Short note on osteomeatal complex
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Here is a comprehensive short note on the osteomeatal complex, drawn from authoritative ENT textbooks:
Osteomeatal Complex (OMC)
Definition and Location
The osteomeatal complex (OMC) is a functional anatomical region situated within the middle meatus of the lateral nasal wall. It represents the final common drainage pathway for the majority of the paranasal sinuses - specifically the frontal sinus, anterior/middle ethmoid cells, and maxillary sinus. The sphenoid sinus and posterior ethmoid cells drain separately into the sphenoethmoidal recess.
KJ Lee's Essential Otolaryngology defines its boundaries as:
- Posterior: Basal lamella of the middle turbinate
- Medial: Middle turbinate
- Lateral: Lamina papyracea
- Superior: Fovea ethmoidalis (roof of ethmoid)
Five Key Structures
According to Scott-Brown's Otorhinolaryngology, the OMC comprises five anatomical components:
- Maxillary ostium - the main drainage channel of the maxillary sinus opening into the middle meatus
- Infundibulum - the air channel between the uncinate process and the inferomedial border of the orbit; drains maxillary and ethmoid sinus ostia into the hiatus semilunaris (the second "tight spot" of sinus drainage)
- Bulla ethmoidalis - the largest anterior ethmoid air cell, which projects inferomedially over the hiatus semilunaris; its posterior wall, when intact, creates a space called the sinus lateralis (retrobullar recess) between itself and the basal lamella
- Uncinate process - a crescent-shaped bony projection forming the anterior border of the hiatus semilunaris; its free edge delimits the inferior margin of the infundibulum; superiorly it fuses with the agger nasi cell and nasolacrimal duct
- Hiatus semilunaris - the final drainage passage, a two-dimensional crescentic gap between the free edge of the uncinate process (anteroinferiorly) and the bulla ethmoidalis (posterosuperiorly); medially it opens into the middle meatus
Anterior vs. Posterior Ostiomeatal Units
Cummings Otolaryngology describes two main ostiomeatal channels:
- Anterior ostiomeatal unit - frontal sinus ostium, frontal recess, maxillary sinus ostium, infundibulum, and middle meatus
- Posterior ostiomeatal unit - sphenoid sinus ostium, sphenoethmoidal recess, and superior meatus
Three "tight spots" are the focus of sinus imaging: (1) the frontal recess, (2) the infundibulum, and (3) the sphenoethmoidal recess.
Frontal Recess
The frontal sinus drainage pathway drains via an hourglass-shaped outflow tract. The frontal recess is the narrowest portion - the first tight spot. It is bordered:
- Anteriorly by the agger nasi cell
- Posteriorly by the ethmoid bulla
- Inferiorly by the uncinate process
The direction of uncinate attachment determines whether the frontal sinus drains medial or lateral to it.
Coronal CT Anatomy
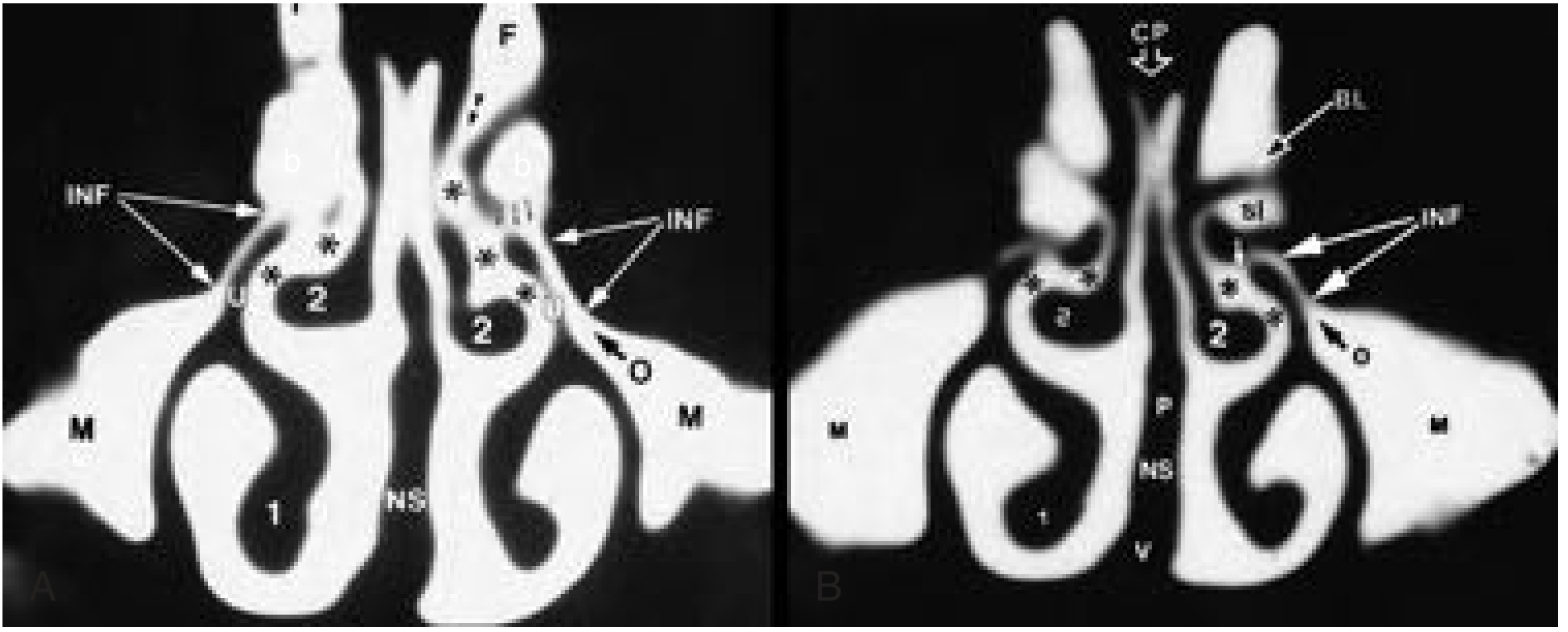
Coronal CT: Anterior ostiomeatal channels showing infundibulum (INF), uncinate (U), maxillary sinus (M), ethmoid bulla (b), middle meatus (), and hiatus semilunaris. - Cummings Otolaryngology, Fig. 38.5*
Clinical Significance
Pathophysiology of sinusitis: Obstruction of the OMC - whether from mucosal inflammation, anatomical variants, polyps, or trauma - is the key precipitating event in most cases of rhinosinusitis. Obstruction leads to:
- Retained secretions in the anterior sinuses
- Reduced sinus aeration and mucosal hypoxia
- Ciliary impairment and mucus stasis
- Secondary bacterial infection and chronic inflammation
This creates a self-perpetuating cycle: mucosal oedema further narrows the OMC, worsening drainage and aeration.
Diagnostic criteria for rhinosinusitis (EPOS guidelines) include CT changes showing mucosal changes within the OMC and/or sinuses, alongside nasal symptoms.
Nasal polyps most commonly originate in the upper nose around the OMC, and Lund-Mackay CT scoring assigns a separate score to OMC opacification.
Nasal septal deviation with a high-angle deviation or bony spur can contribute to mechanical obstruction of the anterior OMC.
Silent sinus syndrome (imploding maxillary sinus) originates from OMC obstruction causing hypoventilation of the maxillary sinus.
Surgical Relevance - FESS
Functional Endoscopic Sinus Surgery (FESS) is specifically designed around OMC anatomy. The surgical objectives include:
- Restoring patency of the OMC
- Uncinectomy (removal of uncinate process) to open the infundibulum
- Clearing obstructing anterior ethmoid cells
- Preserving normal mucosa to allow mucociliary function to recover
Topical decongestants markedly reduce inferior and middle turbinate size and improve OMC patency, but have no effect on [deeper sinus mucosa] - Scott-Brown's, Vol 1.
Summary Table
| Structure | Role |
|---|---|
| Uncinate process | Anterior wall of infundibulum; guides drainage direction |
| Hiatus semilunaris | 2D gap; final drainage passage into middle meatus |
| Infundibulum | 3D air channel; common pathway for maxillary + ethmoid drainage |
| Ethmoid bulla | Largest anterior ethmoid cell; posterior wall of hiatus semilunaris |
| Maxillary ostium | Natural opening of maxillary sinus |
| Frontal recess | Drainage conduit for frontal sinus; most complex and variable |
Sources: KJ Lee's Essential Otolaryngology; Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vols 1 & 2; Cummings Otolaryngology Head & Neck Surgery
This is a shared conversation. Sign in to Orris to start your own chat.