Hi can you help me in making notes I will send text help me in making images whatever text in in the image so it will better to learn and visualise
Neural Development and Regionalization The development of the central and peripheral nervous systems originates from specific embryonic structures. The neuroepithelia in the neural tube give rise to CNS neurons and CNS glial cells, including astrocytes, oligodendrocytes, and ependymal cells. The neural crest is responsible for the formation of PNS neurons, which are divided into alar and basal plates. • Alar plate (dorsal): Sensory function; induced by bone morphogenetic proteins (BMPs). It maintains the same orientation as the spinal cord. Basal plate (ventral): Motor function; induced by sonic hedgehog (SHH). Homeobox (HOX) genes play a crucial role in regulating neural tube segmentation and cranial-caudal differentiation. Mutations in these genes can lead to conditions such as syndactyly (affecting limbs) and hypospadias (affecting the urogenital system). Neural Tube and Vesicle Formation The neural tube undergoes regionalization to form different parts of the brain and spinal cord. The telencephalon is the first part, followed by the diencephalon. The remaining parts are arranged alphabetically: mesencephalon, metencephalon, and myelencephalon.
A clean, colorful medical study notes infographic on "Neural Development and Regionalization" with the following sections clearly laid out: TITLE at top: "Neural Development & Regionalization" in bold SECTION 1 - "Origins" box: - Neuroepithelia (Neural Tube) → CNS Neurons + CNS Glial Cells (Astrocytes, Oligodendrocytes, Ependymal cells) - Neural Crest → PNS Neurons SECTION 2 - Two side-by-side colored boxes for Alar vs Basal Plate: Left box (blue, dorsal): "ALAR PLATE" - Sensory Function - Induced by BMPs - Same orientation as spinal cord Right box (orange, ventral): "BASAL PLATE" - Motor Function - Induced by Sonic Hedgehog (SHH) SECTION 3 - "HOX Genes" box: - Regulate neural tube segmentation & cranial-caudal differentiation - Mutations → Syndactyly (limbs), Hypospadias (urogenital system) SECTION 4 - Neural Tube Vesicle Formation timeline/flowchart: Telencephalon → Diencephalon → Mesencephalon → Metencephalon → Myelencephalon With a note: "Telo & Diencephalon first, rest in alphabetical order" Use bright pastel background, color-coded sections, bold headings, arrows, and icons for easy memorization. Clean white background, medical textbook style.
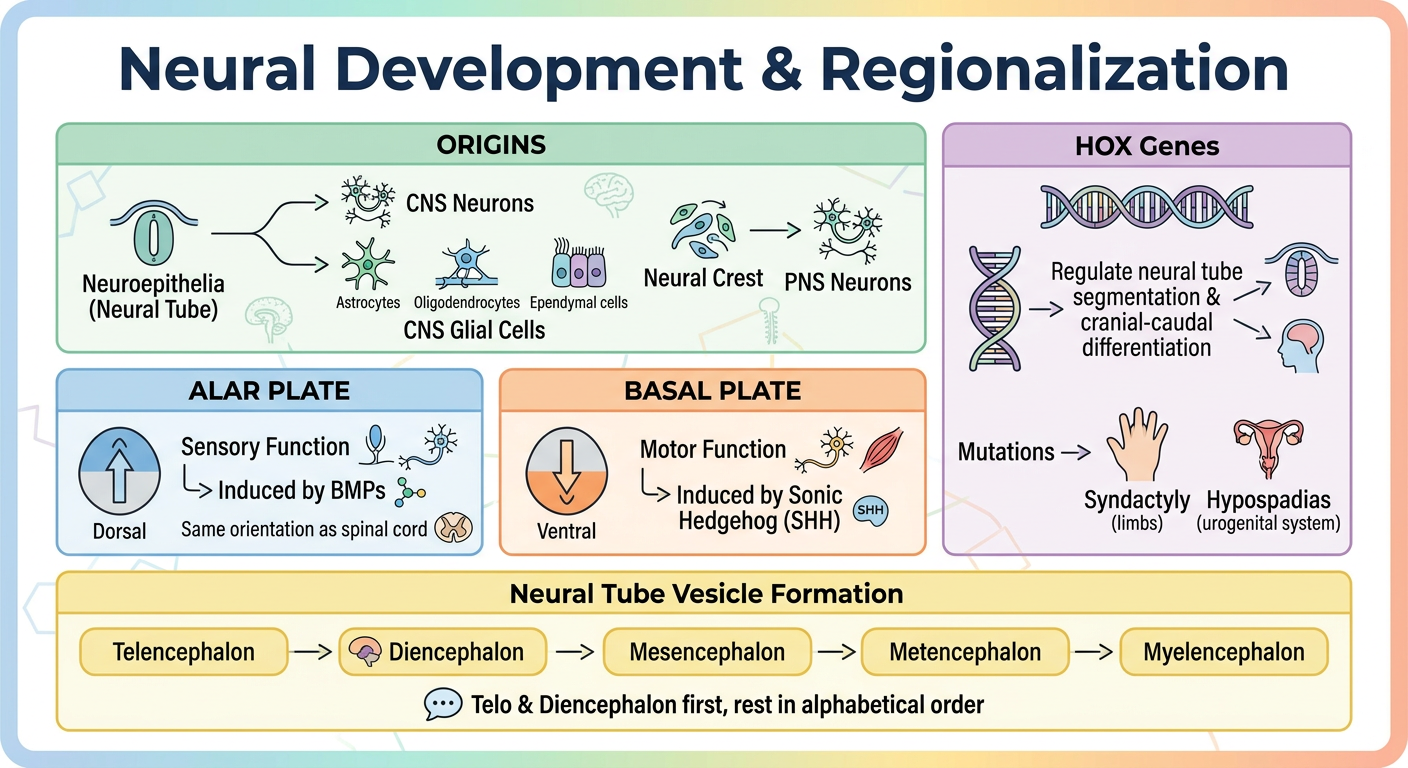
- Neuroepithelia → CNS | Neural Crest → PNS - two separate origins, easy to mix up
- Alar (dorsal) = Sensory - think "A for Above (dorsal) & Afferent (sensory)" - induced by BMPs
- Basal (ventral) = Motor - think "B for Below (ventral) & Basal ganglia (motor)" - induced by SHH
- HOX gene mutations → Syndactyly + Hypospadias (limbs & urogenital)
- Brain vesicles order: Telo → Dien → then alphabetical: Mes → Met → Myel
Create a comprehensive PDF study guide with all your notes
ls -la /tmp/workspace/ 2>/dev/null || mkdir -p /tmp/workspace && ls -la /tmp/workspace/
mkdir -p /tmp/workspace/neural-notes && python3 << 'EOF' from reportlab.lib.pagesizes import A4 from reportlab.lib import colors from reportlab.lib.styles import getSampleStyleSheet, ParagraphStyle from reportlab.lib.units import cm from reportlab.platypus import SimpleDocTemplate, Paragraph, Spacer, Table, TableStyle, HRFlowable from reportlab.platypus import KeepTogether from reportlab.lib.enums import TA_CENTER, TA_LEFT, TA_JUSTIFY from reportlab.lib.colors import HexColor import urllib.request from reportlab.platypus import Image import io # Download the generated image img_url = "https://cdn.orris.care/image-gen/8186ddbb784f4d8a995b16c20347a0a5.png" img_path = "/tmp/workspace/neural-notes/neural_visual.png" urllib.request.urlretrieve(img_url, img_path) print("Image downloaded:", img_path) EOF
python3 << 'EOF' from reportlab.lib.pagesizes import A4 from reportlab.lib import colors from reportlab.lib.styles import getSampleStyleSheet, ParagraphStyle from reportlab.lib.units import cm, mm from reportlab.platypus import SimpleDocTemplate, Paragraph, Spacer, Table, TableStyle, HRFlowable, Image, KeepTogether from reportlab.lib.enums import TA_CENTER, TA_LEFT, TA_JUSTIFY from reportlab.lib.colors import HexColor # Color palette DARK_BG = HexColor("#1a1a2e") ACCENT_BLUE = HexColor("#4a90e2") ACCENT_GREEN = HexColor("#27ae60") ACCENT_ORG = HexColor("#e67e22") ACCENT_PUR = HexColor("#8e44ad") ACCENT_RED = HexColor("#e74c3c") LIGHT_BLUE = HexColor("#ebf5fb") LIGHT_GREEN = HexColor("#eafaf1") LIGHT_ORG = HexColor("#fef9e7") LIGHT_PUR = HexColor("#f5eef8") LIGHT_RED = HexColor("#fdedec") WHITE = colors.white DARK_TEXT = HexColor("#2c3e50") MID_GRAY = HexColor("#7f8c8d") doc = SimpleDocTemplate( "/tmp/workspace/neural-notes/Neural_Development_Study_Guide.pdf", pagesize=A4, rightMargin=1.8*cm, leftMargin=1.8*cm, topMargin=2*cm, bottomMargin=2*cm ) W, H = A4 content_w = W - 3.6*cm styles = getSampleStyleSheet() # Custom styles def S(name, **kw): return ParagraphStyle(name, **kw) title_style = S("Title", fontSize=24, leading=30, textColor=WHITE, fontName="Helvetica-Bold", alignment=TA_CENTER, spaceAfter=4) subtitle_style = S("Subtitle", fontSize=11, leading=16, textColor=HexColor("#bdc3c7"), fontName="Helvetica", alignment=TA_CENTER, spaceAfter=0) section_head = S("SectionHead", fontSize=14, leading=18, textColor=WHITE, fontName="Helvetica-Bold", alignment=TA_LEFT, spaceBefore=6, spaceAfter=4) body = S("Body", fontSize=10.5, leading=16, textColor=DARK_TEXT, fontName="Helvetica", alignment=TA_JUSTIFY, spaceAfter=6) bullet_style = S("Bullet", fontSize=10.5, leading=16, textColor=DARK_TEXT, fontName="Helvetica", leftIndent=14, bulletIndent=0, spaceAfter=4) key_style = S("Key", fontSize=10, leading=14, textColor=DARK_TEXT, fontName="Helvetica-Bold") sub_key = S("SubKey", fontSize=9.5, leading=14, textColor=MID_GRAY, fontName="Helvetica") mem_tip = S("MemTip", fontSize=9.5, leading=14, textColor=HexColor("#6c3483"), fontName="Helvetica-Oblique", leftIndent=8) story = [] # ── HEADER BANNER ────────────────────────────────────────────────────────────── banner_data = [[ Paragraph("🧠 Neural Development & Regionalization", title_style), Paragraph("Comprehensive Study Guide • Embryology & Neuroanatomy", subtitle_style) ]] banner = Table(banner_data, colWidths=[content_w]) banner.setStyle(TableStyle([ ("BACKGROUND", (0,0), (-1,-1), DARK_BG), ("ROUNDEDCORNERS", [10]), ("TOPPADDING", (0,0), (-1,-1), 18), ("BOTTOMPADDING",(0,0),(-1,-1), 18), ("LEFTPADDING", (0,0), (-1,-1), 20), ("RIGHTPADDING",(0,0), (-1,-1), 20), ("ALIGN", (0,0), (-1,-1), "CENTER"), ("VALIGN", (0,0), (-1,-1), "MIDDLE"), ])) story.append(banner) story.append(Spacer(1, 14)) # ── HELPER: section banner ───────────────────────────────────────────────────── def section_banner(text, color): t = Table([[Paragraph(text, section_head)]], colWidths=[content_w]) t.setStyle(TableStyle([ ("BACKGROUND", (0,0),(-1,-1), color), ("ROUNDEDCORNERS",[8]), ("TOPPADDING", (0,0),(-1,-1), 8), ("BOTTOMPADDING",(0,0),(-1,-1), 8), ("LEFTPADDING", (0,0),(-1,-1), 14), ("RIGHTPADDING", (0,0),(-1,-1), 14), ])) return t def info_box(text, bg, border_color): t = Table([[Paragraph(text, body)]], colWidths=[content_w]) t.setStyle(TableStyle([ ("BACKGROUND", (0,0),(-1,-1), bg), ("LINEAFTER", (0,0),(0,-1), 4, border_color), ("LINEBEFORE", (0,0),(0,-1), 4, border_color), ("ROUNDEDCORNERS",[6]), ("TOPPADDING", (0,0),(-1,-1), 8), ("BOTTOMPADDING",(0,0),(-1,-1), 8), ("LEFTPADDING", (0,0),(-1,-1), 12), ("RIGHTPADDING", (0,0),(-1,-1), 12), ])) return t def tip_box(text): tip_style = S("TipS", fontSize=9.5, leading=14, textColor=HexColor("#6c3483"), fontName="Helvetica-Oblique") t = Table([[Paragraph("💡 Memory Tip: " + text, tip_style)]], colWidths=[content_w]) t.setStyle(TableStyle([ ("BACKGROUND", (0,0),(-1,-1), LIGHT_PUR), ("LINEBEFORE", (0,0),(0,-1), 4, ACCENT_PUR), ("ROUNDEDCORNERS",[6]), ("TOPPADDING", (0,0),(-1,-1), 7), ("BOTTOMPADDING", (0,0),(-1,-1), 7), ("LEFTPADDING", (0,0),(-1,-1), 12), ("RIGHTPADDING", (0,0),(-1,-1), 12), ])) return t # ════════════════════════════════════════════════════════════════════════════════ # SECTION 1 – Origins # ════════════════════════════════════════════════════════════════════════════════ story.append(section_banner("📌 Section 1: Origins of the Nervous System", ACCENT_BLUE)) story.append(Spacer(1, 8)) story.append(info_box( "The central and peripheral nervous systems originate from specific embryonic structures formed " "early in development. Two key structures drive all neural tissue formation:", LIGHT_BLUE, ACCENT_BLUE)) story.append(Spacer(1, 8)) origins_data = [ [Paragraph("<b>Embryonic Structure</b>", key_style), Paragraph("<b>Gives Rise To</b>", key_style), Paragraph("<b>Cell Types</b>", key_style)], [Paragraph("Neuroepithelia\n(Neural Tube)", body), Paragraph("CNS", body), Paragraph("• Neurons\n• Astrocytes\n• Oligodendrocytes\n• Ependymal cells", body)], [Paragraph("Neural Crest", body), Paragraph("PNS", body), Paragraph("• PNS Neurons\n• Schwann cells\n• Dorsal root ganglion cells", body)], ] origins_table = Table(origins_data, colWidths=[content_w*0.3, content_w*0.2, content_w*0.5]) origins_table.setStyle(TableStyle([ ("BACKGROUND", (0,0),(-1,0), ACCENT_BLUE), ("TEXTCOLOR", (0,0),(-1,0), WHITE), ("FONTNAME", (0,0),(-1,0), "Helvetica-Bold"), ("FONTSIZE", (0,0),(-1,0), 10), ("BACKGROUND", (0,1),(-1,1), LIGHT_BLUE), ("BACKGROUND", (0,2),(-1,2), WHITE), ("ALIGN", (0,0),(-1,-1), "LEFT"), ("VALIGN", (0,0),(-1,-1), "TOP"), ("GRID", (0,0),(-1,-1), 0.5, HexColor("#cce0f5")), ("TOPPADDING", (0,0),(-1,-1), 7), ("BOTTOMPADDING", (0,0),(-1,-1), 7), ("LEFTPADDING", (0,0),(-1,-1), 10), ("RIGHTPADDING", (0,0),(-1,-1), 10), ("ROWBACKGROUNDS",(0,1),(-1,-1), [LIGHT_BLUE, WHITE]), ])) story.append(origins_table) story.append(Spacer(1, 8)) story.append(tip_box("Neural Tube → CNS (Think: Tube runs through the CENTER of the body). Neural Crest → PNS (PERIPHERAL, outside the tube).")) story.append(Spacer(1, 14)) # ════════════════════════════════════════════════════════════════════════════════ # SECTION 2 – Alar vs Basal # ════════════════════════════════════════════════════════════════════════════════ story.append(section_banner("📌 Section 2: Alar Plate vs. Basal Plate", ACCENT_GREEN)) story.append(Spacer(1, 8)) half = (content_w - 8) / 2 alar_col = [ Paragraph("<b>ALAR PLATE</b>", S("AH", fontSize=13, leading=18, textColor=ACCENT_BLUE, fontName="Helvetica-Bold", alignment=TA_CENTER)), Spacer(1, 4), Paragraph("📍 Location: <b>Dorsal</b> (posterior)", body), Paragraph("⚡ Function: <b>Sensory</b>", body), Paragraph("🧬 Inducer: <b>BMPs</b> (Bone Morphogenetic Proteins)", body), Paragraph("🔄 Orientation: Same as spinal cord", body), Spacer(1,4), Paragraph("Receives incoming sensory information from the periphery.", sub_key), ] basal_col = [ Paragraph("<b>BASAL PLATE</b>", S("BH", fontSize=13, leading=18, textColor=ACCENT_ORG, fontName="Helvetica-Bold", alignment=TA_CENTER)), Spacer(1, 4), Paragraph("📍 Location: <b>Ventral</b> (anterior)", body), Paragraph("⚡ Function: <b>Motor</b>", body), Paragraph("🧬 Inducer: <b>SHH</b> (Sonic Hedgehog)", body), Paragraph("🔄 Contains motor neuron pools", body), Spacer(1,4), Paragraph("Sends outgoing motor commands to muscles and glands.", sub_key), ] plates_table = Table([[alar_col, basal_col]], colWidths=[half, half], spaceBefore=0) plates_table.setStyle(TableStyle([ ("BACKGROUND", (0,0),(0,0), LIGHT_BLUE), ("BACKGROUND", (1,0),(1,0), LIGHT_ORG), ("LINEAFTER", (0,0),(0,0), 2, ACCENT_BLUE), ("VALIGN", (0,0),(-1,-1), "TOP"), ("TOPPADDING", (0,0),(-1,-1), 12), ("BOTTOMPADDING", (0,0),(-1,-1), 12), ("LEFTPADDING", (0,0),(-1,-1), 12), ("RIGHTPADDING", (0,0),(-1,-1), 12), ("ROUNDEDCORNERS",[8]), ("BOX", (0,0),(-1,-1), 1, HexColor("#d5d8dc")), ])) story.append(plates_table) story.append(Spacer(1, 8)) story.append(tip_box("'A for Afferent = Alar (Sensory)' | 'B for Below (ventral) = Basal (Motor)' | BMP → Alar → dorsal (B goes up!) | SHH → Basal → ventral")) story.append(Spacer(1, 14)) # ════════════════════════════════════════════════════════════════════════════════ # SECTION 3 – HOX Genes # ════════════════════════════════════════════════════════════════════════════════ story.append(section_banner("📌 Section 3: HOX Genes (Homeobox Genes)", ACCENT_RED)) story.append(Spacer(1, 8)) story.append(info_box( "<b>HOX genes</b> are master regulatory genes that control the body plan along the cranial–caudal " "(head-to-tail) axis. In the nervous system, they govern <b>neural tube segmentation</b> and " "ensure each region of the developing brain and spinal cord gets the correct identity.", LIGHT_RED, ACCENT_RED)) story.append(Spacer(1, 8)) hox_data = [ [Paragraph("<b>Role</b>", key_style), Paragraph("<b>Details</b>", key_style)], [Paragraph("Neural tube segmentation", body), Paragraph("HOX genes divide the neural tube into discrete segments (rhombomeres in the hindbrain).", body)], [Paragraph("Cranial–caudal identity", body), Paragraph("Each segment expresses a unique combination of HOX genes ('HOX code') that determines its fate.", body)], [Paragraph("Limb development", body), Paragraph("Mutations → <b>Syndactyly</b> (fusion of digits/limbs)", body)], [Paragraph("Urogenital development", body), Paragraph("Mutations → <b>Hypospadias</b> (urethral opening on ventral penis)", body)], ] hox_table = Table(hox_data, colWidths=[content_w*0.32, content_w*0.68]) hox_table.setStyle(TableStyle([ ("BACKGROUND", (0,0),(-1,0), ACCENT_RED), ("TEXTCOLOR", (0,0),(-1,0), WHITE), ("FONTNAME", (0,0),(-1,0), "Helvetica-Bold"), ("FONTSIZE", (0,0),(-1,0), 10), ("ALIGN", (0,0),(-1,-1), "LEFT"), ("VALIGN", (0,0),(-1,-1), "TOP"), ("GRID", (0,0),(-1,-1), 0.5, HexColor("#f5c6cb")), ("TOPPADDING", (0,0),(-1,-1), 7), ("BOTTOMPADDING", (0,0),(-1,-1), 7), ("LEFTPADDING", (0,0),(-1,-1), 10), ("RIGHTPADDING", (0,0),(-1,-1), 10), ("ROWBACKGROUNDS",(0,1),(-1,-1), [LIGHT_RED, WHITE]), ])) story.append(hox_table) story.append(Spacer(1, 8)) story.append(tip_box("HOX mutations affect 'outer structures': Syndactyly (fingers stuck together) and Hypospadias (urethral misdirection). Think: HOX = 'HOw eXactly' each body part knows its position.")) story.append(Spacer(1, 14)) # ════════════════════════════════════════════════════════════════════════════════ # SECTION 4 – Neural Tube Vesicle Formation # ════════════════════════════════════════════════════════════════════════════════ story.append(section_banner("📌 Section 4: Neural Tube & Brain Vesicle Formation", ACCENT_PUR)) story.append(Spacer(1, 8)) story.append(info_box( "The neural tube regionalizes into 5 primary brain vesicles. <b>Telencephalon</b> comes first, " "then <b>Diencephalon</b>, followed by the remaining three <b>in alphabetical order</b>: " "Mesencephalon → Metencephalon → Myelencephalon.", LIGHT_PUR, ACCENT_PUR)) story.append(Spacer(1, 10)) # Vesicle flow table vesicle_data = [ ["1", "Telencephalon", "Cerebral cortex, basal ganglia, hippocampus, amygdala"], ["2", "Diencephalon", "Thalamus, hypothalamus, epithalamus, subthalamus"], ["3", "Mesencephalon", "Midbrain (tectum, tegmentum, cerebral peduncles)"], ["4", "Metencephalon", "Pons + Cerebellum"], ["5", "Myelencephalon", "Medulla oblongata"], ] vesicle_styles_bg = [LIGHT_PUR, HexColor("#f0e6ff"), LIGHT_PUR, HexColor("#f0e6ff"), LIGHT_PUR] row_styles = [] for i, bg in enumerate(vesicle_styles_bg): row_styles.append(("BACKGROUND", (0, i+1), (-1, i+1), bg)) vs = [ [Paragraph("<b>#</b>", key_style), Paragraph("<b>Vesicle</b>", key_style), Paragraph("<b>Develops Into</b>", key_style)], ] for row in vesicle_data: vs.append([Paragraph(row[0], body), Paragraph(f"<b>{row[1]}</b>", body), Paragraph(row[2], body)]) vt = Table(vs, colWidths=[content_w*0.06, content_w*0.3, content_w*0.64]) vt.setStyle(TableStyle([ ("BACKGROUND", (0,0),(-1,0), ACCENT_PUR), ("TEXTCOLOR", (0,0),(-1,0), WHITE), ("FONTNAME", (0,0),(-1,0), "Helvetica-Bold"), ("FONTSIZE", (0,0),(-1,0), 10), ("ALIGN", (0,0),(0,-1), "CENTER"), ("ALIGN", (1,0),(-1,-1), "LEFT"), ("VALIGN", (0,0),(-1,-1), "MIDDLE"), ("GRID", (0,0),(-1,-1), 0.5, HexColor("#d7bde2")), ("TOPPADDING", (0,0),(-1,-1), 8), ("BOTTOMPADDING", (0,0),(-1,-1), 8), ("LEFTPADDING", (0,0),(-1,-1), 10), ("RIGHTPADDING", (0,0),(-1,-1), 10), ("ROWBACKGROUNDS",(0,1),(-1,-1), [LIGHT_PUR, HexColor("#f0e6ff")]), ])) story.append(vt) story.append(Spacer(1, 8)) story.append(tip_box("Order: Telo → Dien → then ALPHABETICAL: Mes → Met → Myel. Mnemonic: 'Tiny Dogs Make Many Mistakes'")) story.append(Spacer(1, 14)) # ════════════════════════════════════════════════════════════════════════════════ # SECTION 5 – Visual Note (the image) # ════════════════════════════════════════════════════════════════════════════════ story.append(section_banner("🖼️ Section 5: Visual Summary Diagram", ACCENT_GREEN)) story.append(Spacer(1, 10)) img = Image("/tmp/workspace/neural-notes/neural_visual.png", width=content_w, height=content_w*0.72) story.append(img) story.append(Spacer(1, 8)) # ════════════════════════════════════════════════════════════════════════════════ # QUICK REFERENCE CHEAT SHEET # ════════════════════════════════════════════════════════════════════════════════ story.append(Spacer(1, 6)) story.append(section_banner("⚡ Quick Reference Cheat Sheet", HexColor("#2c3e50"))) story.append(Spacer(1, 8)) qr_data = [ [Paragraph("<b>Concept</b>", key_style), Paragraph("<b>Key Fact</b>", key_style), Paragraph("<b>Mnemonic</b>", key_style)], [Paragraph("Neural Tube → CNS", body), Paragraph("Neurons + Astrocytes + Oligodendrocytes + Ependymal", body), Paragraph("NAOE", S("M", fontSize=9.5, textColor=ACCENT_PUR, fontName="Helvetica-Bold"))], [Paragraph("Neural Crest → PNS", body), Paragraph("PNS neurons, Schwann cells, DRG", body), Paragraph("'Crest = Peripheral Crown'", S("M", fontSize=9.5, textColor=ACCENT_PUR, fontName="Helvetica-Bold"))], [Paragraph("Alar = Sensory", body), Paragraph("Dorsal | Induced by BMPs", body), Paragraph("A = Afferent", S("M", fontSize=9.5, textColor=ACCENT_BLUE, fontName="Helvetica-Bold"))], [Paragraph("Basal = Motor", body), Paragraph("Ventral | Induced by SHH", body), Paragraph("B = Below + efferent", S("M", fontSize=9.5, textColor=ACCENT_ORG, fontName="Helvetica-Bold"))], [Paragraph("HOX mutations", body), Paragraph("Syndactyly + Hypospadias", body), Paragraph("'HOX wrecks limbs & plumbing'", S("M", fontSize=9.5, textColor=ACCENT_RED, fontName="Helvetica-Bold"))], [Paragraph("Vesicle order", body), Paragraph("Telo → Dien → Mes → Met → Myel", body), Paragraph("Tiny Dogs Make Many Mistakes", S("M", fontSize=9.5, textColor=ACCENT_PUR, fontName="Helvetica-Bold"))], ] qrt = Table(qr_data, colWidths=[content_w*0.25, content_w*0.42, content_w*0.33]) qrt.setStyle(TableStyle([ ("BACKGROUND", (0,0),(-1,0), HexColor("#2c3e50")), ("TEXTCOLOR", (0,0),(-1,0), WHITE), ("FONTNAME", (0,0),(-1,0), "Helvetica-Bold"), ("FONTSIZE", (0,0),(-1,0), 10), ("ALIGN", (0,0),(-1,-1), "LEFT"), ("VALIGN", (0,0),(-1,-1), "TOP"), ("GRID", (0,0),(-1,-1), 0.5, HexColor("#d5d8dc")), ("TOPPADDING", (0,0),(-1,-1), 7), ("BOTTOMPADDING", (0,0),(-1,-1), 7), ("LEFTPADDING", (0,0),(-1,-1), 10), ("RIGHTPADDING", (0,0),(-1,-1), 10), ("ROWBACKGROUNDS",(0,1),(-1,-1), [HexColor("#f2f3f4"), WHITE]), ])) story.append(qrt) story.append(Spacer(1, 16)) # Footer footer_data = [[Paragraph( "📖 Neural Development & Regionalization • Study Guide • Generated for exam preparation", S("F", fontSize=8.5, textColor=WHITE, fontName="Helvetica", alignment=TA_CENTER))]] footer_table = Table(footer_data, colWidths=[content_w]) footer_table.setStyle(TableStyle([ ("BACKGROUND", (0,0),(-1,-1), DARK_BG), ("TOPPADDING", (0,0),(-1,-1), 8), ("BOTTOMPADDING", (0,0),(-1,-1), 8), ("LEFTPADDING", (0,0),(-1,-1), 14), ("RIGHTPADDING", (0,0),(-1,-1), 14), ("ROUNDEDCORNERS",[8]), ])) story.append(footer_table) doc.build(story) print("PDF created successfully!") EOF
Neural Development Study Guide
PDF Document · PDF
| Section | Content |
|---|---|
| Section 1 | Origins table - Neural Tube vs Neural Crest with all cell types |
| Section 2 | Alar vs Basal Plate side-by-side comparison (function, location, inducer) |
| Section 3 | HOX Genes - roles, mutations, and clinical conditions |
| Section 4 | All 5 brain vesicles with what each develops into |
| Section 5 | Your visual diagram image embedded |
| Cheat Sheet | Quick reference table with all mnemonics in one place |
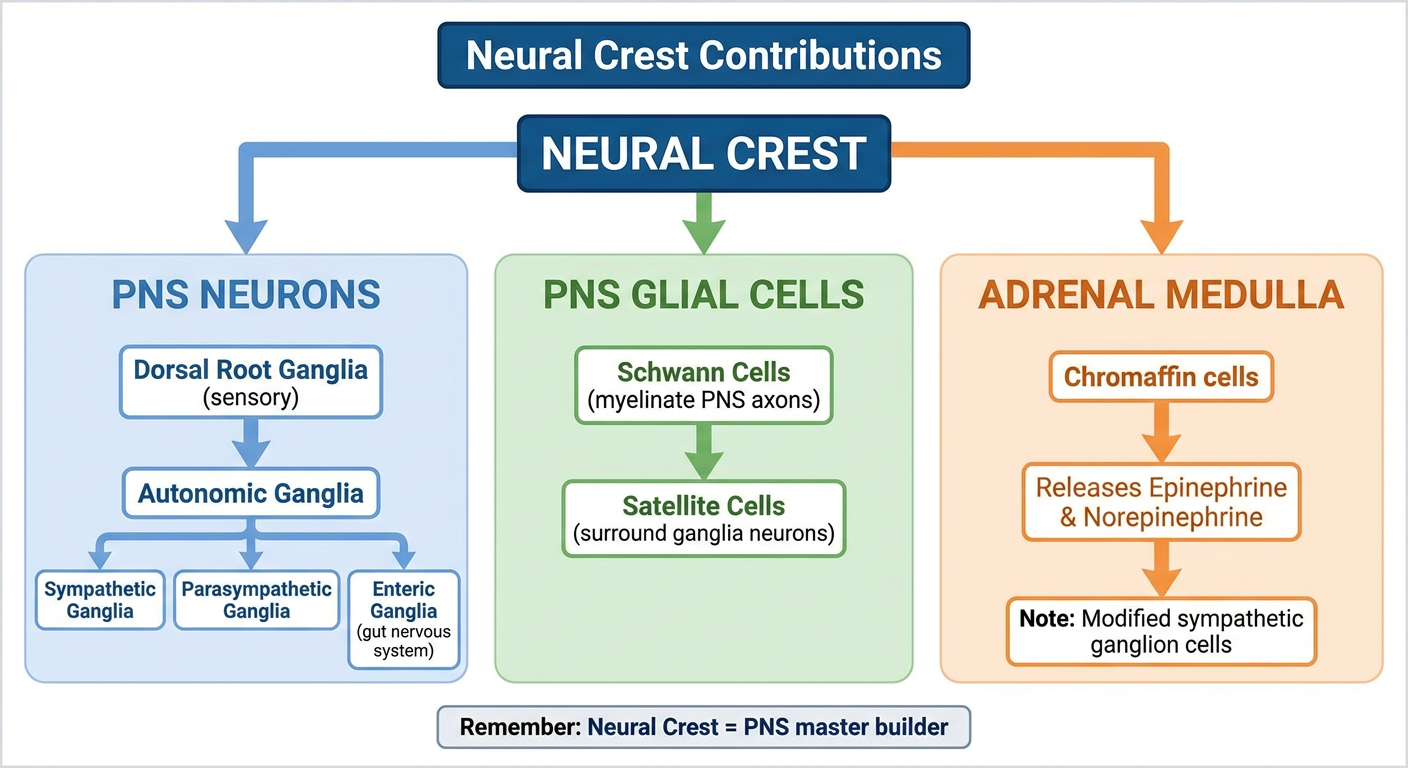
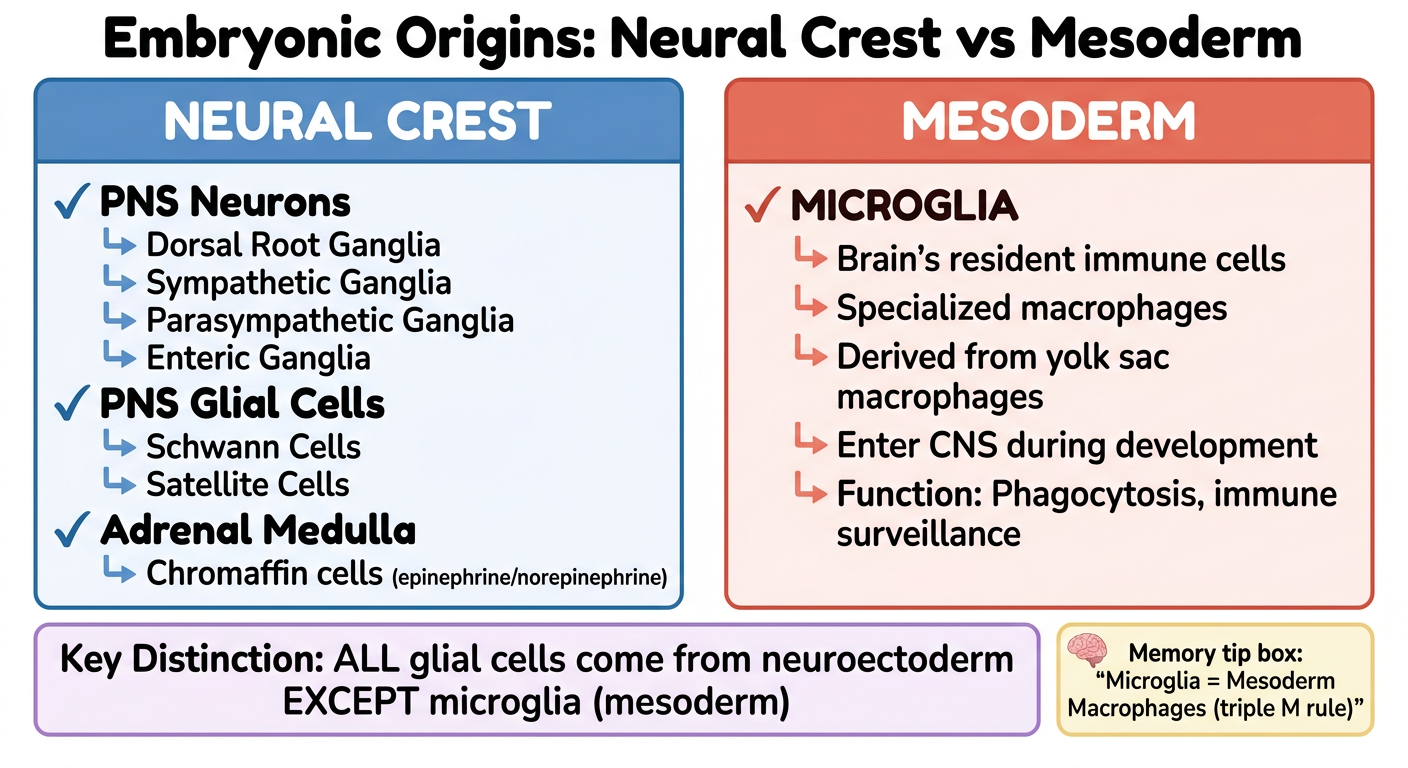
Neural Crest and Mesoderm Contributions The neural crest contributes to the formation of PNS neurons, including dorsal root ganglia and autonomic ganglia (sympathetic, parasympathetic, enteric), as well as PNS glial cells like Schwann cells and satellite cells. It also contributes to the adrenal medulla. The mesoderm gives rise to microglia, which are specialized macrophages. Make images to know the concept better
A clean colorful medical study infographic titled "Neural Crest Contributions" showing a branching tree/flowchart diagram: ROOT NODE (center-top): "NEURAL CREST" in bold dark box Branching into 3 main categories with colored boxes: Branch 1 (blue) - "PNS NEURONS": - Dorsal Root Ganglia (sensory) - Autonomic Ganglia: → Sympathetic Ganglia → Parasympathetic Ganglia → Enteric Ganglia (gut nervous system) Branch 2 (green) - "PNS GLIAL CELLS": - Schwann Cells (myelinate PNS axons) - Satellite Cells (surround ganglia neurons) Branch 3 (orange) - "ADRENAL MEDULLA": - Chromaffin cells - Releases Epinephrine & Norepinephrine - Note: Modified sympathetic ganglion cells Small footnote box at bottom: "Remember: Neural Crest = PNS master builder" Use pastel backgrounds, color-coded branches, bold headings, arrows connecting nodes, clean white background, medical textbook infographic style. Very clear and readable.
A clean colorful medical study infographic comparing two embryonic origins side by side: TITLE: "Embryonic Origins: Neural Crest vs Mesoderm" LEFT PANEL (blue theme) - "NEURAL CREST": Large header box. Below it, a list of all contributions: ✓ PNS Neurons - Dorsal Root Ganglia - Sympathetic Ganglia - Parasympathetic Ganglia - Enteric Ganglia ✓ PNS Glial Cells - Schwann Cells - Satellite Cells ✓ Adrenal Medulla - Chromaffin cells (epinephrine/norepinephrine) RIGHT PANEL (red/orange theme) - "MESODERM": Large header box. Below it: ✓ MICROGLIA - Brain's resident immune cells - Specialized macrophages - Derived from yolk sac macrophages - Enter CNS during development - Function: Phagocytosis, immune surveillance BOTTOM COMPARISON BOX: "Key Distinction: ALL glial cells come from neuroectoderm EXCEPT microglia (mesoderm)" Memory tip box: "Microglia = Mesoderm Macrophages (triple M rule)" Pastel colors, clean layout, bold text, arrows, white background, medical education style.
| Structure | Origin | Tip |
|---|---|---|
| PNS Neurons (DRG, autonomic, enteric) | Neural Crest | "Crest builds the periphery" |
| Schwann Cells + Satellite Cells | Neural Crest | PNS glia = Neural Crest |
| Adrenal Medulla | Neural Crest | Modified sympathetic ganglion |
| Microglia | Mesoderm | Triple M: Microglia = Mesoderm Macrophages |
The #1 exam trap: All glial cells come from neuroectoderm EXCEPT microglia - they are the odd ones out, derived from mesoderm (yolk sac macrophages).
Notochord and Neural Plate The notochord, a precursor to the nucleus pulposus of intervertebral discs, induces the ectoderm to form neuroectoderm, leading to the development of the neural plate. The neural plate subsequently gives rise to the neural tube and neural crest cells. The lateral walls of the neural tube are divided into alar and basal plates, with the alar plate being sensory and the basal plate being motor. Same make images to knows conceot better like visual diagram of how it made
A detailed medical embryology infographic showing the step-by-step process of neural tube formation, drawn as a left-to-right sequential flowchart with anatomical illustrations at each step: TITLE at top: "Notochord → Neural Plate → Neural Tube Formation" STEP 1 (leftmost): Label: "NOTOCHORD" Simple oval/rod structure underneath ectoderm layer Arrow pointing up labeled "Induces" Note below: "• Precursor to Nucleus Pulposus of intervertebral discs" STEP 2: Label: "ECTODERM becomes NEUROECTODERM" Show flat ectoderm layer thickening in the middle Note: "Notochord signals ectoderm to specialize" STEP 3: Label: "NEURAL PLATE" Show thickened flat plate of cells (top-down view) Note: "Neuroectoderm thickens to form flat neural plate" STEP 4: Label: "NEURAL GROOVE" Show the plate beginning to fold inward, forming a groove (cross-section view) Neural folds rising on both sides STEP 5: Label: "NEURAL TUBE + NEURAL CREST" Show the tube fully closed Neural crest cells pinching off from the top (dorsal) edges Arrow pointing to tube: "→ CNS" Arrow pointing to crest cells: "→ PNS" STEP 6 (rightmost): Cross-section of closed neural tube showing: - TOP (dorsal): ALAR PLATE - blue - "SENSORY" - BOTTOM (ventral): BASAL PLATE - orange - "MOTOR" - Neural crest cells migrating outward Use soft pastel colors, clear anatomical labels, bold arrows showing progression, clean white background, medical textbook style. Make it visually clear and memorable for exam study.
A detailed medical cross-section anatomy diagram titled "Neural Tube Cross-Section & Key Relationships" Show a large, clear CROSS-SECTION of the developing neural tube in the center of the image with these labeled parts: OUTER STRUCTURE: - Label at very top: "DORSAL (back)" - Label at very bottom: "VENTRAL (front)" INSIDE THE NEURAL TUBE (cross-section circle/oval): - TOP HALF shaded BLUE labeled: "ALAR PLATE" with arrow: "→ SENSORY (Afferent)" and "Induced by BMPs" - BOTTOM HALF shaded ORANGE labeled: "BASAL PLATE" with arrow: "→ MOTOR (Efferent)" and "Induced by SHH (Sonic Hedgehog)" - Thin line dividing them labeled: "Sulcus Limitans" OUTSIDE THE TUBE - LEFT SIDE: Small rod structure labeled "NOTOCHORD" with upward arrow labeled "Induces SHH → Basal plate" Below notochord: "Later becomes Nucleus Pulposus of intervertebral disc" OUTSIDE THE TUBE - TOP CORNERS: Two clusters of cells labeled "NEURAL CREST CELLS" migrating outward Arrow: "→ PNS neurons, Schwann cells, Adrenal medulla" BOTTOM INFO BOX: Two columns: Left: "Alar Plate (Dorsal/Blue): Sensory | BMPs | Afferent signals | Same orientation as spinal cord" Right: "Basal Plate (Ventral/Orange): Motor | Sonic Hedgehog | Efferent signals | Motor neuron pools" Clean white background, bright colors, bold labels, medical textbook style, very clear anatomy diagram.
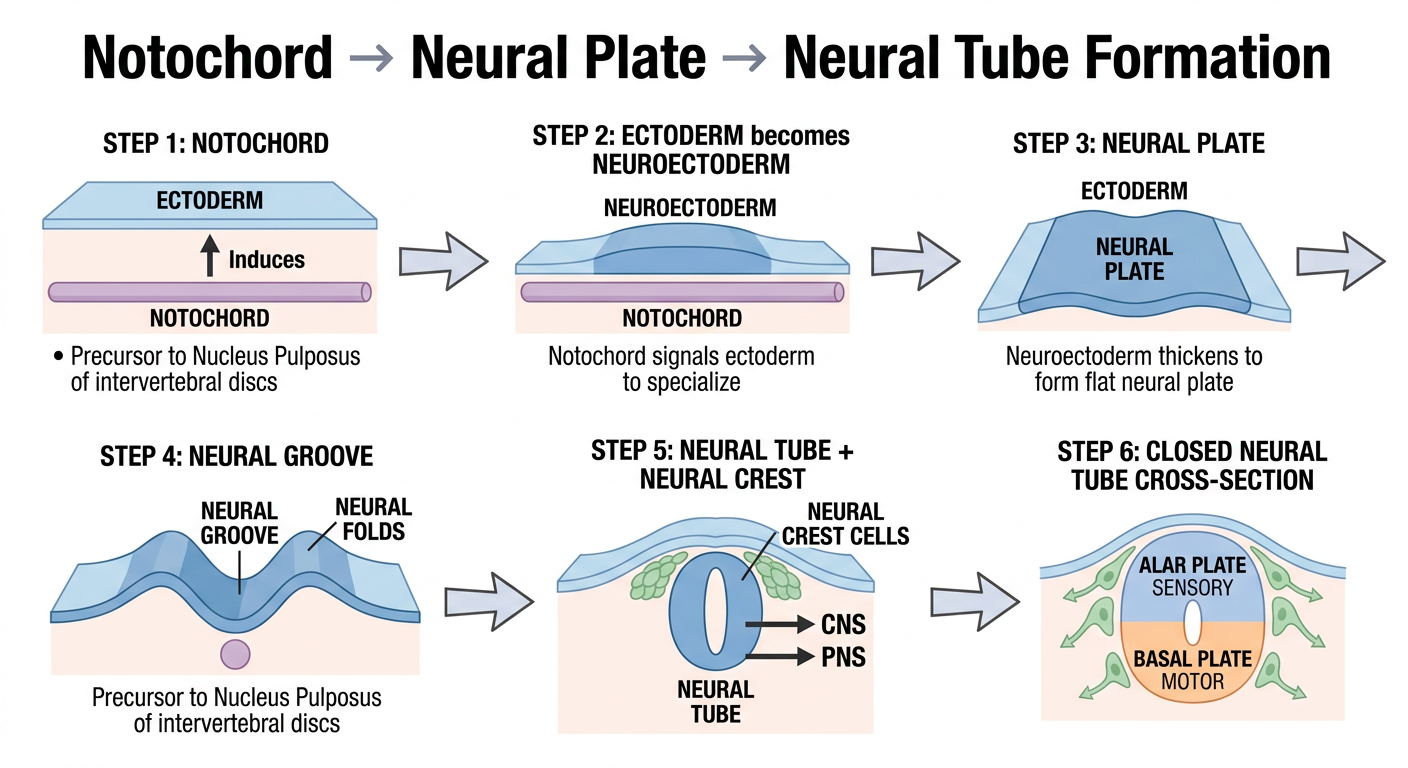
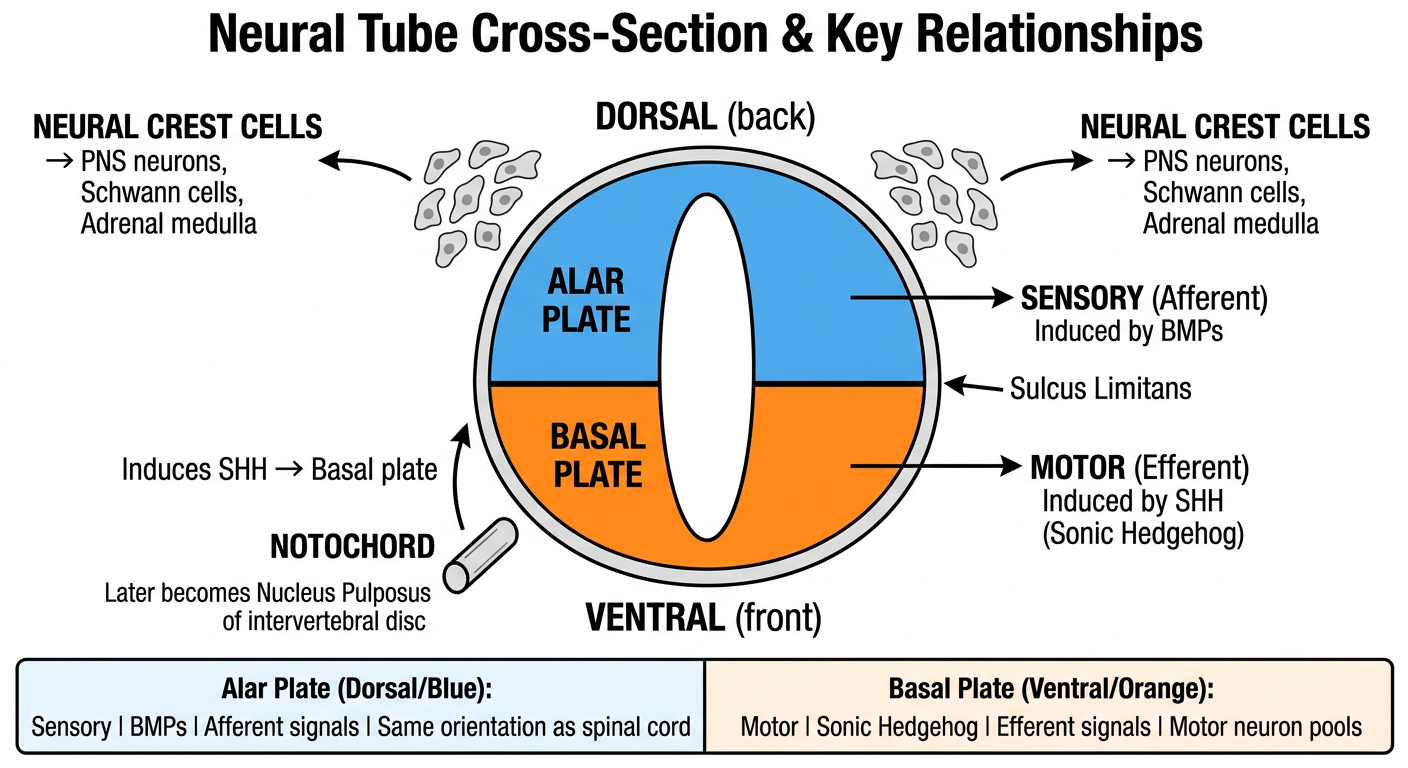
NOTOCHORD
↓ (signals ectoderm)
NEUROECTODERM
↓ (thickens)
NEURAL PLATE
↓ (folds inward)
NEURAL GROOVE
↓ (fuses/closes)
NEURAL TUBE + NEURAL CREST cells (pinch off at edges)
↓ ↓
CNS PNS
- Notochord's adult remnant = Nucleus Pulposus (inside intervertebral discs) - a common MCQ trap
- Sulcus Limitans = the dividing line between alar (sensory) and basal (motor) plates inside the tube
- Neural crest cells are sometimes called the "4th germ layer" because of how many structures they form
Spina Bifida Occulta Neural Tube Defects Neural tube defects (NTDs) result from the failure of the neural tube to close completely by week 4 of development. This condition is associated with maternal folate deficiency or exposure to teratogens Such as valproate and carbamazepine during pregnancy. Diagnosis is typically made via ultrasound, maternal serum alpha-fetoprotein (AFP), and/or amniotic fluid acetylcholinesterase (AChE), which are elevated in open NTDS. Same for this make images to make concept better
A clean medical study infographic titled "Neural Tube Defects (NTDs) - Overview" with 3 clearly separated sections: SECTION 1 - RED ALERT BOX at top: "CAUSE: Failure of neural tube to close by WEEK 4" Two sub-boxes side by side: Left (yellow): "Folate Deficiency" with note "Most preventable cause - take folic acid pre-conception" Right (red): "Teratogens: Valproate, Carbamazepine" with note "Antiepileptic drugs - avoid in pregnancy" SECTION 2 - DIAGNOSIS TABLE (blue theme): Title: "How to Diagnose NTDs" Three columns: 1. Ultrasound - "Structural visualization of defect" 2. Maternal Serum AFP - "ELEVATED in open NTDs" with up arrow 3. Amniotic Fluid AChE - "ELEVATED in open NTDs" with up arrow Note at bottom: "AFP + AChE only elevated in OPEN NTDs (not closed/covered)" SECTION 3 - TYPES COMPARISON (green theme): Title: "Types of Spina Bifida" Three boxes left to right: Box 1 (lightest): "Spina Bifida OCCULTA - Hidden defect, skin covered, tuft of hair, no neurological defect" Box 2 (medium): "MENINGOCELE - Meninges herniate out, CSF-filled sac, skin covered, mild symptoms" Box 3 (darkest red): "MYELOMENINGOCELE - Meninges + spinal cord herniate, open/exposed, severe neurological deficits" Memory tip at bottom: "O-M-M: Occulta (hidden) → Meningocele (meninges) → Myelomeningocele (worst)" Clean white background, bold text, color-coded severity, medical textbook infographic style.
A detailed medical anatomy diagram showing the 3 types of Spina Bifida as side-by-side cross-section spine illustrations, titled "Spina Bifida: Types Comparison - Cross-Section View" Show 3 vertebral cross-sections side by side, each showing the spine from behind with different levels of defect: ILLUSTRATION 1 - "SPINA BIFIDA OCCULTA" (green/mild): - Vertebral arch has a small gap/split but skin is intact over it - Show tuft of hair or dimple on skin surface - Spinal cord is normal inside - Label: "Vertebral arch defect only" - Label: "Skin intact - CLOSED" - Label: "No cord herniation" - Label: "Often asymptomatic" - AFP: NORMAL (not elevated) ILLUSTRATION 2 - "MENINGOCELE" (yellow/moderate): - Vertebral gap with meninges bulging out as a sac - Sac is filled with CSF (show fluid inside) - Spinal cord stays inside the spinal canal (not in sac) - Skin covers the sac - Label: "Meninges herniate" - Label: "CSF-filled sac" - Label: "Cord NOT involved" - AFP: ELEVATED (if open) ILLUSTRATION 3 - "MYELOMENINGOCELE" (red/severe): - Large open defect - Both meninges AND spinal cord herniate into the sac - Sac may be open/exposed (no skin covering) - Show nerve roots inside the sac - Label: "Meninges + Spinal cord herniate" - Label: "OPEN defect - exposed" - Label: "Severe neurological deficits" - Label: "Paralysis, bladder/bowel dysfunction" - AFP + AChE: BOTH ELEVATED Bottom severity bar: Green → Yellow → Red (Mild to Severe) Caption: "Most common form requiring surgery: Myelomeningocele" Clean white background, accurate anatomy, color-coded severity scale, bold labels, medical textbook style.
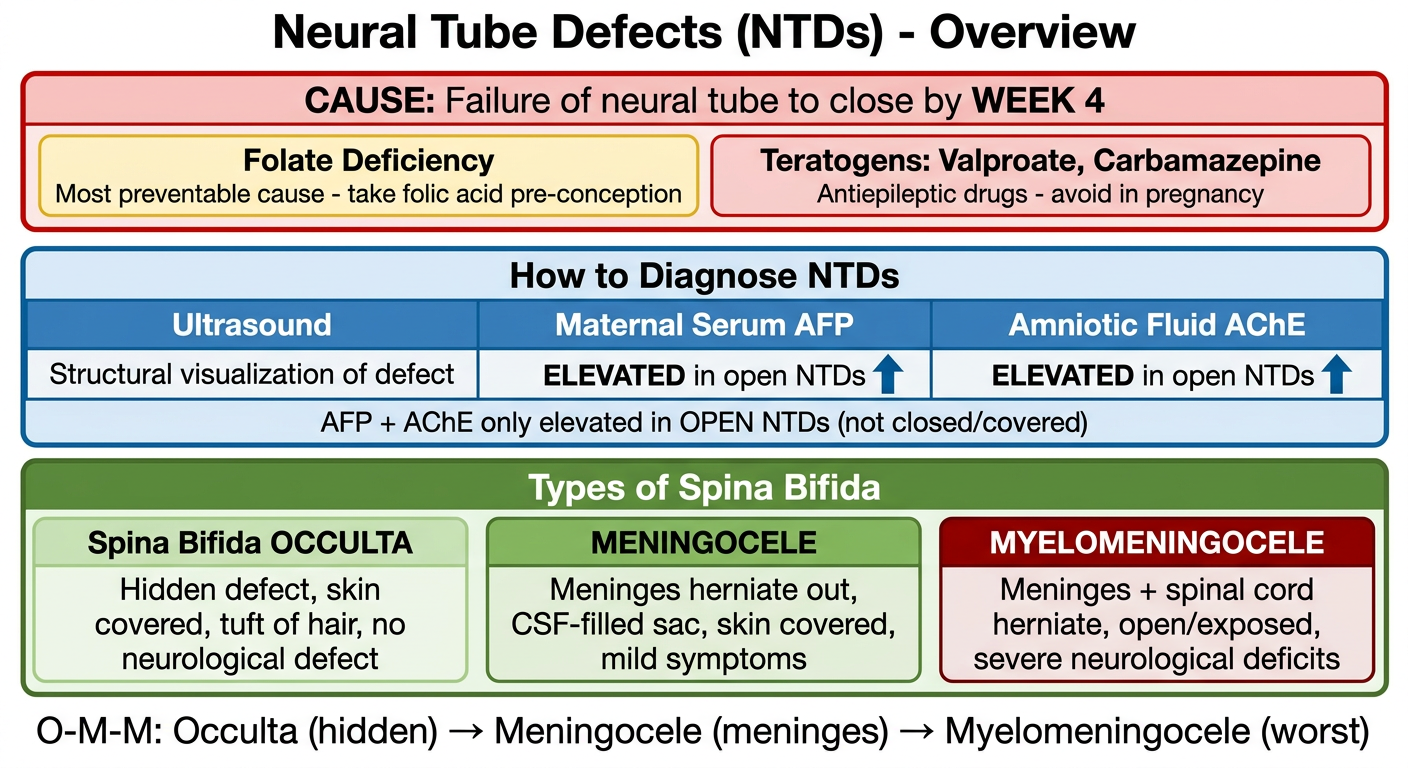
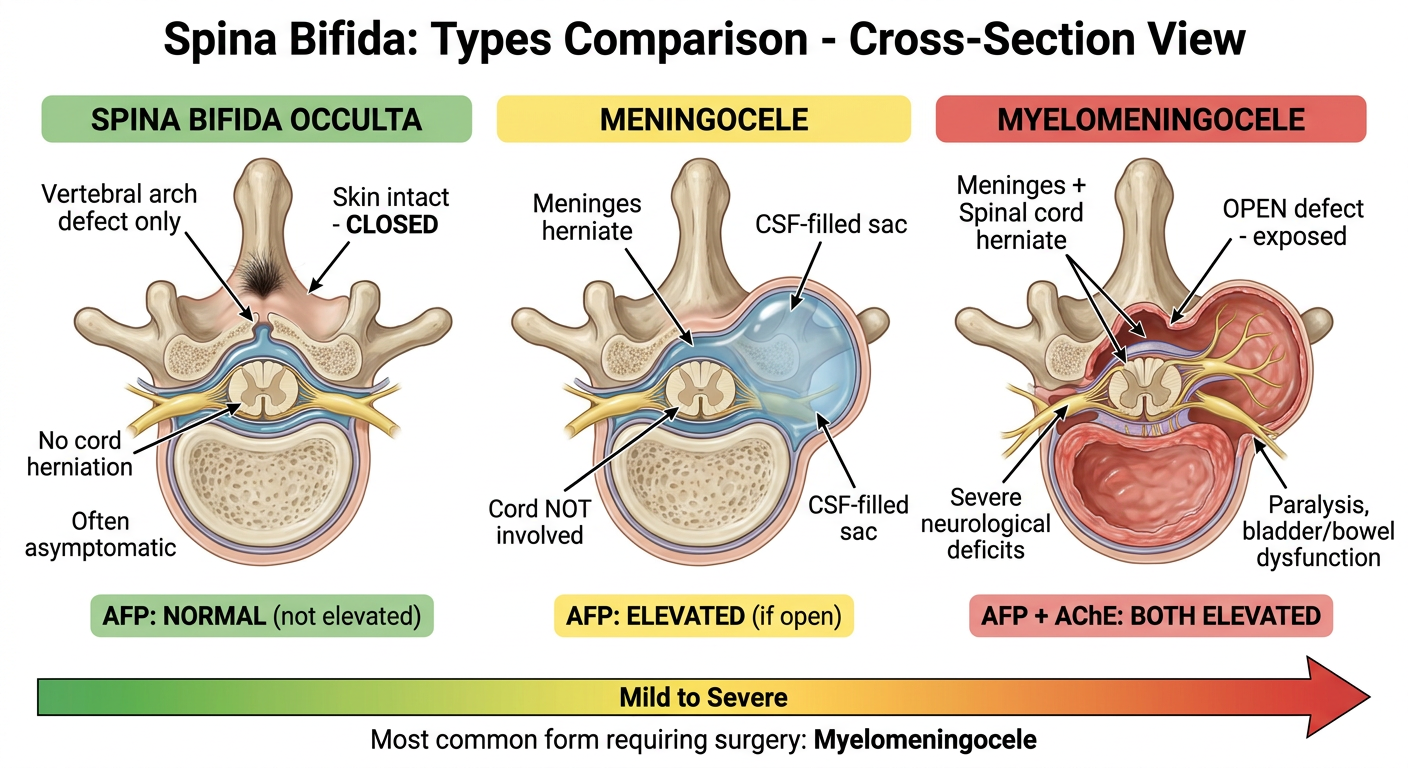
| Type | Defect | Skin | AFP/AChE | Symptoms |
|---|---|---|---|---|
| Occulta | Vertebral arch gap only | Intact (hair/dimple) | Normal | Usually none |
| Meningocele | Meninges herniate | Covered | Elevated (if open) | Mild |
| Myelomeningocele | Meninges + cord herniate | Open/exposed | Both elevated | Paralysis, bladder/bowel |
- Week 4 = deadline for neural tube closure - this is when NTDs occur
- AFP + AChE elevated only in OPEN NTDs (Occulta is closed = normal levels)
- Valproate & Carbamazepine are the two classic teratogen drugs - both are antiepileptics
Prevention: Folic acid supplementation before conception (not after pregnancy confirmed) reduces NTD risk by ~70%
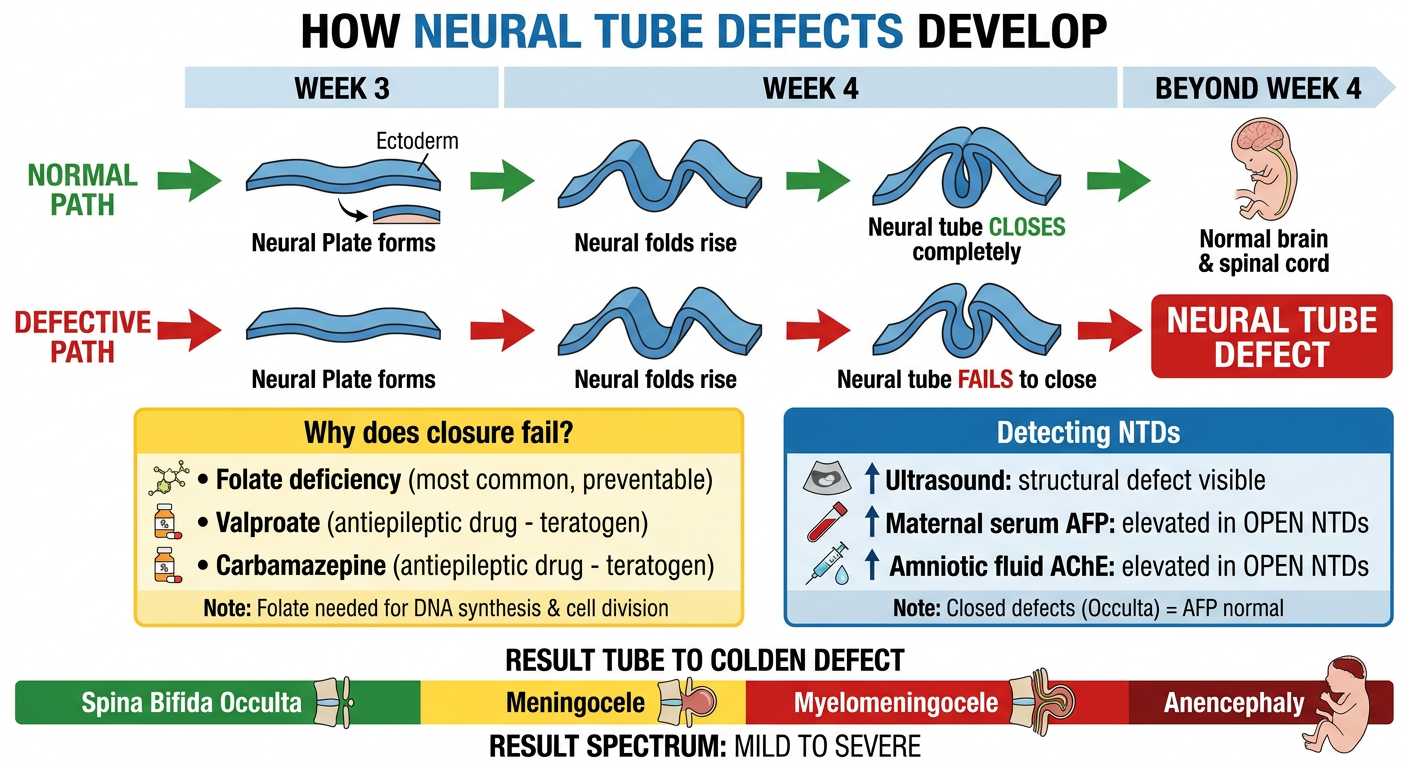
Spina Bifida Occulta Neural Tube Defects Neural tube defects (NTDs) result from the failure of the neural tube to close completely by week 4 of development. This condition is associated with maternal folate deficiency or exposure to teratogens Such as valproate and carbamazepine during pregnancy. Diagnosis is typically made via ultrasound, maternal serum alpha-fetoprotein (AFP), and/or amniotic fluid acetylcholinesterase (AChE), which are elevated in open NTDS. Make images to make concept visual better like visual diagram how it made
A medical embryology infographic showing "How Neural Tube Defects Develop" as a timeline/process diagram from left to right: TIMELINE FLOW (top of image): NORMAL PATH (green arrow, top row): Week 3: "Neural Plate forms" → Week 4: "Neural folds rise" → "Neural tube CLOSES completely" → "Normal brain & spinal cord" DEFECTIVE PATH (red arrow, bottom row): Week 3: "Neural Plate forms" → Week 4: "Neural folds rise" → "Neural tube FAILS to close" → RED BOX: "NEURAL TUBE DEFECT" CAUSES BOX (yellow, center-left): Title: "Why does closure fail?" • Folate deficiency (most common, preventable) • Valproate (antiepileptic drug - teratogen) • Carbamazepine (antiepileptic drug - teratogen) Note: "Folate needed for DNA synthesis & cell division" DIAGNOSIS BOX (blue, center-right): Title: "Detecting NTDs" Three items with UP arrows: ↑ Ultrasound: structural defect visible ↑ Maternal serum AFP: elevated in OPEN NTDs ↑ Amniotic fluid AChE: elevated in OPEN NTDs Note at bottom: "Closed defects (Occulta) = AFP normal" RESULT BOX (bottom): Spectrum bar from mild to severe: [GREEN] Spina Bifida Occulta → [YELLOW] Meningocele → [RED] Myelomeningocele → [DARK RED] Anencephaly Clean white background, color-coded steps, bold arrows, medical textbook style, easy to memorize.
A detailed medical anatomy educational diagram focused specifically on "Spina Bifida Occulta - Deep Dive" showing: TITLE at top: "Spina Bifida Occulta - The Hidden Defect" LARGE CENTER ILLUSTRATION: Draw a realistic posterior (back) view of lower lumbar spine vertebra with: - Vertebral body visible - Posterior vertebral arch has a MIDLINE GAP/SPLIT (incomplete fusion) - Spinal cord shown INTACT inside the spinal canal - Overlying skin is FULLY INTACT and CLOSED - On the skin surface above the defect: show a small tuft of hair AND a skin dimple - Dashed circle highlighting the gap in the bone LABELS with arrows pointing to each structure: → "Incomplete vertebral arch fusion" (pointing to bone gap) → "Spinal cord - INTACT, not herniated" (pointing to cord) → "Skin intact - fully covered" (pointing to skin) → "Tuft of hair - cutaneous marker" (pointing to hair) → "Dimple - cutaneous marker" (pointing to dimple) → "Spinal canal - normal" (pointing to canal) RIGHT SIDE - COMPARISON MINI DIAGRAM: Small cross-section showing: Normal vertebra (left) vs Spina Bifida Occulta (right, showing gap in arch) BOTTOM INFO BOXES - 3 boxes: Box 1 GREEN: "Symptoms: Usually NONE - asymptomatic, found incidentally" Box 2 BLUE: "Diagnosis: X-ray or MRI showing bony defect; AFP = NORMAL" Box 3 YELLOW: "Key fact: Most common NTD. Skin acts as barrier = closed defect" Memory tip: "OCCULTA = OCCULT = HIDDEN - the defect hides under normal skin" White background, anatomically accurate, clear labels, color-coded, medical school study style.
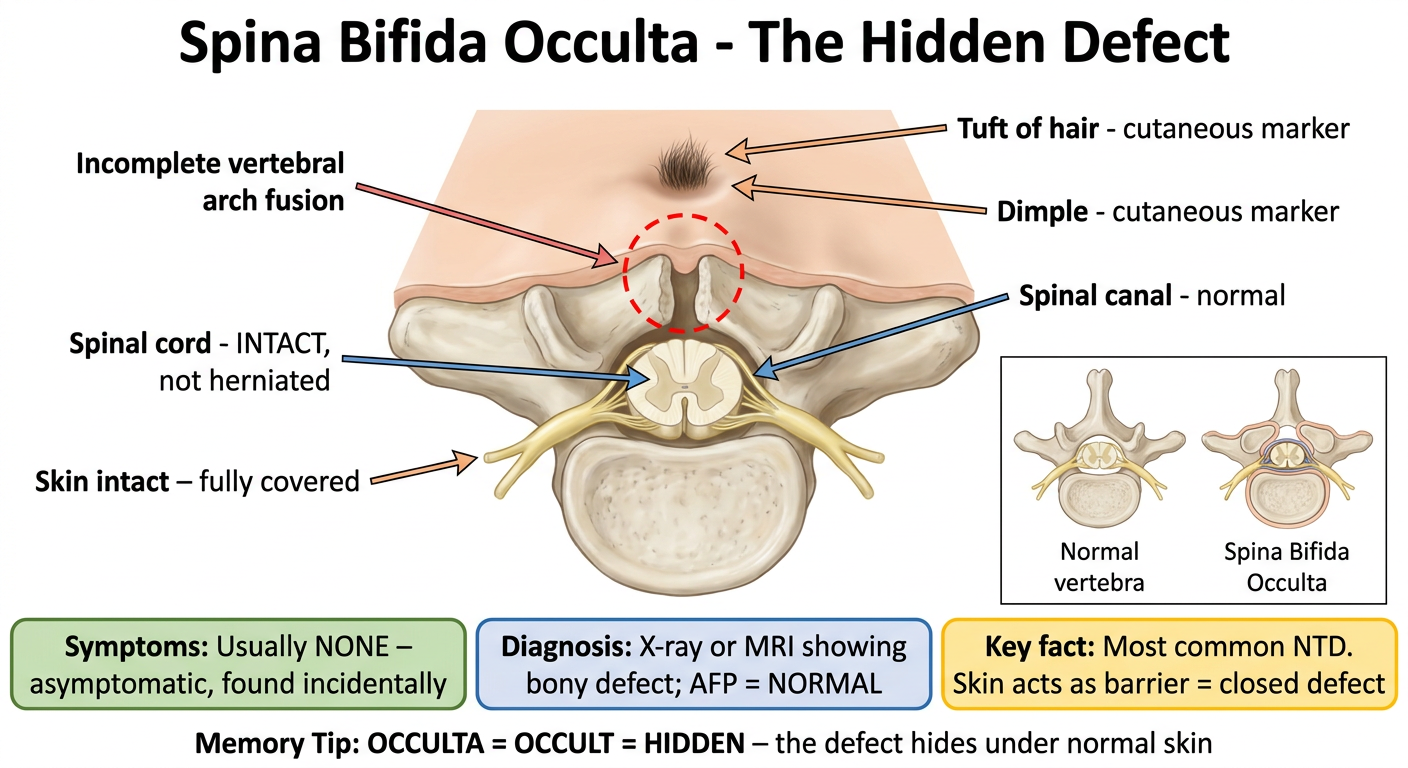
| Feature | Detail |
|---|---|
| Meaning | "Occulta" = Latin for hidden |
| Defect | Vertebral arch fails to fuse - bone gap only |
| Skin | Fully intact - closed defect |
| Cord | Normal - no herniation |
| Signs | Tuft of hair / skin dimple over lower back |
| Symptoms | Usually none - found incidentally on X-ray |
| AFP/AChE | Normal (closed = nothing leaks into amniotic fluid) |
| Treatment | Usually none needed |
OPEN defect (Myelomeningocele)
→ fetal proteins leak into amniotic fluid
→ AFP & AChE ↑↑↑ in maternal serum
CLOSED defect (Occulta)
→ skin seals everything in
→ AFP stays NORMAL
Types of Spinal Dysraphism • Spina Bifida Occulta: A closed NTD where the caudal neural tube fails to close, but there is no herniation. The dura remains intact. It is usually seen at lower vertebral levels and is associated with a tuft of hair or skin dimple at the level of the bony defect. • Meningocele: An open NTD where the meninges herniate through a bony defect, but no neural tissue is involved. • Myelomeningocele: An open NTD where both meninges and neural tissue, such as the cauda equina, herniate through a bony defect. • Myeloschisis: An open NTD characterized by exposed, unfused neural tissue without skin or meningeal COvering. Make images to make concept visual better like visual diagram how it made
A detailed medical anatomy diagram showing all 4 types of Spinal Dysraphism as side-by-side cross-section spine illustrations. Title: "Types of Spinal Dysraphism - Visual Comparison" Show 4 vertebral cross-sections in a 2x2 grid layout, each showing the spine from a posterior cross-section view: PANEL 1 - TOP LEFT - "SPINA BIFIDA OCCULTA" (green border, CLOSED label): - Vertebral arch has a small midline gap in the bone (incomplete fusion) - Spinal cord sits INSIDE spinal canal - perfectly normal - Dura is INTACT - Skin is fully closed over everything - Small tuft of hair drawn on skin surface - Labels: "Bone gap only", "Dura intact", "No herniation", "Skin closed", "CLOSED NTD" PANEL 2 - TOP RIGHT - "MENINGOCELE" (yellow/orange border, OPEN label): - Vertebral arch has a larger gap - Meninges bulge outward through the gap forming a round sac - Sac is filled with CSF (light blue fluid inside) - Spinal cord stays INSIDE the canal - not in the sac - Skin may or may not cover the sac - Labels: "Meninges herniate", "CSF-filled sac", "No neural tissue in sac", "OPEN NTD" PANEL 3 - BOTTOM LEFT - "MYELOMENINGOCELE" (orange/red border, OPEN label): - Large vertebral gap - Both meninges AND spinal cord/nerve roots herniate into the sac - Show nerve roots (cauda equina) clearly inside the sac - Sac is larger than meningocele - Labels: "Meninges + neural tissue herniate", "Cauda equina in sac", "Severe neurological deficits", "Most common serious NTD", "OPEN NTD" PANEL 4 - BOTTOM RIGHT - "MYELOSCHISIS" (dark red border, OPEN + WORST label): - Wide open vertebral defect - Neural tissue is completely EXPOSED - flat open neural plate visible - NO meningeal covering - NO skin covering - Raw exposed spinal cord tissue - Labels: "Exposed unfused neural tissue", "No meninges covering", "No skin covering", "Most severe", "OPEN NTD" BOTTOM ROW: Severity bar from GREEN to DARK RED: Occulta → Meningocele → Myelomeningocele → Myeloschisis Clean white background, color-coded by severity, anatomically accurate cross-sections, bold clear labels, medical textbook style.
A clean medical study infographic titled "Spinal Dysraphism - What's Inside Each Type?" showing a structured comparison table with visual icons: TITLE: "Spinal Dysraphism: Layer-by-Layer Comparison" MAIN COMPARISON TABLE with 5 columns and 5 rows: HEADER ROW (dark navy): Type | Bone Defect | Dura/Meninges | Neural Tissue | Skin Cover ROW 1 (light green): SPINA BIFIDA OCCULTA | ✓ Gap in arch | ✓ Intact | ✓ Normal inside | ✓ Closed ROW 2 (light yellow): MENINGOCELE | ✓ Bony defect | ✗ Herniates out (CSF sac) | ✓ Stays in canal | ± May be covered ROW 3 (light orange): MYELOMENINGOCELE | ✓ Bony defect | ✗ Herniates out | ✗ Herniates into sac (cauda equina) | ✗ Open/exposed ROW 4 (light red): MYELOSCHISIS | ✓ Wide defect | ✗ Absent entirely | ✗ Exposed flat neural plate | ✗ No covering at all BELOW THE TABLE - Two side-by-side info boxes: Left box (blue): "CLOSED NTDs" • Spina Bifida Occulta only • Skin covers defect • AFP = NORMAL • Usually asymptomatic Right box (red): "OPEN NTDs" • Meningocele, Myelomeningocele, Myeloschisis • Neural tissue or meninges exposed • AFP = ELEVATED • AChE = ELEVATED (in amniotic fluid) • Require surgical intervention MEMORY AID BOX at bottom (purple): "Layers Lost as Severity Increases: Occulta: All layers intact (just bone gap) Meningocele: Meninges lost (herniated) Myelomeningocele: Meninges + Cord lost (herniated) Myeloschisis: Everything lost (fully exposed)" Clean white background, color-coded rows by severity, bold text, medical school infographic style.
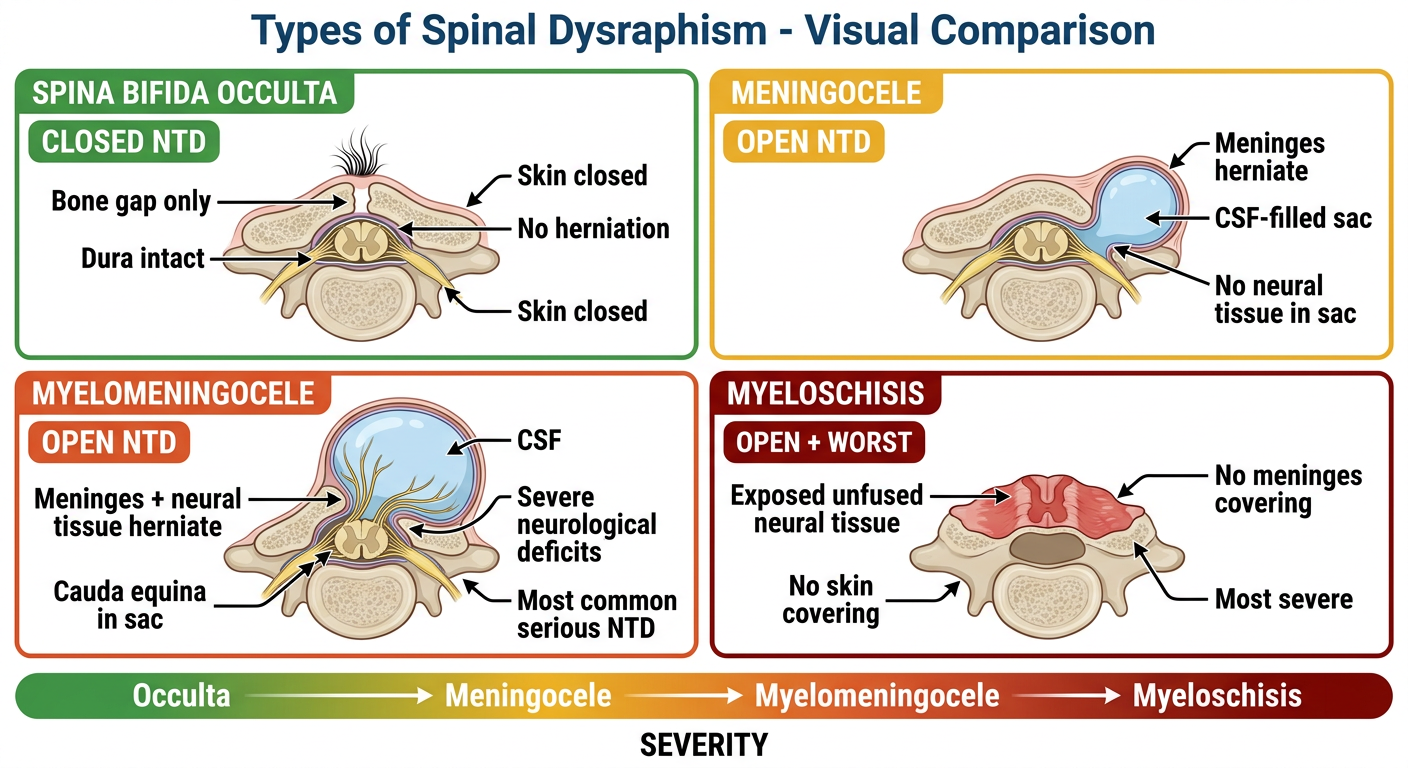
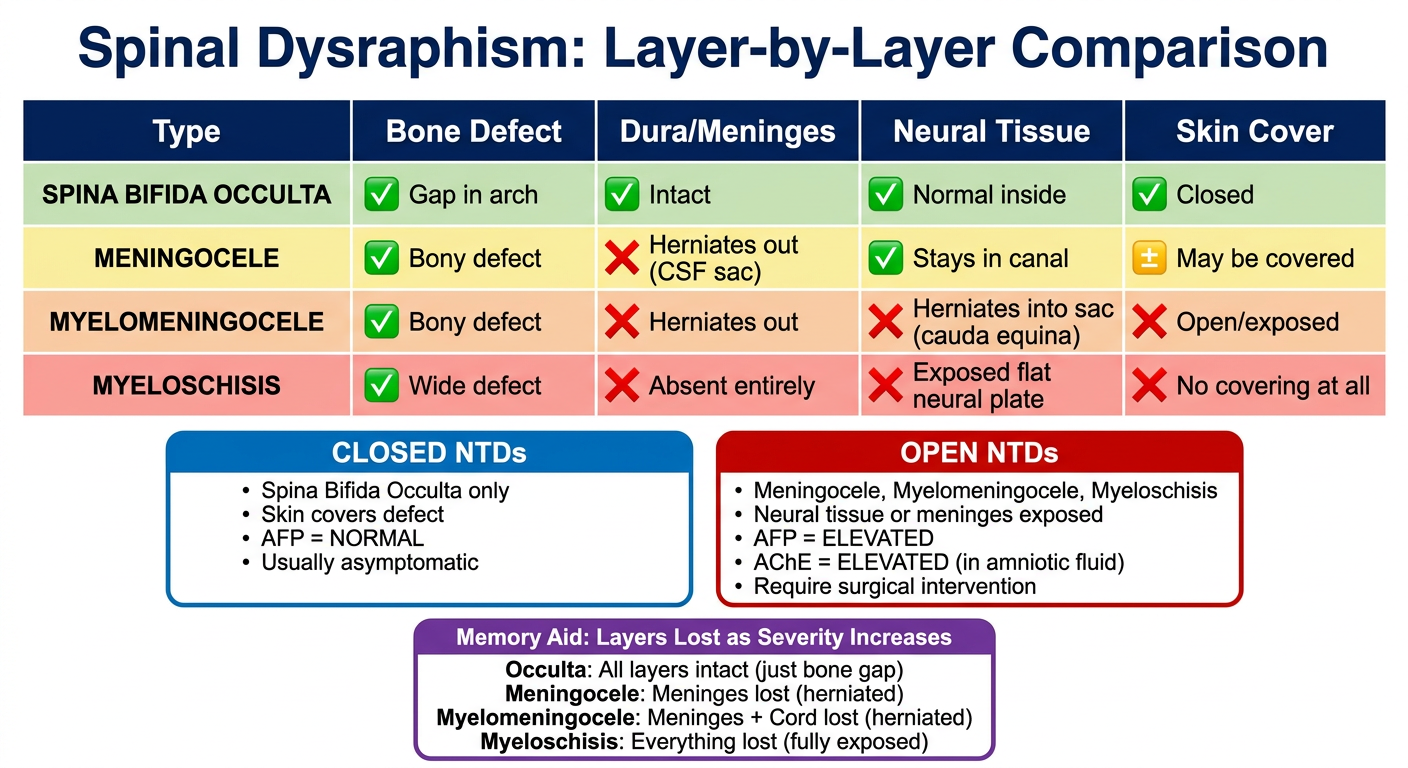
| Type | Open/Closed | Meninges | Neural Tissue | Skin | AFP |
|---|---|---|---|---|---|
| Occulta | Closed | Intact | In canal | Intact + hair/dimple | Normal |
| Meningocele | Open | Herniated (CSF sac) | In canal | May cover sac | Elevated |
| Myelomening. | Open | Herniated | Herniated (cauda equina) | Exposed | Elevated |
| Myeloschisis | Open | Absent | Fully exposed flat plate | None | Elevated |
Occulta → Bone only affected. All soft tissues intact.
Meningocele → Bone + Meninges herniate. Cord safe.
Myelomeningocele → Bone + Meninges + Cord all herniate.
Myeloschisis → Bone + Meninges + Cord all gone. Raw plate.
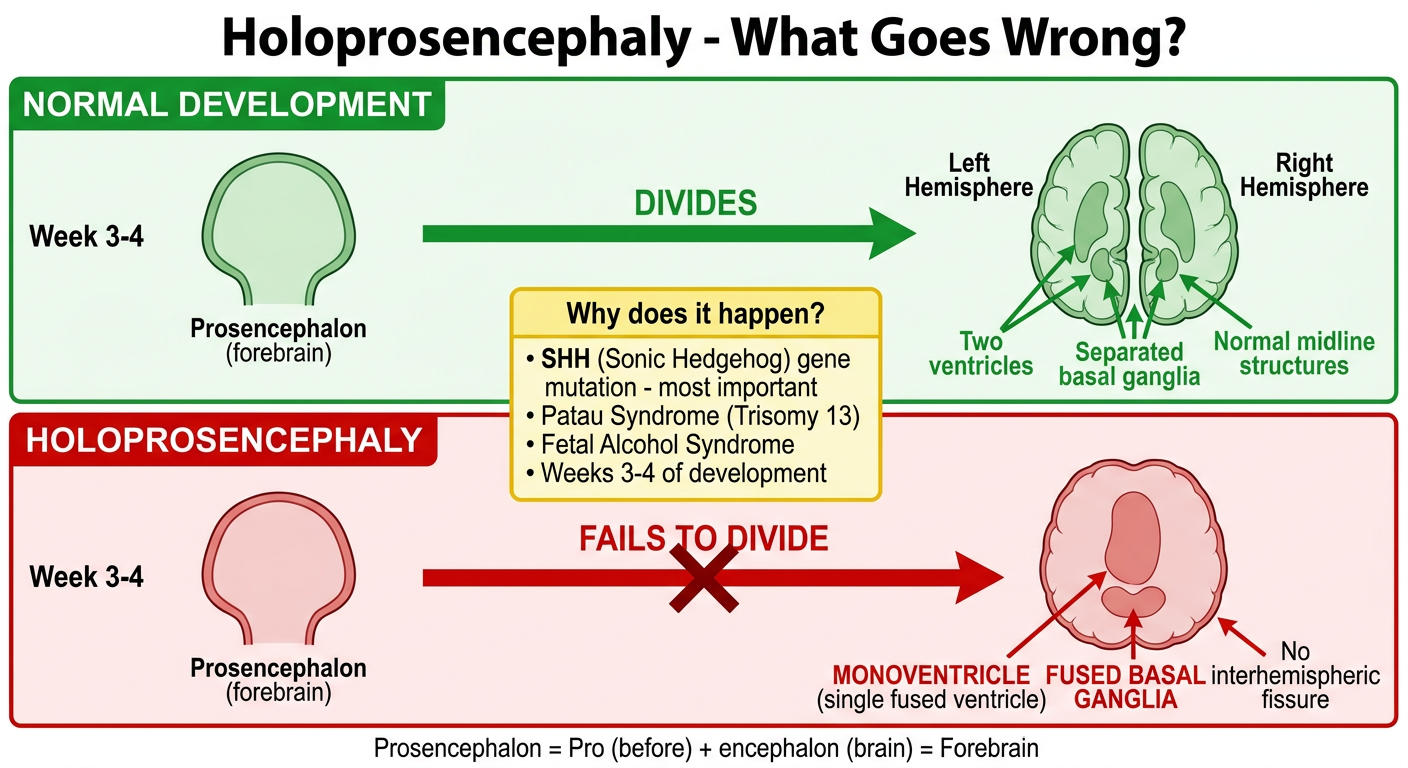
Brain Malformations Brain malformations often result in conditions incompatible with postnatal life, and survivors may be profoundly disabled. Holoprosencephaly: A failure of the forebrain (prosencephalon) to divide into two cerebral hemispheres, typicaly occurring at weeks 3-4 of development. It is associated with SHH mutations and may be seen in Patau syndrome (trisomy 13) and fetal alcohol syndrome. Clinical features include midline defects such as a monoventricle, fused basal ganglia, cleft lip/palate, hypotelorism, cyclopia, and proboscis. There is an increased risk for pituitary dysfunction, such as diabetes insipidus. Same make images to make concept visual better like visual diagram how it made
A medical embryology diagram titled "Holoprosencephaly - What Goes Wrong?" showing a clear visual comparison: TOP SECTION - "NORMAL DEVELOPMENT" (green theme): Left to right flow with simple brain illustrations: Week 3-4: "Prosencephalon (forebrain)" - single vesicle → Arrow labeled "DIVIDES" → Two separate cerebral hemispheres drawn from above (left hemisphere + right hemisphere clearly separated by midline fissure) → Labels: "Two ventricles", "Separated basal ganglia", "Normal midline structures" BOTTOM SECTION - "HOLOPROSENCEPHALY" (red theme): Week 3-4: "Prosencephalon (forebrain)" - single vesicle → Arrow labeled "FAILS TO DIVIDE" with red X over it → Single fused brain drawn from above (no midline separation, smooth surface) → Labels: "MONOVENTRICLE (single fused ventricle)", "FUSED BASAL GANGLIA", "No interhemispheric fissure" MIDDLE CAUSES BOX (yellow): Title: "Why does it happen?" • SHH (Sonic Hedgehog) gene mutation - most important • Patau Syndrome (Trisomy 13) • Fetal Alcohol Syndrome • Weeks 3-4 of development BOTTOM NOTE: "Prosencephalon = Pro (before) + encephalon (brain) = Forebrain" Clean white background, simple brain outlines drawn from top view, bold arrows, color-coded normal vs abnormal, medical education style.
A detailed medical clinical features infographic titled "Holoprosencephaly - Clinical Features Mind Map" with a central hub and radiating branches: CENTER HUB (dark red circle): "HOLOPROSENCEPHALY" with subtitle "Forebrain fails to divide - Weeks 3-4" SIX radiating branches with colored boxes: BRANCH 1 (blue, top-left) - "BRAIN FINDINGS": • Monoventricle (single fused ventricle) • Fused basal ganglia • No interhemispheric fissure • Alobar (most severe) / Semilobar / Lobar types BRANCH 2 (red, top-right) - "FACIAL MIDLINE DEFECTS": Show small face illustration with: • Cyclopia (single eye or fused orbits) - draw one eye in center • Proboscis (tube-like nose above eye) • Hypotelorism (eyes too close together) • Cleft lip and/or palate BRANCH 3 (orange, right) - "ASSOCIATED CONDITIONS": • Patau Syndrome (Trisomy 13) - most associated • Fetal Alcohol Syndrome • SHH gene mutations • Edwards syndrome (Trisomy 18) - less common BRANCH 4 (purple, bottom-right) - "ENDOCRINE COMPLICATIONS": • Pituitary dysfunction • Diabetes Insipidus (ADH deficiency) • Growth hormone deficiency • Reason: midline pituitary affected BRANCH 5 (green, bottom-left) - "PROGNOSIS": • Often incompatible with life (severe forms) • Survivors profoundly disabled • Alobar = worst prognosis • Lobar = mildest, may survive longer BRANCH 6 (yellow, left) - "KEY MECHANISM": • SHH normally induces midline separation • SHH mutation = no signal to divide • Compare: SHH also induces Basal plate (motor) MEMORY TIP BOX at bottom (purple): "HOLO = WHOLE (Greek) - the whole forebrain stays as one unit, never dividing into two" "Trisomy 13 = Patau = Holoprosencephaly + Cyclopia + Polydactyly" Clean white background, mind map style, color-coded branches, bold text, clear labels, medical school infographic.
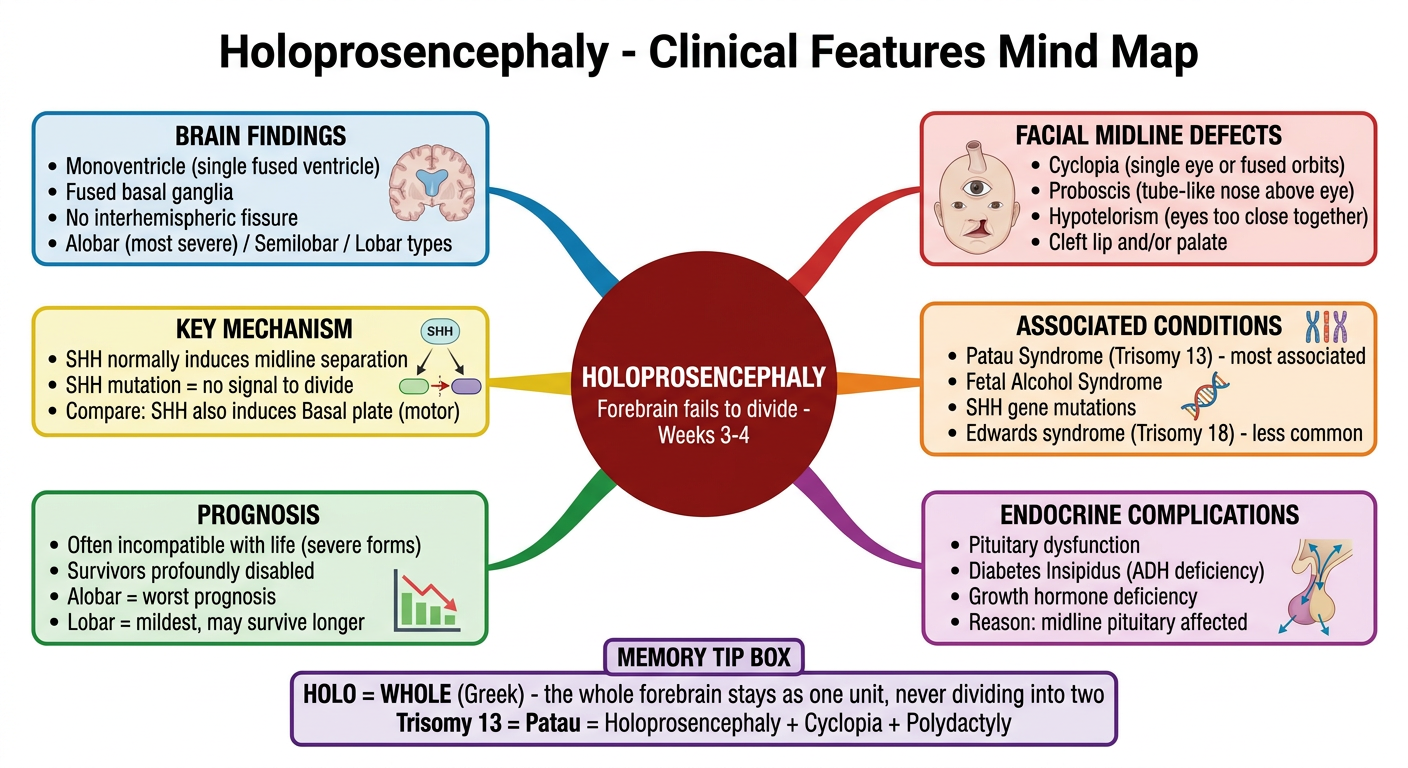
| Feature | Detail |
|---|---|
| What fails | Prosencephalon (forebrain) doesn't split into 2 hemispheres |
| When | Weeks 3-4 of development |
| Cause | SHH mutation, Trisomy 13 (Patau), Fetal Alcohol Syndrome |
| Brain | Monoventricle, fused basal ganglia, no midline fissure |
| Face | Cyclopia, proboscis, hypotelorism, cleft lip/palate |
| Endocrine | Pituitary dysfunction → Diabetes Insipidus |
| Prognosis | Often fatal; survivors severely disabled |
SHH normally signals midline structures to form/divide
→ In neural tube: SHH induces BASAL PLATE (motor, ventral)
→ In forebrain: SHH induces hemisphere DIVISION
→ SHH mutation = Holoprosencephaly (forebrain stays fused)
- Holoprosencephaly (brain)
- Cyclopia / midline face defects
- Polydactyly (extra digits)
Brain Malformations Brain malformations often result in conditions incompatible with postnatal life, and survivors may be profoundly disabled. Holoprosencephaly: A failure of the forebrain (prosencephalon) to divide into two cerebral hemispheres, typicaly occurring at weeks 3-4 of development. It is associated with SHH mutations and may be seen in Patau syndrome (trisomy 13) and fetal alcohol syndrome. Clinical features include midline defects such as a monoventricle, fused basal ganglia, cleft lip/palate, hypotelorism, cyclopia, and proboscis. There is an increased risk for pituitary dysfunction, such as diabetes insipidus. Same make images to make concept visual better like visual diagram how it made
- ✅ How it forms - normal prosencephalon division vs failed division (Image 1)
- ✅ All clinical features - cyclopia, proboscis, monoventricle, fused basal ganglia, cleft lip/palate, hypotelorism, pituitary dysfunction (Image 2)
- ✅ Causes - SHH mutation, Trisomy 13 (Patau), Fetal Alcohol Syndrome
- ✅ Memory tips - "HOLO = WHOLE brain stays as one"
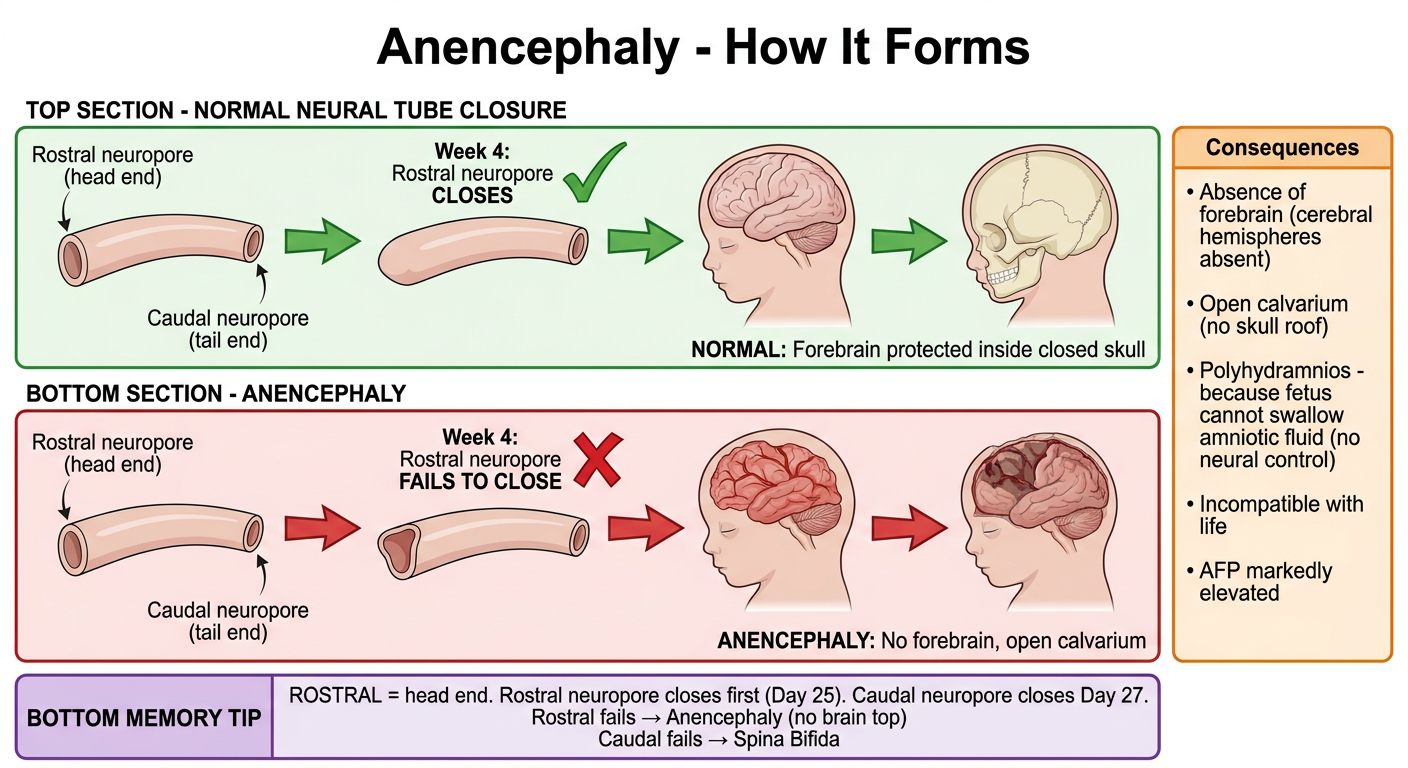
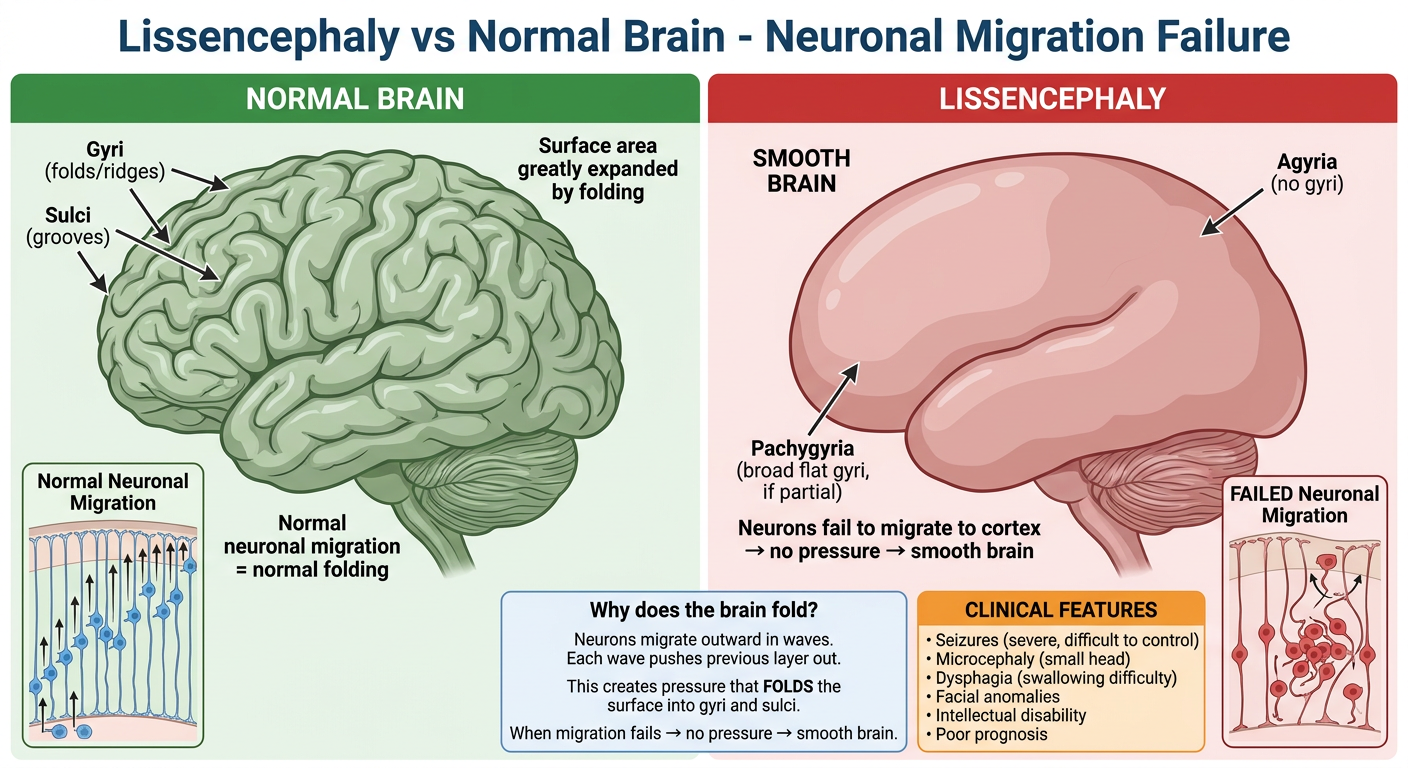
Anencephaly: An open NTD resulting from the failure of the rostral neuropore to close, leading to the absence of the forebrain and an open calvarium. It often presents with polyhydramnios due to fetal swallowing issues from lack of neural control. Lissencephaly: A failure of neuronal migration resulting in a smooth brain Surface that lacks sulci and gyri. It presents with dysphagia, seizures, microcephaly, and facial anomalies. Same make images to make concept visual better like visual diagram how tit made
A medical embryology diagram titled "Anencephaly - How It Forms" showing a clear step-by-step process: TOP SECTION - NORMAL NEURAL TUBE CLOSURE (green): Sequential diagram left to right: Step 1: Neural tube with TWO open ends labeled "Rostral neuropore (head end)" and "Caudal neuropore (tail end)" Step 2: Arrow showing "Week 4: Rostral neuropore CLOSES" with green checkmark Step 3: Normal brain develops - show brain outline with forebrain, cerebellum visible Step 4: Normal skull (calvarium) forms around brain Label: "NORMAL: Forebrain protected inside closed skull" BOTTOM SECTION - ANENCEPHALY (red): Step 1: Same neural tube with two open ends Step 2: Arrow showing "Week 4: Rostral neuropore FAILS TO CLOSE" with large red X Step 3: Forebrain tissue is exposed and degenerates - show brain with top half missing/absent Step 4: Open skull - calvarium absent (draw skull with open top, no roof) Label: "ANENCEPHALY: No forebrain, open calvarium" SIDE BOX (orange) - "Consequences": • Absence of forebrain (cerebral hemispheres absent) • Open calvarium (no skull roof) • Polyhydramnios - because fetus cannot swallow amniotic fluid (no neural control) • Incompatible with life • AFP markedly elevated BOTTOM MEMORY TIP (purple): "ROSTRAL = head end. Rostral neuropore closes first (Day 25). Caudal neuropore closes Day 27. Rostral fails → Anencephaly (no brain top) Caudal fails → Spina Bifida" Clean white background, sequential arrows, anatomical side-view head illustrations, color-coded, medical education style.
A detailed medical comparison diagram titled "Lissencephaly vs Normal Brain - Neuronal Migration Failure" LEFT PANEL - "NORMAL BRAIN" (green theme): Large illustration of a normal brain from the side (lateral view) showing: - Numerous deep SULCI (grooves/valleys) drawn clearly - Prominent GYRI (ridges/bumps) between the sulci - Labeled: "Sulci (grooves)" with arrows - Labeled: "Gyri (folds/ridges)" with arrows - Label: "Surface area greatly expanded by folding" - Label: "Normal neuronal migration = normal folding" - Small inset showing neuron migration: neurons climbing up radial glia fibers in organized layers RIGHT PANEL - "LISSENCEPHALY" (red theme): Large illustration of lissencephalic brain from same side view showing: - SMOOTH surface with NO sulci or gyri - Brain looks like a smooth oval/egg - Labeled: "Agyria (no gyri)" - Labeled: "Pachygyria (broad flat gyri, if partial)" - Labeled: "SMOOTH BRAIN" - Small inset showing FAILED migration: neurons stuck, not reaching cortex, disorganized layers - Label: "Neurons fail to migrate to cortex → no folding signal" BOTTOM COMPARISON BOX: Title: "Why does the brain fold?" "Neurons migrate outward in waves. Each wave pushes previous layer out. This creates pressure that FOLDS the surface into gyri and sulci. When migration fails → no pressure → smooth brain." CLINICAL FEATURES BOX (orange, bottom right): Lissencephaly symptoms: • Seizures (severe, difficult to control) • Microcephaly (small head) • Dysphagia (swallowing difficulty) • Facial anomalies • Intellectual disability • Poor prognosis Clean white background, large clear brain illustrations, labeled anatomy, bold text, medical school infographic style.
A clean medical study comparison infographic titled "Brain Malformations - Anencephaly vs Lissencephaly" structured as a detailed side-by-side comparison: TITLE BAR (dark navy): "Brain Malformations at a Glance" TWO LARGE COLUMNS: LEFT COLUMN (red theme) - "ANENCEPHALY": Header box: "ANENCEPHALY" in bold red Category rows: 🔴 TYPE: Open Neural Tube Defect (NTD) 🔴 CAUSE: Rostral neuropore fails to close - Week 4 🔴 DEFECT: Absence of forebrain + Open calvarium (no skull roof) 🔴 MECHANISM: Rostral neuropore → closes Day 25 normally. Failure = brain exposed, degenerates 🔴 UNIQUE SIGN: Polyhydramnios (fetus can't swallow - no neural control of swallowing) 🔴 AFP: Markedly ELEVATED (open defect) 🔴 PROGNOSIS: Incompatible with life - lethal 🔴 ASSOCIATED: Folate deficiency, teratogens RIGHT COLUMN (blue theme) - "LISSENCEPHALY": Header box: "LISSENCEPHALY" in bold blue Category rows: 🔵 TYPE: Neuronal Migration Defect (NOT an NTD) 🔵 CAUSE: Failure of neuronal migration to cortex 🔵 DEFECT: Smooth brain - absent/reduced sulci and gyri (agyria/pachygyria) 🔵 MECHANISM: Neurons fail to migrate outward in waves → no cortical folding 🔵 UNIQUE SIGN: "Smooth brain" on MRI - agyria 🔵 AFP: Normal (not an open NTD) 🔵 PROGNOSIS: Survivors profoundly disabled 🔵 ASSOCIATED: LIS1 gene mutation, CMV infection, Miller-Dieker syndrome BOTTOM BOX (green): KEY DISTINCTION "Anencephaly = CLOSURE failure (NTD, week 4, open) Lissencephaly = MIGRATION failure (NOT NTD, neurons don't travel properly)" Clean white background, two-column format, bold labels, color-coded, easy to compare, medical exam study style.
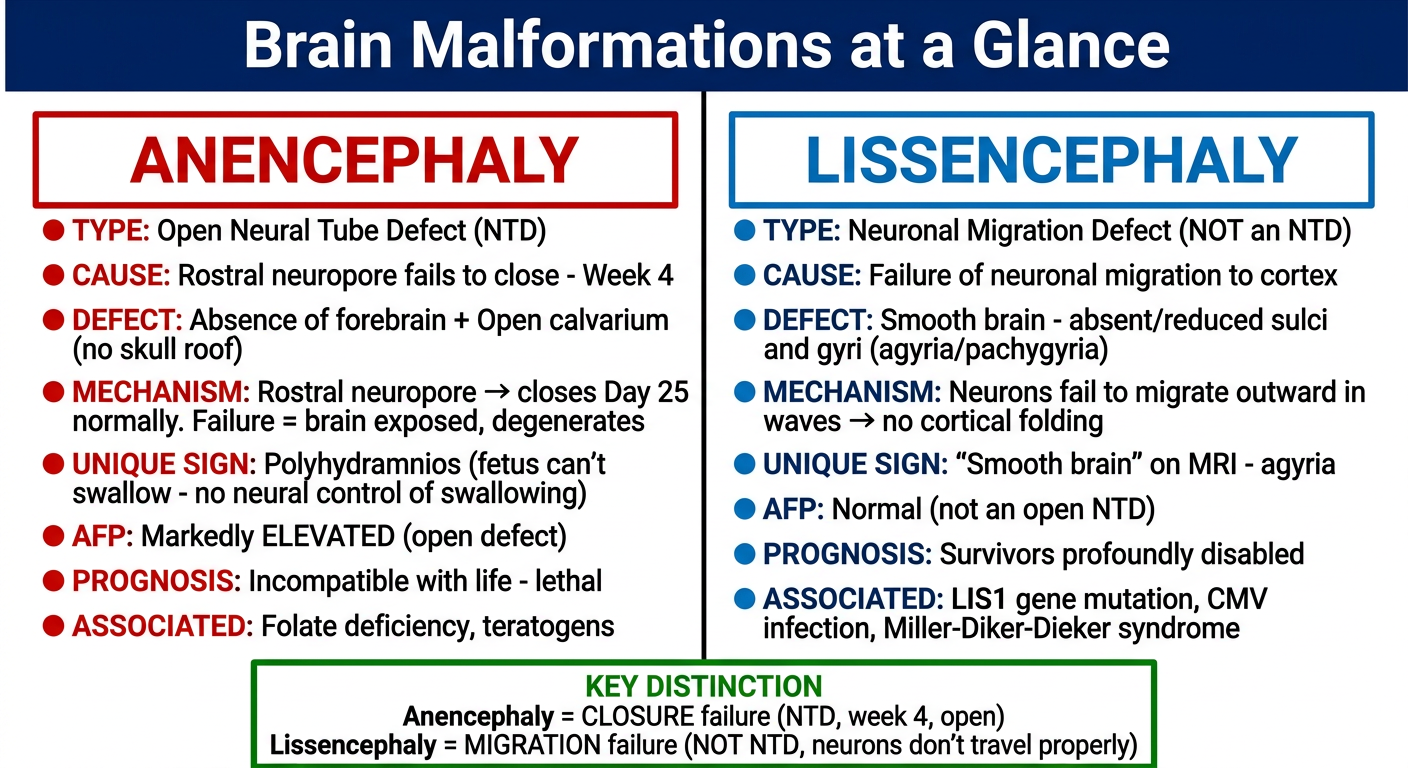
| Anencephaly | Lissencephaly | |
|---|---|---|
| Failure type | Neural tube CLOSURE | Neuronal MIGRATION |
| When | Week 4 | Later (weeks 12-24) |
| Neuropore | Rostral fails (Day 25) | Not a neuropore issue |
| Brain look | Absent forebrain, open skull | Smooth, no gyri/sulci |
| AFP | Markedly elevated | Normal |
| Unique sign | Polyhydramnios | Smooth brain on MRI |
| Prognosis | Fatal (incompatible with life) | Severely disabled |
Rostral neuropore → closes Day 25
Fails → ANENCEPHALY (top of brain gone)
Caudal neuropore → closes Day 27
Fails → SPINA BIFIDA (bottom of spine open)
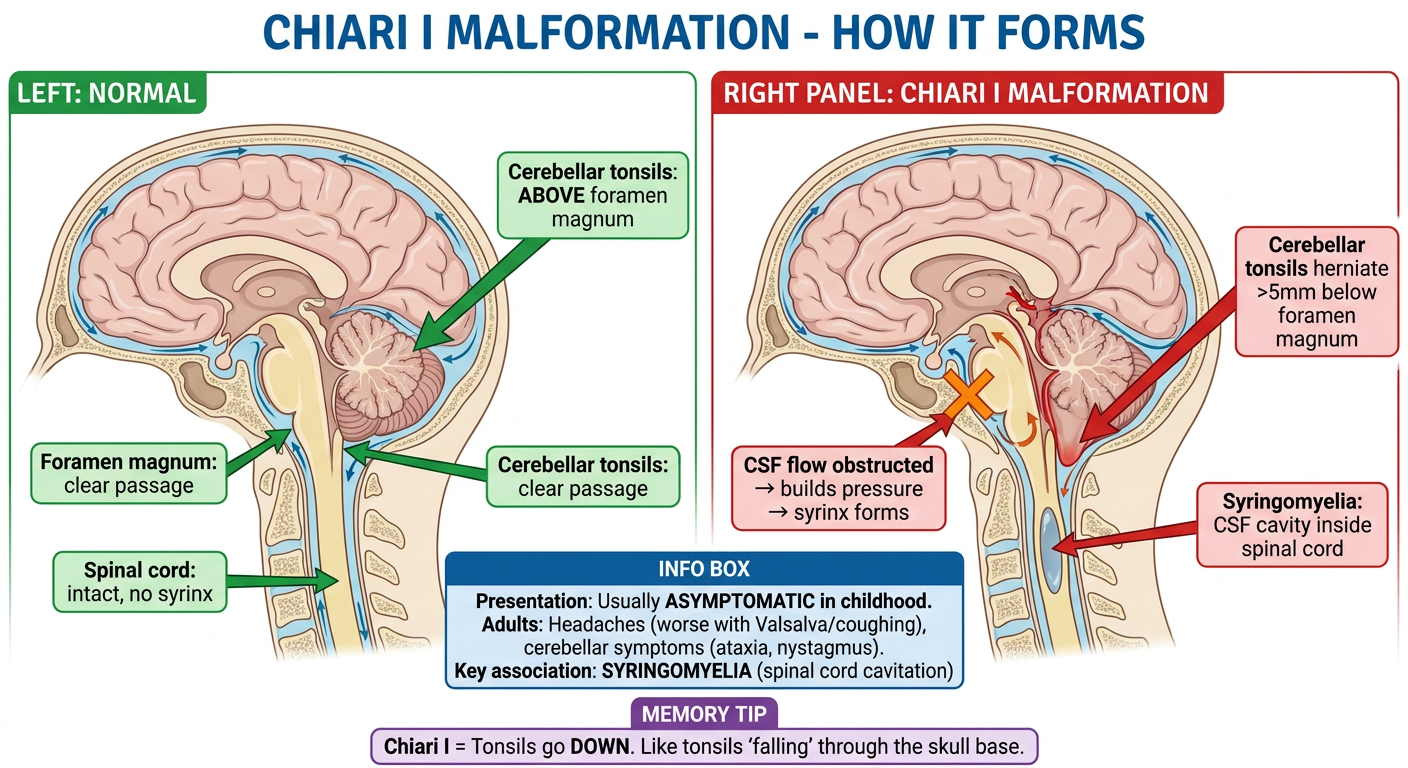
Syrinx Posterior Fossa Malformations Posterior fossa mnalformations include Chiari l and Il malformations and Dandy- Walker malformation. These conditions involve structural abnormalities in the brain, particularly affecting the cerebellum and Surrounding areas. Chiari I Malformation Chiari I malformation is characterized by the downward displacement of the cerebellar tonsils through the foramen magnum. It is usually asymptomatic in childhood but can manifest in adulthood with headaches and cerebelar symptoms. This condition is often associated with spinal cord cavitations, such as syringomyelia. Same make images to make concept visual baetter like visual diagram how it made
A detailed medical anatomy diagram titled "Chiari I Malformation - How It Forms" showing a sagittal (side cross-section) view of the brain and upper spinal cord: LEFT PANEL - "NORMAL" (green theme): Sagittal brain cross-section showing: - Cerebellum sitting normally ABOVE the foramen magnum - Cerebellar tonsils clearly labeled, sitting inside the posterior fossa - Foramen magnum labeled as a clear opening at skull base - Brainstem (medulla) passing cleanly through foramen magnum - Spinal cord below, normal and solid (no cavity) - Label: "Cerebellar tonsils: ABOVE foramen magnum" - Label: "Foramen magnum: clear passage" - Label: "Spinal cord: intact, no syrinx" RIGHT PANEL - "CHIARI I MALFORMATION" (red theme): Same sagittal view showing: - Cerebellar tonsils HERNIATED DOWNWARD through the foramen magnum (draw them pointing down like a cone through the opening) - Red arrow showing downward displacement - Label: "Cerebellar tonsils herniate >5mm below foramen magnum" - Foramen magnum crowded/compressed - CSF flow blocked at foramen magnum level (show blockage with orange X) - Below in spinal cord: a fluid-filled cavity (syrinx) shown as a central oval cavity inside the cord - Label: "Syringomyelia: CSF cavity inside spinal cord" - Label: "CSF flow obstructed → builds pressure → syrinx forms" BOTTOM INFO BOX (blue): "Presentation: Usually ASYMPTOMATIC in childhood Adults: Headaches (worse with Valsalva/coughing), cerebellar symptoms (ataxia, nystagmus) Key association: SYRINGOMYELIA (spinal cord cavitation)" MEMORY TIP (purple): "Chiari I = Tonsils go DOWN. Like tonsils 'falling' through the skull base." Clean white background, anatomically accurate sagittal brain views, bold arrows, color-coded, medical textbook style.
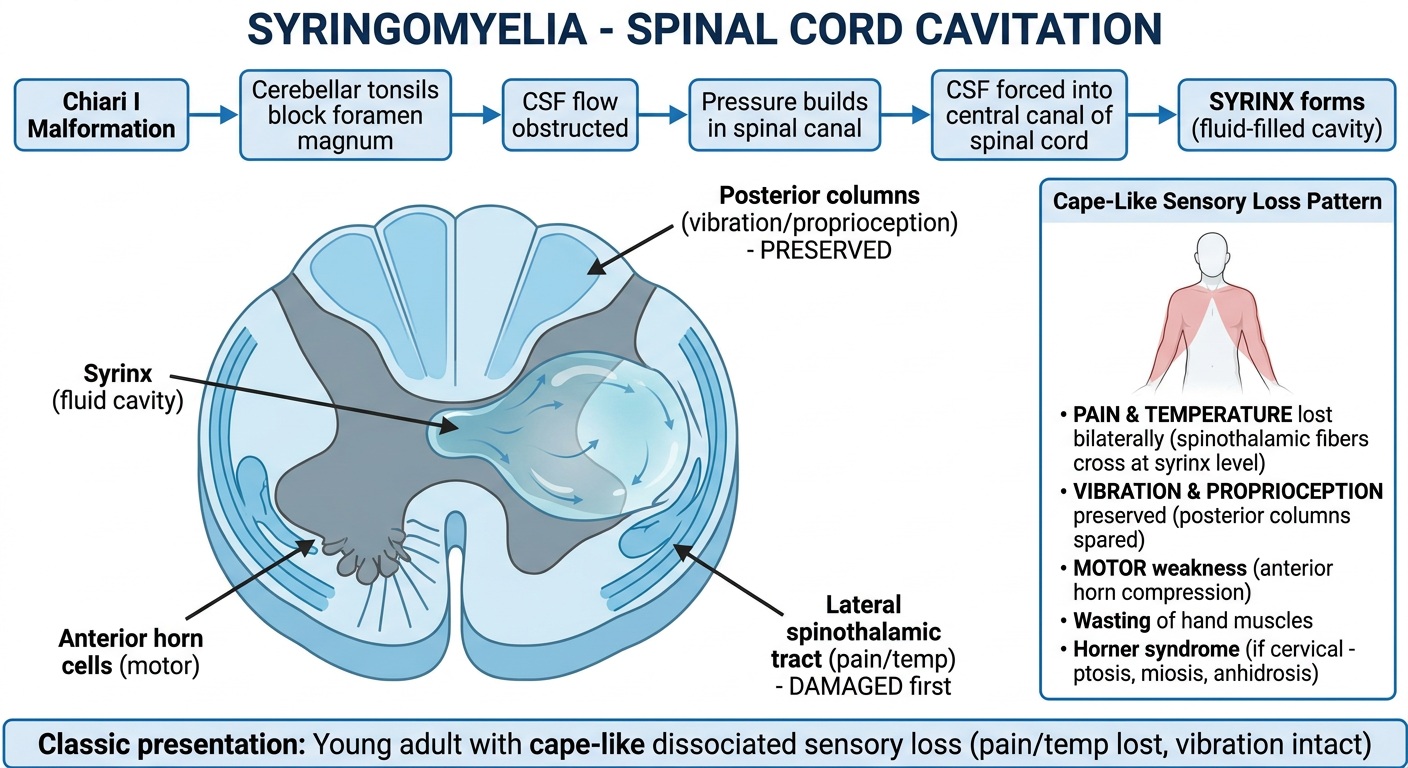
A detailed medical anatomy diagram titled "Syringomyelia - Spinal Cord Cavitation" showing: TOP SECTION - MECHANISM (blue flow diagram): "Chiari I Malformation" → "Cerebellar tonsils block foramen magnum" → "CSF flow obstructed" → "Pressure builds in spinal canal" → "CSF forced into central canal of spinal cord" → "SYRINX forms (fluid-filled cavity)" CENTER - LARGE CROSS-SECTION of spinal cord at cervical level: Show a transverse (axial) cross-section of the spinal cord with: - Outer white matter ring - Inner grey matter in butterfly/H shape - CENTRAL CAVITY (syrinx) shown as a large fluid-filled space in the CENTER, expanding outward - The syrinx expanding and compressing surrounding structures ANATOMICAL LABELS on the cross-section: - "Syrinx (fluid cavity)" - pointing to central cavity - "Anterior horn cells (motor)" - pointing to ventral grey - "Posterior columns (vibration/proprioception) - PRESERVED" - pointing to dorsal white - "Lateral spinothalamic tract (pain/temp) - DAMAGED first" - pointing to lateral area SYMPTOMS BOX (right side): Title: "Cape-Like Sensory Loss Pattern" Show small body outline with shaded area across shoulders/upper arms like a cape Labels: • PAIN & TEMPERATURE lost bilaterally (spinothalamic fibers cross at syrinx level) • VIBRATION & PROPRIOCEPTION preserved (posterior columns spared) • MOTOR weakness (anterior horn compression) • Wasting of hand muscles • Horner syndrome (if cervical - ptosis, miosis, anhidrosis) BOTTOM NOTE: "Classic presentation: Young adult with cape-like dissociated sensory loss (pain/temp lost, vibration intact)" Clean white background, detailed spinal cord cross-section, color-coded tracts, clinical correlation, medical education style.
A clean medical study infographic titled "Posterior Fossa Malformations - Overview & Comparison" comparing three conditions in a structured table/card layout: TITLE BAR (dark navy): "Posterior Fossa Malformations" Subtitle: "Chiari I, Chiari II, Dandy-Walker" THREE CARDS side by side: CARD 1 (blue) - "CHIARI I": Icon: Brain with tonsils pointing down through skull base Key facts: • Cerebellar TONSILS herniate through foramen magnum (>5mm) • Acquired or congenital • Asymptomatic in childhood • Adults: headaches, cerebellar signs • SYRINGOMYELIA common association • No spina bifida association • Treatment: surgical decompression CARD 2 (orange) - "CHIARI II": Icon: Brain with larger herniation + spine defect Key facts: • Cerebellar VERMIS + brainstem herniate through foramen magnum • More severe herniation than Chiari I • ALWAYS associated with Myelomeningocele (spina bifida) • Presents in INFANCY (not adulthood) • Hydrocephalus common • Aqueductal stenosis • Treatment: repair myelomeningocele + shunt CARD 3 (green) - "DANDY-WALKER": Icon: Large posterior fossa with cystic space Key facts: • Cerebellar vermis ABSENT or hypoplastic • Large CYSTIC dilation of 4th ventricle • Posterior fossa enlarged • Hydrocephalus (CSF cannot drain) • Corpus callosum agenesis possible • Intellectual disability • Treatment: VP shunt for hydrocephalus COMPARISON TABLE at bottom: 4 rows: Herniation type | Spina bifida link | Syrinx | Onset Values filled for each of 3 conditions MEMORY TIP (purple box): "Chiari I = Tonsils only, adult onset, syrinx Chiari II = Vermis + brainstem, always with myelomeningocele, infant Dandy-Walker = No vermis, BIG 4th ventricle cyst" Clean white background, 3 distinct colored cards, bold text, comparison table, medical school study style.
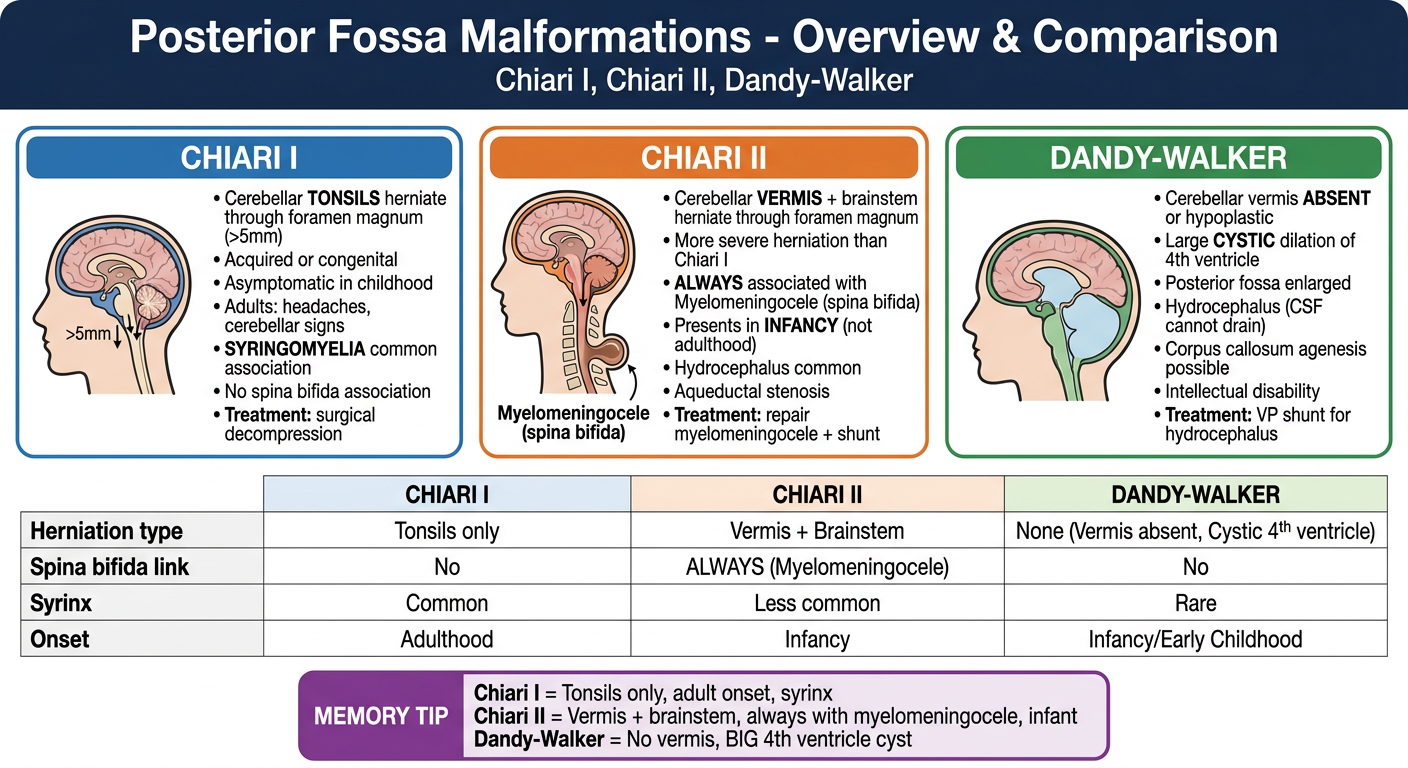
| Feature | Chiari I | Chiari II | Dandy-Walker |
|---|---|---|---|
| What herniates | Cerebellar tonsils | Vermis + brainstem | Nothing herniates - vermis absent |
| Herniation size | >5mm below FM | Large | N/A |
| Spina bifida | No | Always (myelomeningocele) | No |
| Syrinx | Common | Less common | Rare |
| Hydrocephalus | Rare | Common | Always |
| Onset | Adulthood | Infancy | Infancy |
| 4th ventricle | Normal | Compressed | Massively dilated (cyst) |
Syrinx expands from CENTER of cord outward
→ Hits crossing spinothalamic fibers FIRST
→ Pain & temperature lost (bilateral, cape distribution)
→ Posterior columns (vibration/proprioception) SPARED
→ Called: DISSOCIATED sensory loss
- Chiari I = Tonsils, Adults, Syrinx
- Chiari II = Vermis, Infants, Myelomeningocele
- Dandy-Walker = No vermis, Giant 4th ventricle, Hydrocephalus
Syrinx Posterior Fossa Malformations Posterior fossa mnalformations include Chiari l and Il malformations and Dandy- Walker malformation. These conditions involve structural abnormalities in the brain, particularly affecting the cerebellum and Surrounding areas. Chiari I Malformation Chiari I malformation is characterized by the downward displacement of the cerebellar tonsils through the foramen magnum. It is usually asymptomatic in childhood but can manifest in adulthood with headaches and cerebelar symptoms. This condition is often associated with spinal cord cavitations, such as syringomyelia. Same make images to make concept visual baetter like visual diagram how it made
- ✅ Chiari I anatomy - tonsils herniating through foramen magnum, normal vs abnormal (Image 1)
- ✅ Syringomyelia - how the syrinx forms + cape-like sensory loss pattern (Image 2)
- ✅ All 3 posterior fossa malformations - Chiari I, Chiari II, Dandy-Walker compared (Image 3)
Chiari Il Malformation Chiari Il malformation involves the downward displacement of the cerebellum (including the vermis and tonsils) and the medulla through the foramen magnum. It is more severe than Chiari I and typically presents early in life with symptoms such as dysphagia, stridor, apnea, and limb weakness. It is associated with noncommunicating hydrocephalus and myelomeningocele, usually in the lumbosacral region. Dandy-Walker Malformation Dandy-Walker malformation is characterized by the agenesis of the cerebellar vermis, leading to cystic enlargement of the fourth ventricle, which fills the enlarged posterior fossa. It is associated with noncommunicating hydrocephalus and spina bifida. Same make images to make concept visual better like visual diagram how it made
A detailed medical sagittal brain anatomy diagram titled "Chiari II Malformation - What Herniates?" showing side-by-side comparison: LEFT PANEL - "NORMAL" (green): Sagittal brain cross-section: - Cerebellum (vermis + tonsils) sitting fully inside posterior fossa - Medulla sitting above foramen magnum - 4th ventricle normal size - Spinal cord normal below - Labels: "Vermis: inside posterior fossa", "Medulla: above foramen magnum", "4th ventricle: normal" RIGHT PANEL - "CHIARI II" (red): Same sagittal view with dramatic downward herniation: - Cerebellar VERMIS herniated down through foramen magnum (large herniation, draw elongated tissue going down) - Cerebellar TONSILS also herniated - MEDULLA also displaced downward and kinked - Red bold arrows showing downward displacement of ALL structures - Foramen magnum completely crowded - 4th ventricle compressed/distorted - Labels with bold arrows: → "Cerebellar VERMIS herniated" → "Cerebellar TONSILS herniated" → "MEDULLA displaced + kinked" → "Foramen magnum severely crowded" → "More severe than Chiari I" LOWER SPINE inset on right panel: - Show lumbosacral spine with MYELOMENINGOCELE sac - Label: "ALWAYS associated with Myelomeningocele (lumbosacral)" SYMPTOMS BOX (orange, bottom right): "Presents in INFANCY (not adulthood like Chiari I): • Dysphagia (swallowing difficulty) • Stridor (breathing noise) • Apnea (breathing stops) • Limb weakness • Noncommunicating hydrocephalus" MEMORY TIP (purple): "Chiari II = EVERYTHING goes down: vermis + tonsils + medulla. Always paired with myelomeningocele." Clean white background, anatomically accurate sagittal views, bold labels, color-coded, medical textbook style.
A detailed medical anatomy diagram titled "Dandy-Walker Malformation - How It Forms" showing sagittal brain views: LEFT PANEL - "NORMAL DEVELOPMENT" (green): Sagittal brain cross-section showing: - Cerebellar VERMIS fully formed (midline cerebellar structure, clearly labeled) - 4th ventricle normal small size between cerebellum and brainstem - Posterior fossa normal size - CSF flow arrows showing normal drainage through 4th ventricle outlets (foramina of Luschka and Magendie) - Label: "Vermis: fully formed midline cerebellum" - Label: "4th ventricle: normal size" - Label: "Posterior fossa: normal" - Label: "CSF drains normally" RIGHT PANEL - "DANDY-WALKER" (red/orange): Same sagittal view showing: - Cerebellar vermis ABSENT or severely hypoplastic (draw a gap/missing piece where vermis should be) - Huge CYSTIC DILATION of 4th ventricle filling the entire posterior fossa (large blue fluid-filled cyst) - Posterior fossa massively enlarged (torcular-lambdoid inversion) - Cerebellum pushed to the sides (hemispheres present but vermis absent) - CSF CANNOT drain - foramina of Luschka and Magendie obstructed - Hydrocephalus developing (ventricles above enlarged) - Labels: → "Vermis: ABSENT (agenesis)" → "4th ventricle: MASSIVELY dilated cyst" → "Posterior fossa: enlarged" → "CSF outflow BLOCKED" → "Hydrocephalus (noncommunicating)" MECHANISM FLOW (bottom): "Vermis fails to develop" → "4th ventricle has no posterior wall" → "4th ventricle balloons into cyst" → "Posterior fossa expands" → "CSF cannot exit" → "Noncommunicating hydrocephalus" ASSOCIATIONS BOX (blue): • Noncommunicating hydrocephalus • Spina bifida • Corpus callosum agenesis (30%) • Intellectual disability MEMORY TIP (purple): "Dandy-Walker = DANCE floor is empty (no vermis) and the ROOM got huge (4th ventricle cyst)" Clean white background, clear sagittal brain illustrations, bold arrows, color-coded, medical education style.
A comprehensive medical comparison infographic titled "Posterior Fossa Malformations: Chiari I vs Chiari II vs Dandy-Walker" as a detailed structured comparison table: TITLE (dark navy banner): "Posterior Fossa Malformations - Master Comparison" THREE COLUMN LAYOUT with colored headers: Column 1 (blue): CHIARI I Column 2 (orange): CHIARI II Column 3 (green): DANDY-WALKER ROWS comparing each feature: ROW 1 - "What's wrong": Chiari I: Cerebellar tonsils herniate through foramen magnum Chiari II: Vermis + tonsils + medulla ALL herniate through foramen magnum Dandy-Walker: Cerebellar vermis ABSENT, 4th ventricle becomes giant cyst ROW 2 - "How severe": Chiari I: Mild - tonsils only Chiari II: Severe - multiple structures herniate Dandy-Walker: Severe - structural agenesis ROW 3 - "When it presents": Chiari I: Usually ADULTHOOD (headaches, Valsalva) Chiari II: INFANCY (dysphagia, stridor, apnea) Dandy-Walker: INFANCY/childhood (hydrocephalus, developmental delay) ROW 4 - "Key association": Chiari I: SYRINGOMYELIA (spinal cord cavitation) Chiari II: MYELOMENINGOCELE (always, lumbosacral) Dandy-Walker: CORPUS CALLOSUM agenesis (30%) ROW 5 - "Hydrocephalus": Chiari I: Rare Chiari II: Common (noncommunicating) Dandy-Walker: Always (noncommunicating - CSF blocked) ROW 6 - "Spina bifida": Chiari I: No Chiari II: YES - always myelomeningocele Dandy-Walker: Associated (spina bifida) ROW 7 - "Treatment": Chiari I: Surgical decompression of foramen magnum Chiari II: Myelomeningocele repair + VP shunt Dandy-Walker: VP shunt for hydrocephalus BOTTOM MEMORY BOX (purple): "Chiari I = Tonsils fall, adults, syrinx Chiari II = Everything falls, infants, myelomeningocele Dandy-Walker = Vermis gone, 4th ventricle explodes, hydrocephalus" Clean white background, color-coded columns, alternating row shading, bold text, exam-ready comparison style.
400, message: Got more than 4194304 bytes when reading: b'data: {"candidates": [{"content": {"role": "model","parts": [{"inlineData": {"mimeType": "image/png"...'.
We encountered an error while processing your request. Please try again or reach out to us for help.
Chiari Il Malformation Chiari Il malformation involves the downward displacement of the cerebellum (including the vermis and tonsils) and the medulla through the foramen magnum. It is more severe than Chiari I and typically presents early in life with symptoms such as dysphagia, stridor, apnea, and limb weakness. It is associated with noncommunicating hydrocephalus and myelomeningocele, usually in the lumbosacral region. Dandy-Walker Malformation Dandy-Walker malformation is characterized by the agenesis of the cerebellar vermis, leading to cystic enlargement of the fourth ventricle, which fills the enlarged posterior fossa. It is associated with noncommunicating hydrocephalus and spina bifida. Same make images to make concept visual better like visual diagram how it made
An error occurred (ValidationException) when calling the ConverseStream operation: Expected toolResult blocks at messages.66.content for the following Ids: tooluse_tqlp9yi6qGkj38IVRQicyB
We encountered an error while processing your request. Please try again or reach out to us for help.
Chiari Il Malformation Chiari Il malformation involves the downward displacement of the cerebellum (including the vermis and tonsils) and the medulla through the foramen magnum. It is more severe than Chiari I and typically presents early in life with symptoms such as dysphagia, stridor, apnea, and limb weakness. It is associated with noncommunicating hydrocephalus and myelomeningocele, usually in the lumbosacral region. Dandy-Walker Malformation Dandy-Walker malformation is characterized by the agenesis of the cerebellar vermis, leading to cystic enlargement of the fourth ventricle, which fills the enlarged posterior fossa. It is associated with noncommunicating hydrocephalus and spina bifida. Same make images to make concept visual better like visual diagram how it made
An error occurred (ValidationException) when calling the ConverseStream operation: Expected toolResult blocks at messages.66.content for the following Ids: tooluse_tqlp9yi6qGkj38IVRQicyB
We encountered an error while processing your request. Please try again or reach out to us for help.