An an ophthalmologist i want to know about the conditions in which lens zonules are intact but lena is subluxated and those conditions in which lens zolules are broken and lens is subluxated or dislocated
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Loading Image
Loading Image
I now have all the information needed from Kanski's to give a thorough, well-organized answer. Let me compile it.
Ectopia Lentis: Zonule Status as the Key Differentiator
Ectopia lentis means displacement of the lens from its normal position in the patellar fossa. The two broad categories you're asking about - intact zonules vs. broken/disintegrated zonules - are clinically and etiologically distinct.
GROUP 1: Lens Subluxated WITH Intact Zonules
In these conditions the zonules are not broken but are structurally abnormal (weakened, elongated, or stretched), allowing partial displacement. Because the zonules are still functionally present, accommodation is often retained and the lens tilts toward the side of intact zonules.
1. Marfan Syndrome (FBN1 gene - AD)
- Direction: Superotemporal (most characteristic) - upward and outward
- Zonule status: Zonules are intact but elongated due to fibrillin-1 deficiency; accommodation is often retained
- Degree: 80% have bilateral ectopia lentis; subluxation is the rule; outright dislocation into AC or vitreous is rare
- Key point: The subluxated lens tends to deviate toward the meridian of intact/less-stretched zonules
2. Familial Ectopia Lentis (AD)
- Bilateral symmetrical superotemporal displacement
- May manifest congenitally or later in life
- Isolated ocular condition - no systemic features
- Zonules present but weak/elongated
3. Ectopia Lentis et Pupillae (AR, rare)
- Congenital bilateral: lens and pupil displaced in opposite directions (lens temporal, pupil nasal, or vice versa)
- Small pupils that dilate poorly
- May be associated with microspherophakia
- Zonules are present, zonular dehiscence is partial
4. Weill-Marchesani Syndrome (AR or AD, FBN1)
- Conceptually the converse of Marfan syndrome - short stature, brachydactyly, learning difficulties
- Direction: Inferior subluxation, late childhood/early adulthood
- Zonule status: Early - zonules present but abnormal, leading to subluxation; later can progress to dislocation
- Microspherophakia (small, spherical lens) is characteristic
- High risk of angle closure from pupillary block due to microspherophakia - the spherical lens blocks aqueous flow
5. Aniridia
- Occasionally associated with ectopia lentis (inferior subluxation)
- Partial zonule weakness accompanies the iris hypoplasia
6. Sulfite Oxidase Deficiency
- Ectopia lentis is universal
- Zonule status varies; can have intact but functionally deficient zonules
GROUP 2: Lens Subluxated or Dislocated WITH Broken/Disintegrated Zonules
In these conditions the zonular fibers themselves are structurally destroyed, leading to partial or complete support loss. Accommodation is usually lost.
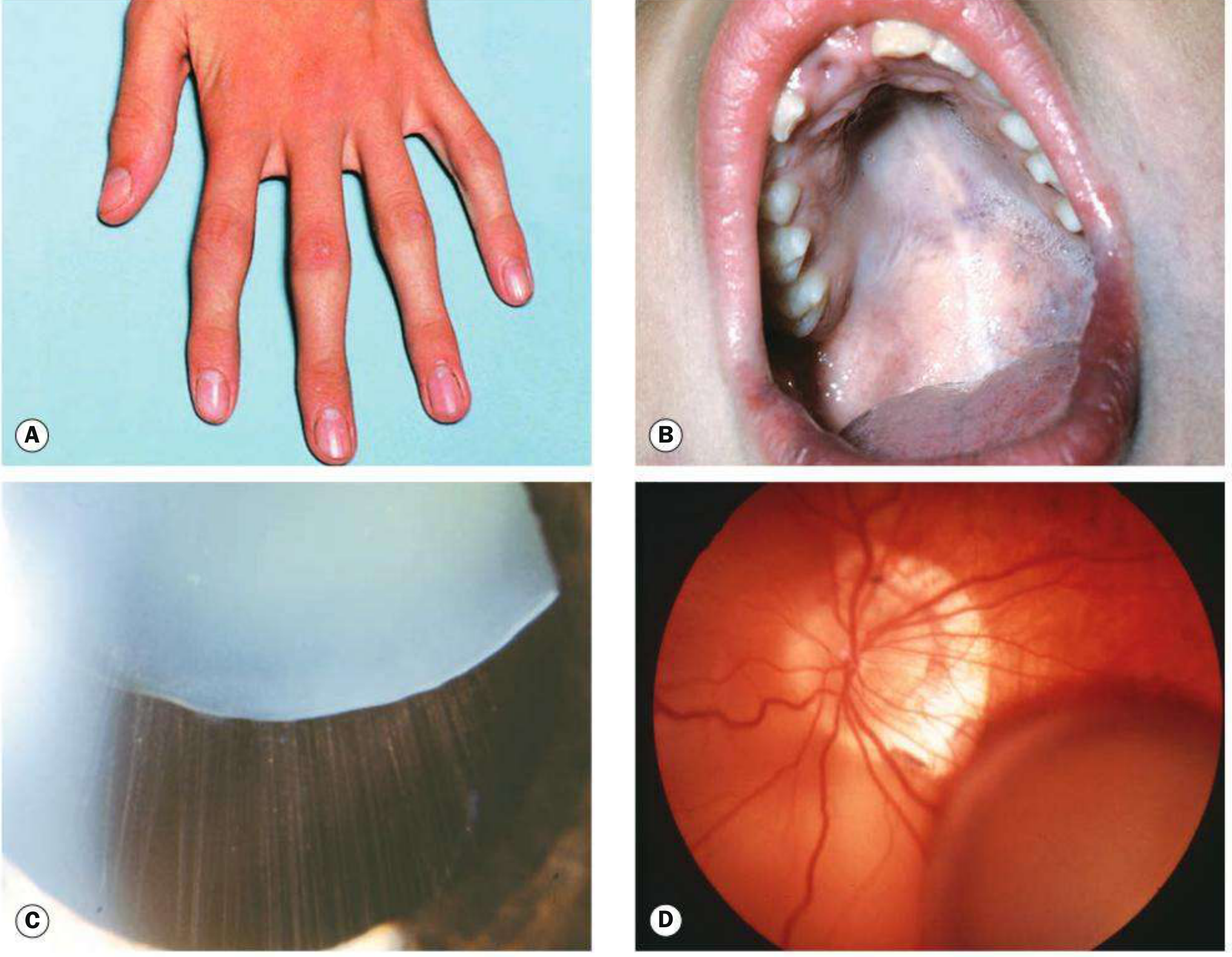
1. Homocystinuria (AR - cystathionine beta-synthase deficiency)
- Direction: Inferonasal - downward and inward (opposite of Marfan)
- Zonule status: Zonules disintegrate because they are rich in cysteine, which is deficient in homocystinuria. This is the most distinctive feature from Marfan
- Almost universal by age 25 in untreated cases
- Accommodation is lost
- Systemic: coarse blond hair, blue irises, Marfanoid habitus, neurodevelopmental delay, severe thrombotic predisposition (very important perioperatively - general anesthesia carries risk of thrombosis)
- Treatment: pyridoxine (B6), folic acid, vitamin B12 to reduce plasma homocysteine
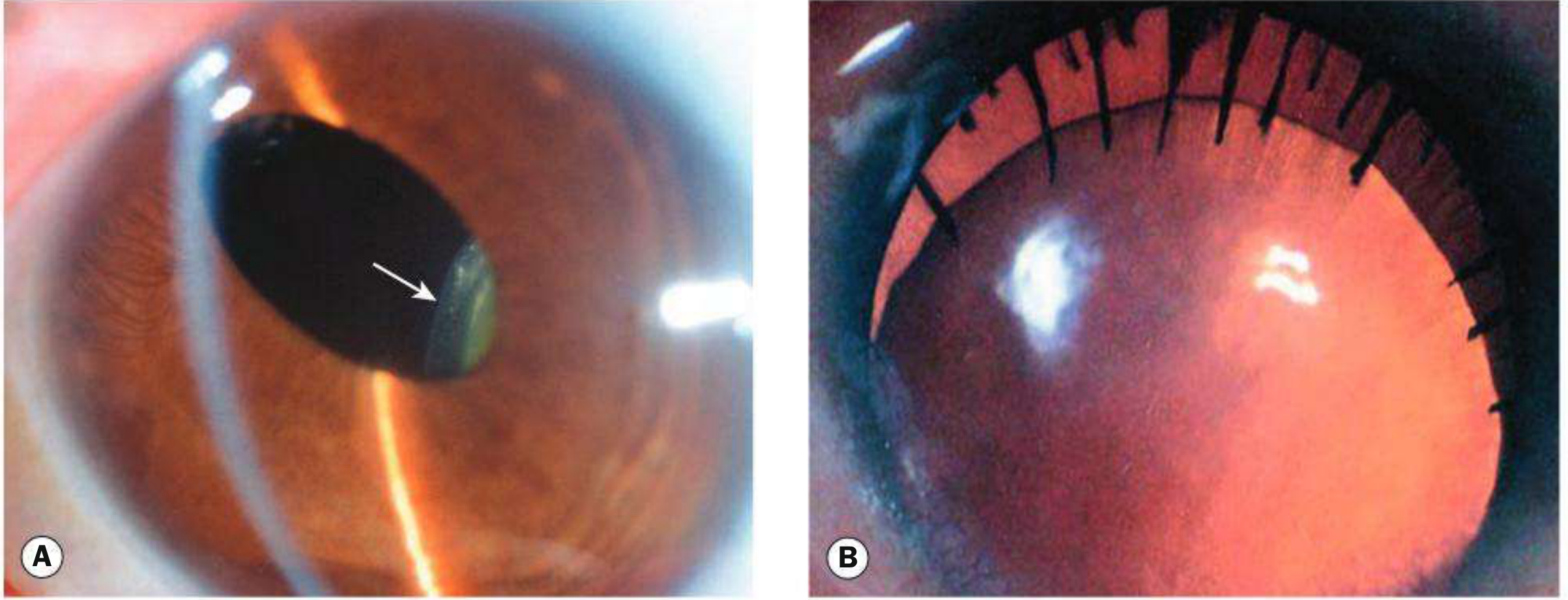
2. Trauma (Blunt)
- The most common acquired cause
- Blunt force tears the suspensory ligament focally (partial) or completely (360° rupture → complete dislocation)
- Partial zonule rupture → subluxation; the lens tilts toward the meridian of intact remaining zonules
- Complete 360° rupture → dislocation into vitreous (most common) or anterior chamber (less common)
- Signs: phakodonesis (lens tremor), iridodonesis (iris tremor), deepened AC over dehiscent area, lens edge visible under mydriasis, uniocular diplopia if pupil partly aphakic
- An underlying predisposing condition (e.g., pseudoexfoliation) should always be considered when zonular rupture occurs with seemingly minor trauma
3. Pseudoexfoliation Syndrome
- Most common cause of acquired zonule weakness worldwide
- Exfoliation material deposits on and weakens the zonules progressively
- Leads to subluxation; complete dislocation can occur spontaneously or with minimal trauma (e.g., during cataract surgery)
- The zonule fibers are structurally abnormal and fragile - not just stretched
- High surgical risk: capsule/zonule complex is weak even if frank subluxation is not yet present
4. Chronic Inflammation / Cyclitis
- Prolonged uveitis (chronic cyclitis, syphilis) causes zonule dissolution through inflammatory mediators
- Zonules are directly destroyed by the inflammatory process
- Lens may subluxate or dislocate
5. Hypermature Cataract
- Liquefaction of the lens cortex with reduction in lens volume and shrinkage causes progressive zonule relaxation and eventual rupture
- The bag-zonule complex loses tension and the lens can subluxate or dislocate
6. High Myopia / Buphthalmos (Large Axial Length)
- Mechanical stretching of the zonules due to globe enlargement
- Zonules become thin, elongated, and may break, permitting lens subluxation
- More common in high myopia (>6D) and congenital glaucoma with buphthalmos
Summary Comparison Table
| Condition | Zonule Status | Direction of Subluxation | Key Feature |
|---|---|---|---|
| Marfan syndrome | Intact (elongated) | Superotemporal | Accommodation retained; fibrillin-1 defect |
| Familial ectopia lentis | Intact (weak) | Superotemporal | No systemic disease |
| Ectopia lentis et pupillae | Intact (partial dehiscence) | Opposite to pupil | Miosis, poor dilation |
| Weill-Marchesani | Initially intact, may rupture later | Inferior | Microspherophakia, angle closure risk |
| Homocystinuria | Disintegrated | Inferonasal | No accommodation; thrombosis risk; cysteine-deficient zonules |
| Trauma | Torn/ruptured | Variable (away from tear) | History of blunt trauma; phakodonesis |
| Pseudoexfoliation | Structurally broken | Variable | Most common acquired cause; surgical risk |
| Chronic uveitis / syphilis | Dissolved | Variable | Inflammatory destruction |
| Hypermature cataract | Stretched then broken | Variable | Shrunken lens, advanced cataract |
| Buphthalmos / high myopia | Mechanically broken | Variable | Globe enlargement |
Clinical Pearls
- A subluxated lens always tilts toward the meridian of intact zonules - this helps localize the site of zonular weakness on examination
- Marfan vs. Homocystinuria: Both cause bilateral ectopia lentis, but Marfan goes up (intact zonules), homocystinuria goes down and in (zonules disintegrated). This is the classic exam distinction
- Phakodonesis/iridodonesis are signs of zonule instability - always look for these before cataract surgery
- Pseudoexfoliation can show phakodonesis without visible subluxation - always examine zonules carefully with retroillumination before surgery
- In homocystinuria, avoid general anesthesia if possible due to extreme thrombotic risk; if surgery is needed, anticoagulation and amino acid normalization are required preoperatively
Source: Kanski's Clinical Ophthalmology: A Systematic Approach, 10th Edition, pp. 354-357 (Ectopia Lentis chapter) and p. 931-932 (Traumatic Lens section)
This is a shared conversation. Sign in to Orris to start your own chat.