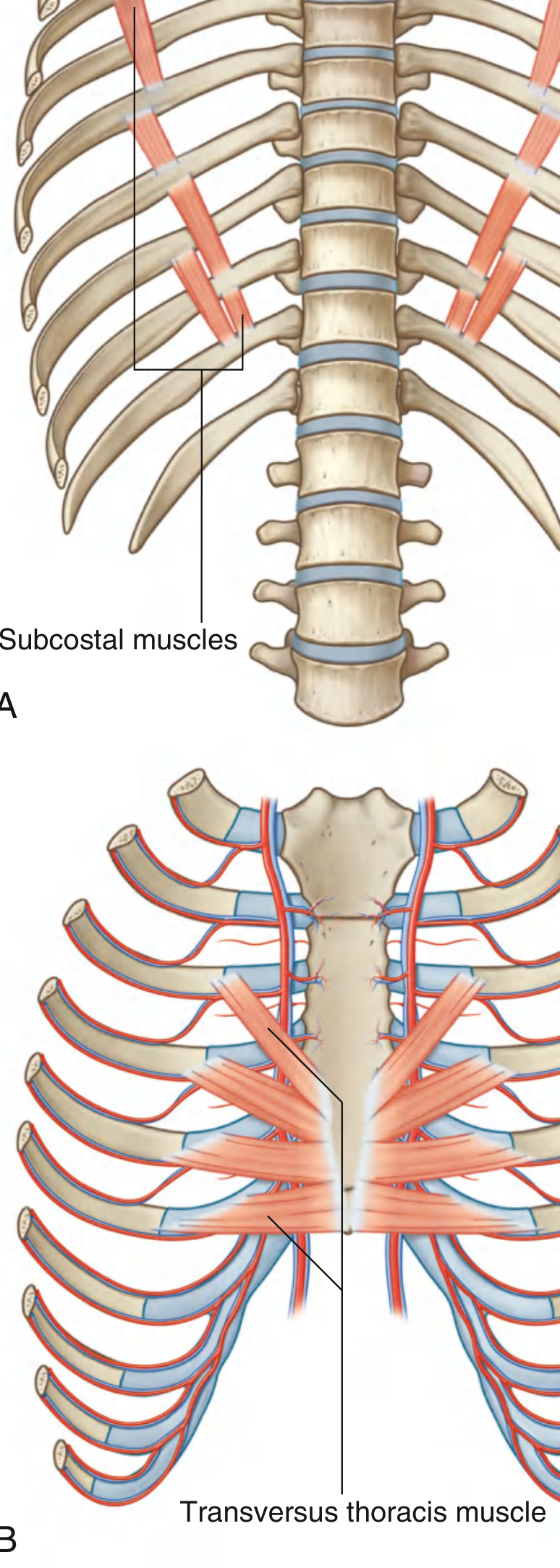
- Same plane as innermost intercostals
- More numerous in the lower posterior thoracic wall
- They span 2-3 ribs (from one rib to the 2nd or 3rd rib below) - unlike intercostals which only span one space
- Function: May depress ribs
E. Transversus Thoracis Muscles
- Found on the deep surface of the anterior thoracic wall (same plane as innermost intercostals)
- Origin: Posterior surface of xiphoid process, inferior sternum body, and adjacent costal cartilages of lower ribs
- Insertion: Lower borders and internal surfaces of costal cartilages of ribs 2-6 (passing superolaterally)
- Function: Depresses costal cartilages (expiration)
Summary Table of Intrinsic Thoracic Wall Muscles (from Gray's Anatomy for Students):
| Muscle | Attachment: Superior | Attachment: Inferior | Innervation | Function |
|---|---|---|---|---|
| External intercostal | Inferior margin of rib above | Superior margin of rib below | T1-T11 | Inspiration; elevates ribs |
| Internal intercostal | Lateral edge of costal groove, rib above | Superior margin of rib below | T1-T11 | Expiration; depresses ribs |
| Innermost intercostal | Medial edge of costal groove, rib above | Internal surface of rib below | T1-T11 | With internal intercostals |
| Subcostales | Internal surface near angle, lower ribs | Internal surface 2nd or 3rd rib below | Related intercostal nn. | May depress ribs |
| Transversus thoracis | Lower costal cartilages 2nd-6th | Inferior sternum, xiphoid, costal cartilages IV-VII | Related intercostal nn. | Depresses costal cartilages |
2. The Intercostal Neurovascular Bundle
Within each intercostal space, the nerve, artery, and vein travel together in the costal groove (on the underside of each rib) - between the internal and innermost intercostals.
Order from top to bottom in the groove: VAN (Vein - Artery - Nerve)
Blood supply:
- Posterior intercostal arteries (spaces 3-11): Arise from the thoracic aorta (the right-sided ones are longer because the aorta lies on the left)
- Anterior intercostal arteries (spaces 1-6): Branch from the internal thoracic artery; spaces 7-9 from the musculophrenic artery
- The internal thoracic artery arises from the subclavian artery, descends ~1 cm lateral to the sternum posterior to the costal cartilages, and terminates at the 6th intercostal space as the superior epigastric artery (entering the abdominal wall) and musculophrenic artery
Venous drainage: Mirrors arterial supply; posterior intercostal veins drain into the azygos system; anterior veins drain into the internal thoracic veins → brachiocephalic veins.
PART 2: Extrinsic (Axioappendicular) Thoracic Muscles
These muscles connect the trunk (axial skeleton) to the upper limb (appendicular skeleton), or vice versa. They live on the thoracic wall but act primarily on the arm or shoulder girdle - and several double as accessory respiratory muscles.
1. Pectoralis Major
- Large, fan-shaped, covers the anterior chest
- Two heads: clavicular (upper) and sternocostal (lower)
- Action: adduction, medial rotation, and flexion of the arm
- As an accessory respiratory muscle: when the arms are fixed (hands on knees), it can help elevate the thorax during forced inspiration - this is why people with respiratory distress instinctively brace their arms
2. Pectoralis Minor
- Lies deep to pectoralis major
- Origin: Anterior surfaces of ribs 3, 4, and 5 (near their costal cartilages)
- Insertion: Medial border and superior surface of the coracoid process of the scapula
- Action: Depresses and protracts the shoulder; tilts the scapula anteriorly
- Accessory respiratory role: With the shoulder fixed, it elevates ribs 3-5 during forced inspiration
Clinical: Poland Syndrome - Congenital unilateral absence of the pectoralis major (and sometimes minor). Associated with ipsilateral brachydactyly (abnormally short fingers), skin/soft tissue defects of the chest wall, and occasionally dextrocardia (rightward displacement of the heart). Rare (1 in 20,000 births).
3. Serratus Anterior
- Origin: Lateral surfaces of ribs 1-8 (or 9), appearing as serrated "teeth" of muscle
- Insertion: Costal surface (anterior aspect) of the medial border of the scapula
- Action: Protracts the scapula (pulls it forward around the chest wall); rotates the glenoid cavity upward (essential for raising the arm above 90°); holds the scapula flat against the thorax
- Innervation: Long thoracic nerve (C5, C6, C7) - runs superficially down the lateral chest wall
Clinical: Winged Scapula - Damage to the long thoracic nerve (e.g., from a stab wound to the axilla, after radical mastectomy, or in some viral illnesses) paralyzes serratus anterior. The medial border of the scapula can no longer be held flat against the posterior thorax and lifts away like a bird's wing - especially visible when the patient pushes against a wall. Classic exam finding.
PART 3: Scalene Muscles
Three muscles on each side of the neck: anterior, middle, and posterior scalene.
- Origin: Transverse processes of cervical vertebrae (C2-C7)
- Insertion: First and second ribs
- Primary action: Lateral flexion and rotation of the cervical spine
- Respiratory role: Elevate ribs 1 and 2 during forced inspiration (accessory)
- The brachial plexus and subclavian artery pass between the anterior and middle scalenes (the scalene triangle) - relevant in thoracic outlet syndrome
PART 4: The Diaphragm - In Full Detail
The diaphragm is the most important respiratory muscle - a dome-shaped musculotendinous sheet separating the thoracic and abdominal cavities. It is responsible for approximately 75% of the tidal volume during quiet breathing.
Structure
The diaphragm has a muscular periphery and a central fibrous tendon (central tendon) shaped like a trilobed clover.
Muscular parts by origin:
| Part | Origin |
|---|---|
| Sternal part | Posterior surface of xiphoid process |
| Costal part | Inner surfaces of lower 6 costal cartilages (ribs 7-12) and lower 6 ribs |
| Lumbar part | Via two crura (right and left) from the vertebral bodies (right: L1-L3; left: L1-L2) and via arcuate ligaments |
Arcuate ligaments (the three "arches"):
- Median arcuate ligament (Lig. arcuatum medianum): A fibrous arch connecting the two crura over the aorta at the midline - forms the roof of the aortic hiatus
- Medial arcuate ligament (Lig. arcuatum medialis): An arch of fascia over the psoas major muscle, connecting the body of L1/L2 to the transverse process of L1
- Lateral arcuate ligament (Lig. arcuatum lateralis): An arch of fascia over the quadratus lumborum muscle, from the transverse process of L1 to the 12th rib
Insertion: All muscular fibers converge into the central tendon.
Innervation: Phrenic nerve (C3, C4, C5 - "C3,4,5 keep the diaphragm alive"). Sensory innervation to the periphery also has contributions from intercostal nerves T6-T11.
The Three Major Openings
| Opening | Vertebral Level | What passes through | Trick |
|---|---|---|---|
| Aortic hiatus | T12 | Aorta, thoracic duct, sometimes azygos vein | The aorta is BEHIND/posterior to the diaphragm (technically between the crura), so it is NOT constricted during diaphragm contraction |
| Esophageal hiatus | T10 | Esophagus, left and right vagus nerves (anterior and posterior vagal trunks) | In the muscular part of the diaphragm - contracts around esophagus; site of hiatal hernias |
| Caval opening (foramen venae cavae) | T8 | Inferior vena cava, right phrenic nerve | In the central tendon - the IVC is pulled open (wider) as the diaphragm contracts, facilitating venous return |
Mnemonic: "I 8 (ate) 10 eggs AT 12" - IVC at T8, Esophagus at T10, Aorta at T12. Or count the letters: "IVC" = 3 letters → T8 ÷ ... just use the mnemonic!
Diaphragm and Respiration
During inspiration:
- Phrenic nerve fires → diaphragm contracts
- The dome descends (flattens) ~1.5 cm in quiet breathing, up to 10 cm in forced breathing
- The volume of the thoracic cavity increases both inferiorly (vertical) and laterally (bucket-handle movement of ribs)
- Intrapleural pressure drops → lungs expand → air flows in (Boyle's Law)
During quiet expiration:
- Passive: Diaphragm simply relaxes; elastic recoil of lungs and chest wall drives air out
- No muscular effort needed
During forced expiration:
- Abdominal muscles (especially transversus abdominis and internal oblique) contract → push abdominal viscera upward against the diaphragm → accelerates exhalation
Congenital Diaphragmatic Hernia (CDH)
During embryological development, the diaphragm forms from four elements: the septum transversum, the pleuroperitoneal membranes, the dorsal mesentery of the esophagus, and body wall mesoderm. Failure of fusion creates a defect.
Bochdalek hernia (most common, ~85% of CDH):
- Posterolateral defect, left side in 85% of cases (because the right side closes earlier)
- Abdominal contents (small bowel, stomach, spleen, liver) herniate into the thorax
- Compresses the developing lungs → bilateral pulmonary hypoplasia (even the contralateral lung is hypoplastic)
- Presents at birth with: respiratory distress, cyanosis, scaphoid (flat/sunken) abdomen, bowel sounds in the thorax, shifted trachea/mediastinum
- Management: Surgical emergency - mechanical ventilation first to stabilize, then surgical repair
Morgagni hernia (rare, ~2%):
- Anterior (parasternal) defect - through the gap between the sternal and costal portions
- Usually contains omentum or colon
- Often asymptomatic, found incidentally
PART 5: Respiratory Muscles - Complete Overview
Primary Muscles (active in every breath)
- Diaphragm - the workhorse
- External intercostals - elevate ribs (bucket-handle and pump-handle movements)
Accessory/Secondary Muscles (recruited during increased ventilatory demand - exercise, disease)
| Muscle | Primary Action as Accessory | Ribs Elevated |
|---|---|---|
| Scalenes (ant, mid, post) | Fix/elevate ribs 1-2 | 1-2 |
| Pectoralis minor | Elevates ribs 3-5 (when shoulder fixed) | 3-5 |
| Serratus anterior (ant + post) | Elevates ribs 6-8 | 6-8 |
| Latissimus dorsi | Elevates ribs 9-10 | 9-10 |
| Quadratus lumborum | Fixes and controls ribs 11-12 (prevents them being pulled inward) | 11-12 |
Muscles of Forced Expiration
- Rectus abdominis, internal oblique, external oblique, transversus abdominis - push the viscera up against the diaphragm
- Internal intercostals - depress ribs
📘 Module 2 - Topic 4: Muscles of the Abdomen (Detailed)
PART 1: Layers of the Anterior Abdominal Wall
Understanding the layers from outside to inside is foundational for any abdominal surgery or hernia diagnosis. From superficial to deep:
- Skin
- Subcutaneous connective tissue - two layers:
- Camper's fascia (superficial/fatty layer): a continuous fatty sheet that extends over the entire body as subcutaneous fat. Below the inguinal ligament it continues into the thigh.
- Scarpa's fascia (deep/membranous layer): a firm, membrane-like sheet. It fuses with the fascia lata of the thigh just below the inguinal ligament. Importantly, it continues as Colles' fascia in the perineum - meaning urine from a ruptured urethra can track upward into the anterior abdominal wall under Scarpa's fascia.
- External oblique muscle
- Internal oblique muscle
- Transversus abdominis muscle
- Transversalis fascia (deep investing fascia of the abdominal wall) - fuses with the fascia lata inferiorly
- Preperitoneal (extraperitoneal) fat
- Parietal peritoneum
Innervation of the anterior abdominal wall:
- Skin and muscles: anterior rami of T7-T12 (intercostal and subcostal nerves) sweep around the costal margin into the abdominal wall
- T6 supplies skin over the xiphoid
- T10 dermatome = the umbilicus (a key clinical landmark)
- L1 (via ilioinguinal and iliohypogastric nerves) supplies the inguinal and suprapubic region
PART 2: Congenital Anterior Wall Defects
Gastroschisis
- Paraumbilical herniation of abdominal contents (usually intestine) through a full-thickness defect in the abdominal wall, almost always on the right side of the umbilicus
- The intestines are not covered by a sac (herniated organs are exposed directly to amniotic fluid → thickened, matted, foreshortened bowel)
- Usually an isolated anomaly (not associated with chromosomal defects)
- Associated with young maternal age, gastroschisis is not related to umbilical cord abnormalities
- Treatment: Immediate surgical repair or staged reduction using a silastic silo
Omphalocele (Exomphalos)
- Herniation of abdominal organs through the umbilicus (midline)
- Contents (can include liver, bowel, spleen) are covered by a translucent sac composed of amnion and peritoneum
- Strongly associated with chromosomal anomalies (trisomy 13, 18, 21) and other syndromes (Beckwith-Wiedemann)
- Larger and more clinically complex than gastroschisis
| Feature | Gastroschisis | Omphalocele |
|---|---|---|
| Location | Paraumbilical (right) | Umbilicus (midline) |
| Sac | Absent - bowel exposed | Present - covered |
| Bowel appearance | Matted/thickened (amniotic fluid damage) | Normal |
| Associations | Usually isolated | Chromosomal/syndromic |
| Maternal risk factor | Young maternal age | Advanced maternal age |
PART 3: The Four Anterior Abdominal Muscles - In Full Detail
1. Rectus Abdominis
The vertical midline muscle that makes the "6-pack."
- Origin: Pubic crest, pubic tubercle, pubic symphysis
- Insertion: Cartilage of 5th, 6th, 7th ribs; xiphoid process
- Action:
- Flexes the trunk (lumbar flexion)
- Compresses the abdomen
- Increases intra-abdominal pressure (coughing, sneezing, Valsalva maneuver, forced expiration, defecation, childbirth)
- Unique feature: Interrupted by 3-4 tendinous intersections (horizontal fibrous bands adherent to the anterior layer of the rectus sheath) - these create the visible "abs" segments
- Innervation: Anterior rami T7-T12
- Enclosed within the rectus sheath (see below)
2. Pyramidalis
A small, often-absent triangular muscle anterior to the lower rectus abdominis.
- Origin: Anterior surface of the pubis
- Insertion: Linea alba
- Action: Tenses the linea alba
- Present in only ~80% of people; absent in ~20%
- Clinical relevance: minimal, but surgeons note its presence during midline incisions
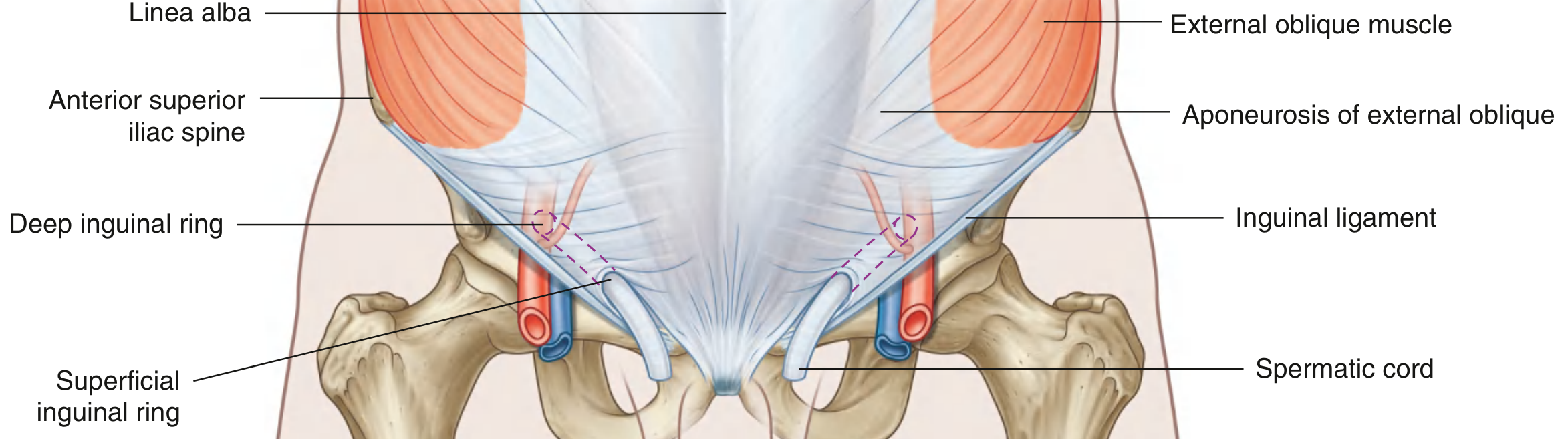
3. External Oblique
The largest and most superficial of the three flat lateral abdominal muscles.
- Origin: Outer surfaces and inferior borders of ribs 5-12 (lower 8 ribs)
- Fiber direction: Obliquely anteroinferiorly - same direction as the external intercostals - like "hands in front pockets" (fibers run downward and toward the midline)
- Insertion:
- Lateral fibers → outer lip of the iliac crest
- Medial/anterior fibers → become a broad flat aponeurosis that contributes to the anterior layer of the rectus sheath and inserts into the linea alba
- The lower free border of this aponeurosis folds inward on itself to form the inguinal ligament (from ASIS to pubic tubercle)
- Actions:
- Ipsilateral lateral flexion of trunk
- Contralateral rotation of trunk (e.g., right external oblique turns you to the LEFT)
- Compresses abdomen; increases intra-abdominal pressure
- Innervation: Anterior rami T5-T12, L1
4. Internal Oblique
The middle flat lateral muscle.
- Origin: Lateral two-thirds of the inguinal ligament; iliac crest; thoracolumbar fascia
- Fiber direction: Obliquely superiorly and medially - perpendicular to external oblique fibers (fan-shaped, running "upward toward the midline")
- Insertion:
- Uppermost fibers → lower 3-4 costal cartilages (ribs 9-12)
- Middle and lower fibers → form the internal oblique aponeurosis, split to wrap around rectus abdominis as part of both layers of the rectus sheath, and insert into the linea alba
- Medial-most fibers → fuse with the lowest fibers of transversus abdominis to form the conjoint tendon (inguinal falx), inserting into the pubic crest and pectineal line
- Actions:
- Ipsilateral lateral flexion of trunk
- Ipsilateral rotation of trunk (opposite to external oblique for rotation - right internal oblique turns you to the RIGHT)
- Compresses abdomen
- Innervation: Anterior rami T7-T12, L1
- Also gives rise to the cremaster muscle (from its lower fibers), which covers the spermatic cord and testis
5. Transversus Abdominis
The deepest of the three flat lateral muscles. Fibers run horizontally.
- Origin: Lateral one-third of the inguinal ligament; inner lip of the iliac crest; thoracolumbar fascia; inner surfaces of lower 6 costal cartilages (ribs 7-12)
- Fiber direction: Horizontal/transverse (hence the name)
- Insertion:
- Upper fibers → form the transversus abdominis aponeurosis → contributes to the rectus sheath → inserts into the linea alba
- Lowermost fibers → fuse with the aponeurosis of the internal oblique to form the conjoint tendon
- Actions:
- Compresses and supports the abdominal contents (the main "corset" muscle)
- Increases intra-abdominal pressure
- No rotational or lateral flexion action (horizontal fibers cannot rotate or flex)
- Innervation: Anterior rami T7-T12, L1
Summary: Rotation Trick
| Muscle | Lateral flexion | Rotation |
|---|---|---|
| External oblique (right) | Right side | Rotates trunk to LEFT |
| Internal oblique (right) | Right side | Rotates trunk to RIGHT |
| So: bilateral external + internal oblique = pure flexion; unilateral = lateral flexion + rotation |
PART 4: The Rectus Sheath - Detailed
The rectus sheath is a fibrous envelope enclosing the rectus abdominis and pyramidalis, formed by the splitting and reuniting of the aponeuroses of all three lateral muscles.
The key structure to understand: the Arcuate Line (of Douglas)
- Located about halfway between the umbilicus and pubic symphysis (roughly at the level of the ASIS)
- Marks where the arrangement of aponeuroses changes
Above the Arcuate Line (upper 2/3):
- Anterior layer: External oblique aponeurosis + anterior lamina of internal oblique aponeurosis
- Posterior layer: Transversus abdominis aponeurosis + posterior lamina of internal oblique aponeurosis (the internal oblique splits and wraps around both sides)
Below the Arcuate Line (lower 1/3):
- At the arcuate line, the transversus abdominis aponeurosis AND the posterior lamina of the internal oblique aponeurosis swing anteriorly to join the anterior layer
- Anterior layer: ALL THREE aponeuroses (external oblique + internal oblique + transversus abdominis)
- Posterior layer: ABSENT
- The posterior surface of the lower rectus abdominis rests directly on the transversalis fascia (and therefore the peritoneum is very close)
Clinical importance of the arcuate line:
- The posterior sheath ends abruptly at the arcuate line - seen as a distinct edge during surgery
- Below the arcuate line, the inferior epigastric vessels (which normally run in the posterior sheath) are now anterior to the peritoneum
- Hematomas of the rectus sheath track differently above vs. below the arcuate line
Key midline structures formed by the rectus sheath:
- Linea alba: The midline fusion of all three aponeuroses from both sides, extending from the xiphoid to the pubic symphysis. This is the bloodless midline incision site in abdominal surgery.
- Linea semilunaris: The lateral edge of the rectus sheath (visible as a curved groove in muscular individuals)
- Tendinous intersections: Horizontal bands within the rectus abdominis creating the "6-pack" appearance
PART 5: Hernias of the Abdominal Wall
Midline Hernias
| Hernia | Location | Details |
|---|---|---|
| Umbilical | Umbilicus (T10 level) | Midline, through the umbilical ring. Common in infants (usually closes by age 2). In adults, often acquired (obesity, ascites, multiparity) |
| Epigastric | Linea alba, xiphoid → umbilicus | Through a weakness in the linea alba between the xiphoid and umbilicus. Often contains preperitoneal fat rather than bowel |
| Incisional | At a previous surgical scar | Post-op complication due to wound dehiscence or impaired healing |
| Spigelian | Along the linea semilunaris near the arcuate line | Below the umbilicus, lateral to rectus abdominis. Rare but can be subtle/occult (herniates between muscle layers) |
Lumbar Hernias (Posterior)
Both occur through naturally weak triangles in the posterior abdominal wall:
Superior (Grynfeltt) Lumbar Triangle:
- Bounded by: 12th rib (superiorly), erector spinae muscle (medially), internal oblique muscle (laterally)
- Protrusion through here = Grynfeltt hernia
Inferior (Petit) Lumbar Triangle:
- Bounded by: Iliac crest (inferiorly), latissimus dorsi (medially), external oblique (laterally)
- Protrusion through here = Petit hernia
PART 6: The Inguinal Region - Full Detail
The Inguinal Ligament
- A fibrous band, approximately 12-15 cm long
- Runs from the anterior superior iliac spine (ASIS) laterally to the pubic tubercle medially
- Formation: The free lower border of the external oblique aponeurosis folds posteriorly and inferiorly on itself → creating a trough/gutter (the "shelving edge")
- The internal oblique and transversus abdominis muscles originate from its lateral two-thirds
- Medially, it has a specialized extension: the lacunar ligament (Gimbernat's ligament) - a triangular expansion of fibers that fans out to attach to the pectineal line. The medial edge of the lacunar ligament forms the sharp medial wall of the femoral ring.
Development of the Inguinal Canal
The inguinal canal is not simply a "hole" - it is a tunnel created during testicular descent. Here is what happens embryologically:
- The gonads form on the posterior abdominal wall (near the kidneys)
- A fibromuscular cord, the gubernaculum, forms and connects the testis to the developing scrotum
- A peritoneal diverticulum called the processus vaginalis pushes through the anterior abdominal wall layers along the gubernaculum's path, dragging the muscular and fascial layers with it
- The testis descends along this path into the scrotum (usually by 7-8 months gestation)
- The processus vaginalis normally closes after birth; if it doesn't → congenital indirect inguinal hernia or hydrocele
This is why the inguinal canal exists and why it is the most common site of herniation in males.
Inguinal Canal - Anatomy
A slit-like passage ~4 cm long that runs downward and medially, just above and parallel to the lower half of the inguinal ligament.
Contents:
- Male: Spermatic cord + ilioinguinal nerve + genital branch of genitofemoral nerve
- Female: Round ligament of uterus + ilioinguinal nerve + genital branch of genitofemoral nerve
Four walls in detail (from Gray's Anatomy for Students):
| Wall | Structure | Key Details |
|---|---|---|
| Anterior | External oblique aponeurosis (entire length) + internal oblique muscle (laterally only, reinforcing over the deep ring) | The lateral reinforcement by internal oblique protects the deep ring |
| Posterior | Transversalis fascia (entire length) + conjoint tendon (medially, reinforcing over the superficial ring) | Conjoint tendon reinforces the medial weak spot |
| Roof (superior) | Arching fibers of internal oblique + transversus abdominis | They arch from the inguinal ligament laterally → conjoint tendon medially, like a "shutter" |
| Floor (inferior) | Inguinal ligament (medial half) + lacunar ligament (medial corner) | Forms a gutter on which the spermatic cord rests |
The "shutter mechanism": When intra-abdominal pressure rises suddenly (coughing, straining), the internal oblique and transversus abdominis contract, pulling the roof downward like a shutter onto the floor. This actively closes the canal and prevents herniation. If this mechanism fails → hernia.
The Two Inguinal Rings
Deep (Internal) Inguinal Ring:
- The entrance to the canal
- Located midway between the ASIS and pubic symphysis, just above the inguinal ligament
- Formed by an outpouching of the transversalis fascia (it is NOT actually a defect - it is the beginning of the fascial sleeve around the spermatic cord = internal spermatic fascia)
- Lies lateral to the inferior epigastric vessels
- The inferior epigastric vessels are the key landmark separating direct from indirect hernias
Superficial (External) Inguinal Ring:
- The exit from the canal
- A triangular opening in the external oblique aponeurosis, superior to the pubic tubercle
- The apex points superolaterally; the base is formed by the pubic crest
- Two crura (medial and lateral) define the sides; held together at the apex by intercrural fibers (preventing the ring from widening)
- The external oblique continues as the external spermatic fascia over the spermatic cord
PART 7: Hesselbach's Triangle and Inguinal Hernias
Hesselbach's (Inguinal) Triangle
The anatomical "weak zone" of the posterior inguinal wall where direct inguinal hernias bulge through.
Three borders:
- Medially: Lateral edge of the rectus abdominis muscle
- Laterally: Inferior epigastric vessels (key landmark)
- Inferiorly: Inguinal ligament
The floor of the triangle is the transversalis fascia + conjoint tendon (which reinforces the medial portion). Direct hernias push through a weakness in this floor.
Inguinal Hernias - Direct vs. Indirect
| Feature | Direct Inguinal Hernia | Indirect Inguinal Hernia |
|---|---|---|
| Path | Pushes directly through the posterior wall of the inguinal canal (through Hesselbach's triangle) | Enters the deep inguinal ring, traverses the full canal, exits the superficial ring (can descend into the scrotum) |
| Relation to inferior epigastric vessels | Medial to the vessels | Lateral to the vessels |
| Coverings | Only covered by transversalis fascia + external spermatic fascia | Covered by all 3 fascial layers: internal spermatic fascia + cremasteric fascia + external spermatic fascia |
| Cause | Acquired weakness in the abdominal wall (aging, obesity, chronic straining) | Congenital (failed closure of processus vaginalis) or acquired |
| Demographics | Older males | Most common overall; males >>> females; all ages |
| Risk of strangulation | Lower (wide neck) | Higher (tight ring can compress blood supply) |
| Finger test | Hernia pushes against the tip of finger inserted at the superficial ring | Hernia comes down the side of the finger (along the canal) |
Mnemonic: "DIrect" = goes DIrect through the abdominal wall, is Medial (think M before N). "INdirect" = goes IN the deep ring, is lateral (lateral comes before medial alphabetically... or remember: indirect has more letters than direct, it takes a longer path).
PART 8: Umbilical Folds and Fossae
Viewed from the inside of the anterior abdominal wall (i.e., looking at the peritoneum), you see 5 ridges (folds) converging toward the umbilicus from below:
The 5 Umbilical Folds (Peritoneal Folds)
| Fold | Number | Deep Structure | Embryological Origin |
|---|---|---|---|
| Median umbilical fold | 1 (midline) | Median umbilical ligament = obliterated urachus | The urachus connected the fetal bladder to the allantois (passes from bladder apex to umbilicus). Its obliteration leaves this ligament. |
| Medial umbilical folds | 2 (one each side of median) | Medial umbilical ligaments = obliterated umbilical arteries | In fetal circulation, the umbilical arteries carried deoxygenated blood from the internal iliac arteries to the placenta. They obliterate at birth. |
| Lateral umbilical folds | 2 (outermost) | Inferior epigastric artery and vein | These are active, functional blood vessels (not obliterated) that run upward to supply the anterior abdominal wall |
Clinical note on the urachus: If the urachus fails to fully obliterate, you get:
- Patent urachus = urine drains from the umbilicus
- Urachal cyst = a fluid-filled cyst along the ligament
- Urachal sinus = opens only at the umbilicus
The Fossae (Depressions Between the Folds)
Between the folds, the peritoneum dips inward creating 3 pairs of shallow depressions (fossae) on each side:
| Fossa | Location | Clinical Significance |
|---|---|---|
| Supravesical fossa | Between median and medial umbilical folds | Size varies with bladder filling (rises as bladder fills). Site of supravesical hernia |
| Medial inguinal fossa (Hesselbach's triangle) | Between the medial and lateral umbilical folds (medial to the inferior epigastric vessels) | Site of DIRECT inguinal hernia |
| Lateral inguinal fossa | Lateral to the lateral umbilical fold (lateral to the inferior epigastric vessels) | Site of INDIRECT inguinal hernia |
This beautifully explains the surgical anatomy: you can look through a laparoscope at the fossae and immediately identify which type of hernia bulge you're dealing with.
PART 9: Posterior Abdominal Muscles
Psoas Major
- Origin: Vertebral bodies and intervertebral discs of T12-L4 + transverse processes of lumbar vertebrae
- Insertion: Lesser trochanter of the femur (joins iliacus = iliopsoas)
- Action: Flexes the thigh at the hip (bringing the knee toward the chest); also flexes the lumbar spine laterally when acting unilaterally
- Innervation: Anterior rami L1-L3 directly
- Clinical: A psoas abscess (e.g., from vertebral TB/Pott's disease or Crohn's disease) tracks along the psoas sheath and can present as a groin lump or cause a painful, fixed-flexion deformity of the hip. The "psoas sign" (pain on passive hip extension) suggests peritoneal irritation (e.g., appendicitis) near the psoas.
Iliacus
- Origin: Iliac fossa (inner surface of the ilium)
- Insertion: Lesser trochanter (with psoas = iliopsoas)
- Action: Flexes the thigh
- Innervation: Femoral nerve (L2, L3)
Iliopsoas
The combined psoas major + iliacus is called the iliopsoas - the most powerful hip flexor. It is the primary muscle you use to walk upstairs, kick, or do a sit-up with straight legs.
Psoas Minor
- Present in only ~50% of people
- Origin: T12-L1 vertebrae
- Insertion: Pecten pubis and iliopubic ramus (iliopectineal eminence)
- Action: Weak flexion of the lumbar spine; assists in tilting the pelvis
- Clinically insignificant
Quadratus Lumborum
- A thick, roughly quadrilateral muscle of the posterior abdominal wall
- Origin: Iliac crest and iliolumbar ligament
- Insertion: 12th rib; transverse processes of L1-L4
- Action:
- Lateral flexion of the trunk (unilateral)
- Fixes the 12th rib during inspiration (prevents it from being pulled upward by the diaphragm's contraction - stabilizing the diaphragm's origin)
- Assists in expiration by pulling the 12th rib inferiorly
- Innervation: T12, L1-L4
- Clinical: A common source of low back pain - often called "the joker of low back pain" because it can mimic many conditions. Trigger points in QL refer pain to the sacroiliac joint and hip.
Quick-Reference Clinical Summary
| Condition | Key Anatomy | Mechanism |
|---|---|---|
| Winged scapula | Serratus anterior (long thoracic nerve) | Scapula not held against thorax |
| Poland syndrome | Absent pectoralis ± brachydactyly | Congenital hypoplasia |
| CDH (Bochdalek) | Left posterolateral diaphragm | Pulmonary hypoplasia |
| Thoracentesis risk | Neurovascular bundle (VAN) in costal groove | Insert above rib lower border |
| Gastroschisis | Right of umbilicus, no sac | Paraumbilical wall defect |
| Omphalocele | At umbilicus, has sac | Midline failure + syndromes |
| Arcuate line | Lower 1/3 rectus - no posterior sheath | Rectus hematoma tracking |
| Spigelian hernia | Along linea semilunaris at arcuate line | Between muscle layers |
| Direct inguinal hernia | Through Hesselbach's triangle, medial to IEV | Acquired wall weakness |
| Indirect inguinal hernia | Through deep ring, lateral to IEV | Patent processus vaginalis |
| Patent urachus | Median umbilical ligament | Failed urachus obliteration |
| Psoas abscess | Psoas sheath | TB / Crohn's tracks into groin |
Sources: Gray's Anatomy for Students (9780323934237); General Anatomy and Musculoskeletal System - THIEME Atlas; Medical Physiology (9780323319737); Sabiston Textbook of Surgery (9780443124341)
This is a shared conversation. Sign in to Orris to start your own chat.