Examination of larynx step wise from dhinghra
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
I now have comprehensive material. Let me compile the full stepwise examination of the larynx as per Dhingra's approach (which aligns precisely with the methods described in these authoritative ENT references).
Examination of the Larynx - Stepwise (Dhingra's ENT)
Note: Dhingra's "Diseases of Ear, Nose and Throat" is not directly available in this library. The following is compiled from authoritative ENT references (Cummings Otolaryngology, Scott-Brown's, KJ Lee's Essential Otolaryngology, Pfenninger & Fowler) that describe the identical stepwise approach outlined in Dhingra.
Anatomy Revision Before Examination
The larynx is divided into three regions:
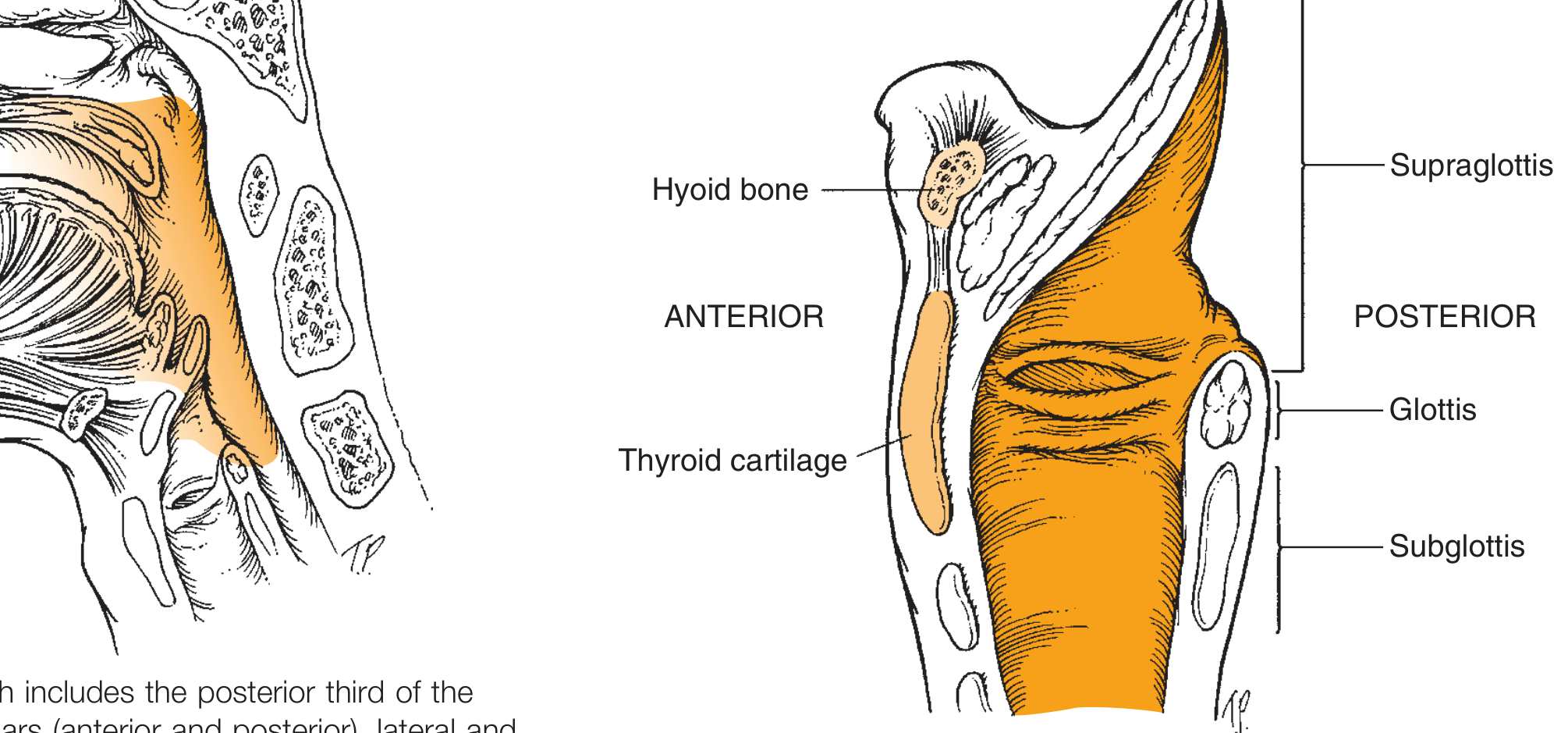
- Supraglottis: epiglottis, aryepiglottic folds, false vocal cords, ventricles
- Glottis: true vocal folds, arytenoids, anterior commissure
- Subglottis: from 5-10 mm below the free edge of the true vocal fold to the inferior margin of the cricoid
STEP 1 - General Inspection
Before any instrumentation:
- Observe the neck - any swelling, asymmetry, surgical scars, or laryngeal crepitus
- Assess the voice quality - hoarseness (dysphonia), breathiness, stridor (inspiratory = supraglottic/glottic, expiratory = subglottic/tracheal, biphasic = fixed lesion)
- Note respiratory pattern - stridor, use of accessory muscles, paradoxical breathing
- Look for dysphagia or odynophagia symptoms suggesting supraglottic pathology
STEP 2 - External Palpation of the Larynx
Palpate the larynx and neck systematically:
- Hyoid bone - most prominent anterior neck structure; note tenderness or fractures
- Thyrohyoid membrane - between hyoid and thyroid cartilage
- Thyroid cartilage - the "Adam's apple," note any crepitus, tenderness, or masses
- Cricothyroid membrane - important landmark for emergency airway access
- Cricoid cartilage ("signet ring") - useful orientation landmark, especially in short/thick necks
- Trachea - assess for midline shift
- Laryngeal crepitus - normally the larynx crunches side-to-side against the cervical spine (cricopharyngeal crepitus); loss suggests postcricoid carcinoma or pathology
- Cervical lymph nodes - levels I-VI for metastatic disease
STEP 3 - Instruments Required
| Instrument | Purpose |
|---|---|
| Head mirror / head lamp | Light source directed into the oral cavity |
| Laryngeal mirror (No. 4 or No. 5) | Indirect visualization |
| Alcohol lamp / spirit lamp | Warming the mirror |
| Gauze swab | Grasping the tongue |
| Tongue depressor | Optional |
| Topical anesthetic (4% xylocaine spray) | For gag reflex suppression |
STEP 4 - Indirect Laryngoscopy (Mirror Examination) - The Classic Method
This is the primary examination technique described in Dhingra.
Patient Positioning
- Patient sits upright in the examination chair
- Legs uncrossed, feet planted flat on the footrest
- Back straight, hips firmly against the chair
- Lean slightly forward from the waist ("military/sniffing position")
- Chin slightly up and forward (not tucked - this closes the larynx)
Examiner Positioning
- Sit facing the patient at the same level
- Head mirror on forehead, light source to patient's right side at ear level
- Focus the reflected light beam into the patient's open mouth
Procedure - Step by Step
Step 4a - Prepare the mirror:
- Warm the laryngeal mirror over an alcohol lamp to just below body temperature
- Test the temperature on the back of your hand or on your own wrist
- The mirror must be warm enough to prevent fogging but not hot enough to burn the mucosa
Step 4b - Tongue retraction:
- Ask the patient to open the mouth wide and protrude the tongue
- Wrap the tongue with a gauze piece for grip
- Grasp the tongue between thumb (below) and index/middle finger (above)
- The examiner's middle finger can retract the upper lip superiorly
- Pull the tongue forward and downward - do NOT pull excessively as this triggers the gag reflex
Step 4c - Mirror placement:
- Hold the warmed mirror in the right hand like a pen
- Introduce the mirror into the oropharynx at an angle
- Rest the back of the mirror against the uvula and soft palate, gently elevating them
- Do NOT touch the posterior tongue base or posterior pharyngeal wall (triggers gag)
- The mirror face is directed downward and forward at approximately 45 degrees
Step 4d - Focus light and observe:
- Direct the reflected head mirror light into the dental mirror
- Ask the patient to breathe quietly through the mouth ("haaaa" phonation opens the larynx)
- Note: the image is reversed (patient's right = examiner's left side in mirror)
STEP 5 - What to Look for on Indirect Laryngoscopy
Examine in a systematic stepwise order from superior to inferior:
A. Tongue Base and Vallecula
- Lingual tonsils, cysts, masses
- Vallecula - pooling of saliva (suggests dysphagia or epiglottis fixity)
B. Epiglottis
- Shape - should be crisp, leaf-shaped (omega or tubular-shaped in children)
- Color - normally pale pink; erythematous + edematous = epiglottitis
- Petiole of epiglottis - normal pointed projection, do not mistake for a cyst
- Lingual surface vs. laryngeal surface
- Any irregular or ulcerated mucosal lesions (carcinoma)
C. Aryepiglottic Folds and Pyriform Fossae
- Note any mucosal irregularity, edema, or masses
- Pyriform sinuses (piriform fossae) - ask patient to "puff the cheeks with mouth closed" to expand them
- Pooling of saliva in pyriform fossae = sign of hypopharyngeal obstruction
- Loss of piriform fossa angle = carcinoma
D. False Vocal Cords (Vestibular Folds)
- Normally pink, smooth bands
- Swelling, hemorrhage, masses
- Paradoxical false cord adduction in dysphonia
E. Laryngeal Ventricles
- Small recesses between false and true vocal cords (hard to see in mirror)
- Ventricular cysts, laryngoceles
F. True Vocal Cords - Most Important
Normally: pearly white, translucent, with crisp free borders
Ask patient to:
- Say "eee" - cords adduct; assess closure, gap, and symmetry
- Pant - rapid abduction/adduction
- High-pitched "eee" - better assessment of cord function
- Deep breath - maximum abduction; check subglottis if possible
Assess:
- Color - white (normal), redness (laryngitis), leukoplakia (white patch), erythroplakia
- Surface - smooth vs. nodules, polyps, papillomas, ulcers
- Edge - straight vs. irregular (carcinoma)
- Mobility:
- Normal: full abduction and adduction
- Paresis: reduced mobility
- Paralysis: fixed cord (note position - paramedian, median, cadaveric)
- Anterior commissure - common site for carcinoma
- Reinke's edema - gelatinous swelling of full cord length (smokers)
G. Arytenoids and Posterior Commissure (Interarytenoid Region)
- Observe arytenoid movement during phonation and breathing
- Redness/edema of interarytenoid mucosa = reflux laryngitis (GERD)
- Arytenoid mucosa erythema - rheumatoid arthritis, post-intubation trauma
- Posterior glottic webs or scars
- Cricoarytenoid joint fixation (immobile arytenoid but normal RLN)
H. Subglottis
- Normally visible during deep inspiration/abduction
- Prominent cricoid seen inferiorly to anterior commissure (normal - do not mistake for subglottic stenosis)
- Any subglottic narrowing, hemangiomas (children), or extension of glottic carcinoma
- Difficult to see in office; CT/MRI or direct laryngoscopy needed for formal assessment
STEP 6 - Additional Maneuvers
| Maneuver | What it reveals |
|---|---|
| Phonation ("eee") | Cord adduction, glottic closure |
| High-pitched "eee" | Subtle cord paresis |
| Panting | Rapid abduction/adduction, arytenoid mobility |
| Puffing cheeks with mouth closed | Distends pyriform sinuses |
| Valsalva | Can reveal laryngoceles and ventricular masses |
| Swallowing | Epiglottis movement, laryngeal elevation |
STEP 7 - Alternative / Supplementary Methods
If indirect laryngoscopy fails (gag reflex, difficult anatomy, children):
| Method | Details |
|---|---|
| Rigid Hopkins rod telescope (70° or 90°) | Trans-oral; excellent optics; best for voice clinic and stroboscopy |
| Flexible fiberoptic nasolaryngoscope (Nasopharyngolaryngoscope) | Trans-nasal; excellent for difficult patients; allows phonation and swallowing assessment; records permanently |
| Chip-tip videoendoscope | High-definition; best for subtle mucosal changes |
| Videostroboscopy | Strobe light added to rigid/flexible scope; evaluates mucosal wave dynamics - distinguishes cysts from nodules, identifies mucosal scarring |
| Direct laryngoscopy (microlaryngoscopy) | Under GA; definitive; allows biopsy |
The stepwise flexible nasolaryngoscopy assessment follows:
- Pass through the anterior nares along the floor of the nose under the inferior turbinate
- Reach postnasal space - ask patient to inspire through the nose (opens nasopharyngeal sphincter)
- Inspect the vallecula (ask patient to protrude the tongue)
- Inspect the supraglottic larynx
- Inspect the glottic larynx
- Assess hypopharynx (pyriform sinuses, postcricoid)
STEP 8 - Normal Findings Summary (What to Report)
A systematic report should note:
- Epiglottis: shape, color, mobility
- AE folds: symmetry, mucosal surface
- False cords: color, size
- True vocal cords: color (pearly white), surface (smooth), edge (crisp), movement (full bilateral adduction/abduction), no lesions
- Arytenoids: mobile, no edema
- Anterior commissure: no lesion
- Posterior commissure: no edema, no inter-arytenoid lesion
- Pyriform sinuses: clear, no pooling
- Subglottis: normal as far as visible
STEP 9 - Causes of Failed Indirect Laryngoscopy
- Excessive gag reflex
- Short, thick neck
- Infantile epiglottis (omega-shaped, obscures view)
- Trismus
- Uncooperative patient
- Management: topical anesthesia (4% xylocaine spray), flexible nasolaryngoscopy, or direct laryngoscopy under GA
Important note: "Failure of indirect laryngoscopy suggests that microlaryngoscopy may also be technically difficult" - Scott-Brown's Otorhinolaryngology
Key Points (Exam-Oriented Summary)
- Image is reversed in indirect laryngoscopy (patient's right = examiner's left)
- Mirror is warmed to prevent fogging but tested on examiner's wrist first
- Patient position: chin up, lean forward (not chin tucked down)
- Tongue is held with gauze - not forcibly pulled
- Do NOT touch posterior tongue base or posterior pharyngeal wall (triggers gag)
- Normal vocal cords are pearly white with crisp translucent borders
- "eee" phonation = cord adduction test; panting/deep breath = abduction test
- Loss of laryngeal crepitus = suggestive of postcricoid carcinoma
- Pooling of saliva in pyriform fossa = sign of obstruction or sensory loss
Sources: Cummings Otolaryngology Head and Neck Surgery; Scott-Brown's Otorhinolaryngology Head & Neck Surgery; K.J. Lee's Essential Otolaryngology; Pfenninger and Fowler's Procedures for Primary Care. This content aligns with the approach described in Dhingra's Diseases of Ear, Nose and Throat.
Ent larynx complain
Asking for Preferences
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
I now have comprehensive material. Here is the full structured answer:
Laryngeal Complaints - Symptoms & Their Causes (ENT)
The larynx produces five cardinal symptoms when diseased. Every laryngeal complaint can be grouped under these five headings:
1. HOARSENESS (Dysphonia)
The most common and most important laryngeal symptom. Defined as any change in voice quality - roughness, breathiness, weakness, or increased effort to speak.
Acute Hoarseness (< 3 weeks)
| Condition | Cause |
|---|---|
| Acute laryngitis | Viral (parainfluenza, influenza, HSV) or bacterial (Moraxella, H. influenzae, Strep pneumoniae) |
| Vocal cord hemorrhage | Sudden vocal abuse/misuse (shouting, screaming) |
| Postnasal drip | Sinusitis, allergies |
| Gastroesophageal reflux (LPR) | Gastric acid irritating posterior larynx |
| Neck/laryngeal trauma | Blunt or penetrating |
| Intubation granuloma | Short or long periods of intubation |
| Conversion disorder / hysterical aphonia | Psychiatric; sudden complete voice loss with normal cords |
Acute hoarseness is rarely malignant. It almost always resolves with conservative management.
Chronic Hoarseness (> 3 weeks - RED FLAG, must scope!)
| Condition | Notes |
|---|---|
| Chronic laryngitis | Smoking, chronic infection, reflux |
| Squamous cell carcinoma | #1 to exclude; progressive, painless, male smoker/alcoholic |
| Vocal cord nodules ("Singer's nodes") | Bilateral, at junction of anterior 1/3 and posterior 2/3; vocal abuse |
| Vocal cord polyp | Usually unilateral; smoking, allergy |
| Recurrent respiratory papillomatosis (RRP) | HPV types 6 & 11; warty lesions; children or adults |
| Vocal cord paralysis | RLN palsy - cancer (thyroid, lung apex, esophagus), trauma, surgical injury, stroke, idiopathic |
| Reinke's edema | Bilateral polypoid degeneration; smokers; low rough voice |
| Leukoplakia / erythroplakia | Pre-malignant; requires biopsy |
| Contact granuloma | Posterior glottis; reflux or intubation |
| Functional dysphonia | No organic lesion; muscle tension dysphonia |
| Spasmodic dysphonia (laryngeal dystonia) | CNS focal dystonia; harsh staccato or breathy voice; resistant to therapy; responds to Botox |
| Systemic: hypothyroidism, amyloidosis, sarcoidosis, RA | Infiltrate or thicken vocal cords |
GRBAS Scale for quantifying hoarseness:
- G - Grade (overall severity)
- R - Roughness
- B - Breathiness
- A - Asthenia (weakness)
- S - Strain
Important rule: Any hoarseness persisting beyond 3 weeks in an adult must have the larynx visualized. Assume malignancy until proven otherwise. - K.J. Lee's Essential Otolaryngology
2. STRIDOR
Noisy breathing from turbulent airflow due to airway obstruction. A symptom, not a diagnosis.
Localization by Phase of Respiration
| Phase | Level of Obstruction | Common Causes |
|---|---|---|
| Inspiratory | At or above the true vocal cords (supraglottic/glottic) | Acute epiglottitis, foreign body, laryngomalacia, croup |
| Expiratory | Below the cords - lower tracheobronchial tree | Asthma, infective tracheobronchitis |
| Biphasic | At the true vocal cords / immediate subglottic level | Subglottic stenosis, bilateral cord palsy, fixed glottic lesion |
Causes by Age Group
Children (more likely congenital/inflammatory):
- Laryngomalacia - most common congenital cause; inspiratory stridor worse with feeding, crying, supine position; resolves by age 2
- Bilateral vocal cord paralysis (birth trauma, Arnold-Chiari)
- Subglottic stenosis (congenital or post-intubation)
- Subglottic hemangioma (worsens with crying)
- Laryngeal web or cleft
- Croup (laryngotracheobronchitis) - most common cause of ACUTE stridor in children; parainfluenza virus; biphasic + barking cough + "steeple sign" on X-ray
- Acute epiglottitis - H. influenzae type b (classic) or Strep; drooling + high fever + "thumbprint sign" + tripod posture; EMERGENCY
- Bacterial tracheitis
- Foreign body inhalation
- Vascular ring (stridor worsens on feeding)
Adults:
- Laryngeal carcinoma
- Bilateral vocal cord paralysis
- Subglottic stenosis (post-intubation, Wegener's granulomatosis)
- Angioneurotic edema / anaphylaxis
- Epiglottitis (adults - increasing incidence)
- Foreign body
Alarm Features in Stridor:
- Cyanosis, severe retractions, confusion, obtundation → imminent airway collapse
- New onset or rapidly worsening stridor → requires urgent ENT/airway management
3. DYSPHAGIA and ODYNOPHAGIA
Swallowing difficulty or pain with swallowing arising from laryngeal/hypopharyngeal pathology.
| Cause | Notes |
|---|---|
| Supraglottic carcinoma | Painless initially; later dysphagia + referred otalgia |
| Epiglottitis | Severe odynophagia + drooling; unable to swallow |
| Arytenoid fixation (cricoarytenoid joint) | RA, trauma, post-intubation |
| Laryngeal trauma | Fracture, hematoma |
| TB laryngitis | Hoarseness + odynophagia + weight loss |
| Hypopharyngeal carcinoma | Piriform sinus carcinoma; progressive dysphagia ± referred otalgia |
| Postcricoid carcinoma | Progressive dysphagia solid → liquids; Plummer-Vinson syndrome predisposition |
| Zenker's diverticulum | Regurgitation of undigested food |
| LPR / GERD | Globus + chronic throat-clearing + dysphagia |
4. COUGH + THROAT SYMPTOMS
| Symptom | Causes |
|---|---|
| Chronic cough | LPR (laryngopharyngeal reflux), vocal cord irritation, laryngeal malignancy, postnasal drip |
| Globus sensation (lump in throat) | LPR/GERD (most common), functional, postcricoid web, pharyngeal pouch, hypopharyngeal tumor |
| Excessive throat clearing | LPR, chronic laryngitis, postnasal drip |
| Hemoptysis | Laryngeal carcinoma, trauma, TB, papilloma - always investigate |
5. RESPIRATORY DISTRESS / APHONIA
| Symptom | Cause |
|---|---|
| Aphonia (complete voice loss) | Bilateral cord palsy, conversion disorder/hysterical, severe laryngitis |
| Acute respiratory distress | Angioedema, epiglottitis, foreign body, bilateral cord palsy, laryngeal fracture |
| Dyspnea on exertion | Laryngeal carcinoma (subglottic extension), stenosis |
Summary: Red Flag Laryngeal Symptoms
| Red Flag | Concern |
|---|---|
| Hoarseness > 3 weeks | Laryngeal carcinoma |
| Hemoptysis + hoarseness | Malignancy until proven otherwise |
| Stridor + drooling + fever (child) | Epiglottitis - EMERGENCY |
| Progressive painless dysphagia | Hypopharyngeal/postcricoid carcinoma |
| Referred otalgia + throat symptom | Carcinoma (via Arnold's nerve reflex) |
| Palpable neck node + hoarseness | Advanced laryngeal/hypopharyngeal malignancy |
| Loss of laryngeal crepitus | Postcricoid carcinoma |
| Pooling of saliva in piriform fossa | Obstruction - carcinoma |
Sources: K.J. Lee's Essential Otolaryngology; Cummings Otolaryngology Head and Neck Surgery; Bailey and Love's Short Practice of Surgery 28th Ed; Textbook of Family Medicine 9e; Rosen's Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.