Articles for soft tissue managements for black triangle
"black triangle" AND "soft tissue" AND gingival embrasure
"open gingival embrasure" AND treatment
interproximal papilla reconstruction AND periodontal
soft tissue management black triangle gingival embrasure treatment review 2023 2024 2025
PMID: 39917646
PMID: 40311633
PMID: 39982591
https://pmc.ncbi.nlm.nih.gov/articles/PMC12271026
PMID: 38198432
PMID: 41582832
PMID: 33110310
PMID: 32472968
Soft Tissue Management of Black Triangles (Open Gingival Embrasures) - Key Articles
Background
Reviews & Overviews
1. Interdental papilla recession and reconstruction of the lost triangle (2024) - BEST STARTING POINT
- Barakat SO | Frontiers in Dental Medicine | PMID: 39917646 | PMC: PMC11797962 (open access)
- Comprehensive narrative review covering etiology, classification, and all treatment modalities: correction of traumatic oral hygiene, restorative interventions, papilla priming, hyaluronic acid (HA) injection, autologous fibroblast injection, orthodontic therapy, and surgical techniques with/without grafts.
- Concludes: no gold standard exists; large-scale RCTs and long-term outcomes data are still lacking.
2. Pink esthetic treatment of gingival recession, black triangle, and gummy smile (2025)
- Frontiers in Dental Medicine | PMC: PMC12271026
- Narrative review linking GBT management within the broader "pink esthetic" framework. Covers gingival phenotype modification (GPM) using sCTG, FGG, and collagen matrix (CM) products. Highlights HA filler as a minimally invasive nonsurgical option. Emphasizes that periodontal health must be controlled first before any esthetic intervention.
3. Factors influencing open gingival embrasures in orthodontic treatment (2025)
- Tian E et al. | Progress in Orthodontics | PMID: 39982591 | PMC: PMC11845328
- Retrospective study of 330 patients; identifies key risk factors: older initial age, longer treatment duration, changes in U1-SN angle, contact point-to-alveolar crest distance. Relevant for prevention during orthodontic planning.
Non-Surgical / Minimally Invasive Approaches
4. Derma Fillers: Ray of Light in Black Triangles (2020)
- Kapoor S, Dudeja A | Contemporary Clinical Dentistry | PMID: 33110310 | PMC: PMC7580754 (open access)
- Pilot study (6 patients): 0.2 mL of 0.2% HA gel injected at baseline, 3 weeks, and 3 months. Significant papillary volume gain and esthetic improvement at 6 months. Supports HA injection as a promising minimally invasive option.
5. Effect of Hyaluronic Acid Filler Injection on the Interdental Papilla in a Mouse Model (2020)
- Kim SB et al. | Int J Environ Res Public Health | PMID: 32660062
- Animal model study confirming histological evidence of papilla reconstruction with HA injection; provides mechanistic support for the clinical use of HA fillers.
6. Comparative Study: L-PRF By-products versus Hyaluronic Acid for Interdental Papillae Regeneration (2026) - MOST RECENT
- Sari R et al. | European Journal of Dentistry | PMID: 40311633
- In vivo rat model comparing L-PRF exudate, concentrated-PRF (C-PRF), combined L-PRF/C-PRF, and HA. C-PRF was superior - enhanced fibroblast activity, vascularization, and epithelialization. Positions platelet-rich fibrin by-products as a potential next step beyond HA in nonsurgical papilla regeneration.
7. Potency of Hyaluronic Acid from Eggshell Membrane for Open Gingival Embrasure Reconstruction (2022)
- Suparwitri S, Alhasyimi AA | Dental Research Journal (Isfahan) | PMID: 36605137
- Histomorphological study evaluating novel HA source (eggshell membrane) for embrasure reconstruction following orthodontic tooth movement.
Surgical Techniques
8. Rebuilding the Interproximal Papilla: The "Tube" Technique (2021)
- Kashani H et al. | Clinical Advances in Periodontics | PMID: 32472968
- Novel surgical approach: a connective tissue graft shaped as a "tube" is inserted into a tunnel created in the interproximal space. Achieves 4-5 mm attachment level gain. Addresses limitations of poor blood supply and inadequate flap thickness inherent to papilla surgery.
9. Novel 3D Tunneling (3DT) Technique for Papilla Reconstruction and Interproximal Attachment Regeneration (2025)
- Kazarian E et al. | Int J Periodontics Restorative Dent | PMID: 38198432
- Case series with 6.5-year follow-up: 18 proximal/midbuccal/midlingual recessions treated simultaneously in anterior mandible. Up to 88.9% mean root coverage in the proximal area. 3D tunneling approach preserves periosteum and vascular supply while allowing simultaneous papilla reconstruction and root coverage.
10. Vertex Technique: A Novel Microsurgical Approach for Papilla Reconstruction (2026) - NEWEST
- Solanes F et al. | Clinical Advances in Periodontics | PMID: 41582832
- Combines microsurgical interproximal tunneling + custom-shaped connective tissue graft + bone graft for PPI 3-4 defects (severe papilla loss) in thick-phenotype patients. Results: PPI improved from 3-4 to 2; stability over 1-5 years. Useful when soft tissue augmentation alone is insufficient due to underlying bone deficiency.
11. "Iceberg" Connective Tissue Graft for Peri-implant Papilla Augmentation (2024)
- Urban IA, Mancini L, Wang HL | Int J Periodontics Restorative Dent | PMID: 37552185
- Describes the "iceberg" CTG technique where a submerged portion of the graft provides volumetric support for interproximal papilla at implant sites following bone reconstruction. Relevant for peri-implant black triangle management.
12. Tunneled Coronally Advanced Flap (verTCAF) for Vertical Soft Tissue Reconstruction (2025)
- Tavelli L et al. | Int J Periodontics Restorative Dent | PMID: 40198777
- Describes the vertical variant of the tunneled coronally advanced flap (verTCAF) specifically for peri-implant papilla augmentation - useful for implant-related black triangles.
Orthodontic Context
13. Incidence and Severity of Open Gingival Embrasures: Clear Aligners vs. Fixed Appliances (2023)
- Yang T et al. | Head & Face Medicine | PMID: 37461116
- Retrospective cohort; compares GBT incidence between clear aligner and fixed appliance patients. Useful for pre-treatment patient counseling on iatrogenic black triangle risk.
14. Occurrence and Risk Factors of Black Triangles After Orthodontic Treatment (2024)
- Jung JS et al. | Diagnostics (Basel) | PMID: 39682655
- Identifies risk factors specific to central incisor region black triangles post-orthodontics: key for prevention protocols.
Treatment Decision Framework (from the literature)
| Severity | Approach |
|---|---|
| Mild (small space, healthy periodontium) | HA filler injection, papilla priming, IPR + restorative |
| Moderate (papilla loss PPI 2-3, bone intact) | Surgical tunneling + CTG (Tube technique, 3DT) |
| Severe (PPI 3-4, bone loss present) | Vertex technique (CTG + bone graft), or staged bone then soft tissue augmentation |
| Peri-implant | Iceberg CTG, verTCAF |
| Orthodontic-related | IPR, root parallelism correction, HA injection post-treatment |
| Emerging (regenerative) | C-PRF injection (superior to HA in animal studies, 2026) |
Generate a comparison poster: surgical vs. nonsurgical black triangle treatments
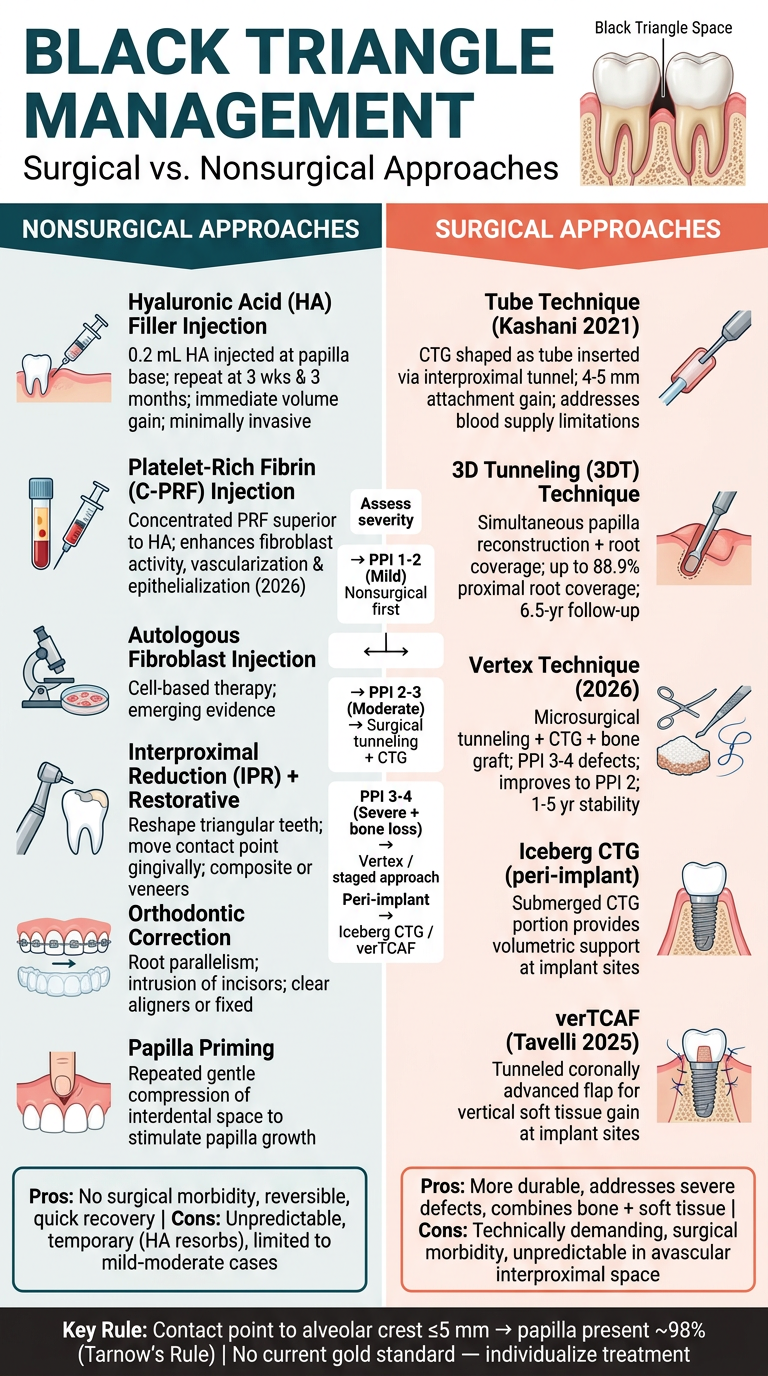
A professional clinical comparison poster titled "Black Triangle Management: Surgical vs. Nonsurgical Approaches" for dental/periodontal use. The poster has a clean two-column layout on a white/light grey background with a dark teal and coral/orange color scheme. TOP HEADER: Large bold title "BLACK TRIANGLE MANAGEMENT" with subtitle "Surgical vs. Nonsurgical Approaches" and a small anatomical illustration of an interdental papilla with a black triangle space visible. LEFT COLUMN (teal/dark green header): "NONSURGICAL APPROACHES" Listed items with icons: 1. Hyaluronic Acid (HA) Filler Injection - "0.2 mL HA injected at papilla base; repeat at 3 wks & 3 months; immediate volume gain; minimally invasive" 2. Platelet-Rich Fibrin (C-PRF) Injection - "Concentrated PRF superior to HA; enhances fibroblast activity, vascularization & epithelialization (2026)" 3. Autologous Fibroblast Injection - "Cell-based therapy; emerging evidence" 4. Interproximal Reduction (IPR) + Restorative - "Reshape triangular teeth; move contact point gingivally; composite or veneers" 5. Orthodontic Correction - "Root parallelism; intrusion of incisors; clear aligners or fixed" 6. Papilla Priming - "Repeated gentle compression of interdental space to stimulate papilla growth" Pros/Cons box for nonsurgical: Pros: No surgical morbidity, reversible, quick recovery | Cons: Unpredictable, temporary (HA resorbs), limited to mild-moderate cases RIGHT COLUMN (coral/orange header): "SURGICAL APPROACHES" Listed items with icons: 1. Tube Technique (Kashani 2021) - "CTG shaped as tube inserted via interproximal tunnel; 4-5 mm attachment gain; addresses blood supply limitations" 2. 3D Tunneling (3DT) Technique - "Simultaneous papilla reconstruction + root coverage; up to 88.9% proximal root coverage; 6.5-yr follow-up" 3. Vertex Technique (2026) - "Microsurgical tunneling + CTG + bone graft; PPI 3-4 defects; improves to PPI 2; 1-5 yr stability" 4. Iceberg CTG (peri-implant) - "Submerged CTG portion provides volumetric support at implant sites" 5. verTCAF (Tavelli 2025) - "Tunneled coronally advanced flap for vertical soft tissue gain at implant sites" Pros/Cons box for surgical: Pros: More durable, addresses severe defects, combines bone + soft tissue | Cons: Technically demanding, surgical morbidity, unpredictable in avascular interproximal space MIDDLE DIVIDER: A simple decision tree/flowchart: "Assess severity" → PPI 1-2 (Mild) → Nonsurgical first → PPI 2-3 (Moderate) → Surgical tunneling + CTG → PPI 3-4 (Severe + bone loss) → Vertex / staged approach → Peri-implant → Iceberg CTG / verTCAF BOTTOM BANNER (dark): "Key Rule: Contact point to alveolar crest ≤5 mm → papilla present ~98% (Tarnow's Rule) | No current gold standard — individualize treatment" Professional medical poster style, well-organized, color-coded, suitable for a dental clinic or conference presentation.