Explain everything about the esophagus especially the vasculature and lympathic drainage
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Searching Images
esophagus lymphatic drainage nodes
Loading Image
Loading Image
I now have everything needed for a comprehensive, authoritative answer. Let me compile it all.
The Esophagus — Complete Anatomy, Vasculature & Lymphatic Drainage
1. Overview and General Anatomy
The esophagus is a muscular tube, approximately 18–26 cm long, that conducts food from the pharynx to the stomach. It begins at the inferior border of the cricoid cartilage (vertebral level C6) and terminates at the cardiac opening of the stomach (T11). Between swallows the lumen is collapsed, but can distend up to 2 cm anteroposteriorly and 3 cm laterally to accommodate a swallowed bolus.
The esophagus descends anterior to the vertebral bodies in a generally midline position through the thorax. As it approaches the diaphragm, it moves anteriorly and to the left, crossing from the right side of the thoracic aorta to lie anterior to it, and passes through the esophageal hiatus (an opening in the muscular part of the diaphragm) at vertebral level T10.
It has three anatomical segments:
- Cervical esophagus — from C6 to the thoracic inlet (≈5 cm)
- Thoracic esophagus — from thoracic inlet to the diaphragmatic hiatus (≈20 cm)
- Abdominal esophagus — below the diaphragm to the gastroesophageal junction (≈2–3 cm)
2. Relations / Posterior Mediastinum
The esophagus shares the posterior mediastinum with critical structures:
| Direction | Structures |
|---|---|
| Posterior | Thoracic duct (right inferiorly, crosses to left superiorly); hemiazygos veins; right posterior intercostal vessels; thoracic aorta near diaphragm |
| Anterior | Trachea (above carina); right pulmonary artery and left main bronchus (below carina); left atrium (separated only by pericardium) |
| Right | Mediastinal parietal pleura |
| Left | Thoracic aorta |
3. Anatomical Constrictions
The esophagus is compressed or narrowed at four sites — clinically important because swallowed objects lodge here, corrosives cause greater damage here, and these are common sites for carcinoma:
- Pharyngo-esophageal junction — at cricopharyngeus (Killian's mouth), ~15 cm from incisors
- Aortic arch crossing — where the arch crosses from right to left, ~22–23 cm
- Left main bronchus — compression at the tracheal bifurcation, ~27 cm
- Esophageal hiatus — where it passes through the diaphragm, ~38 cm
4. Wall Structure & Histology
The esophageal wall lacks a serosa (unlike the rest of the GI tract). It has four layers:
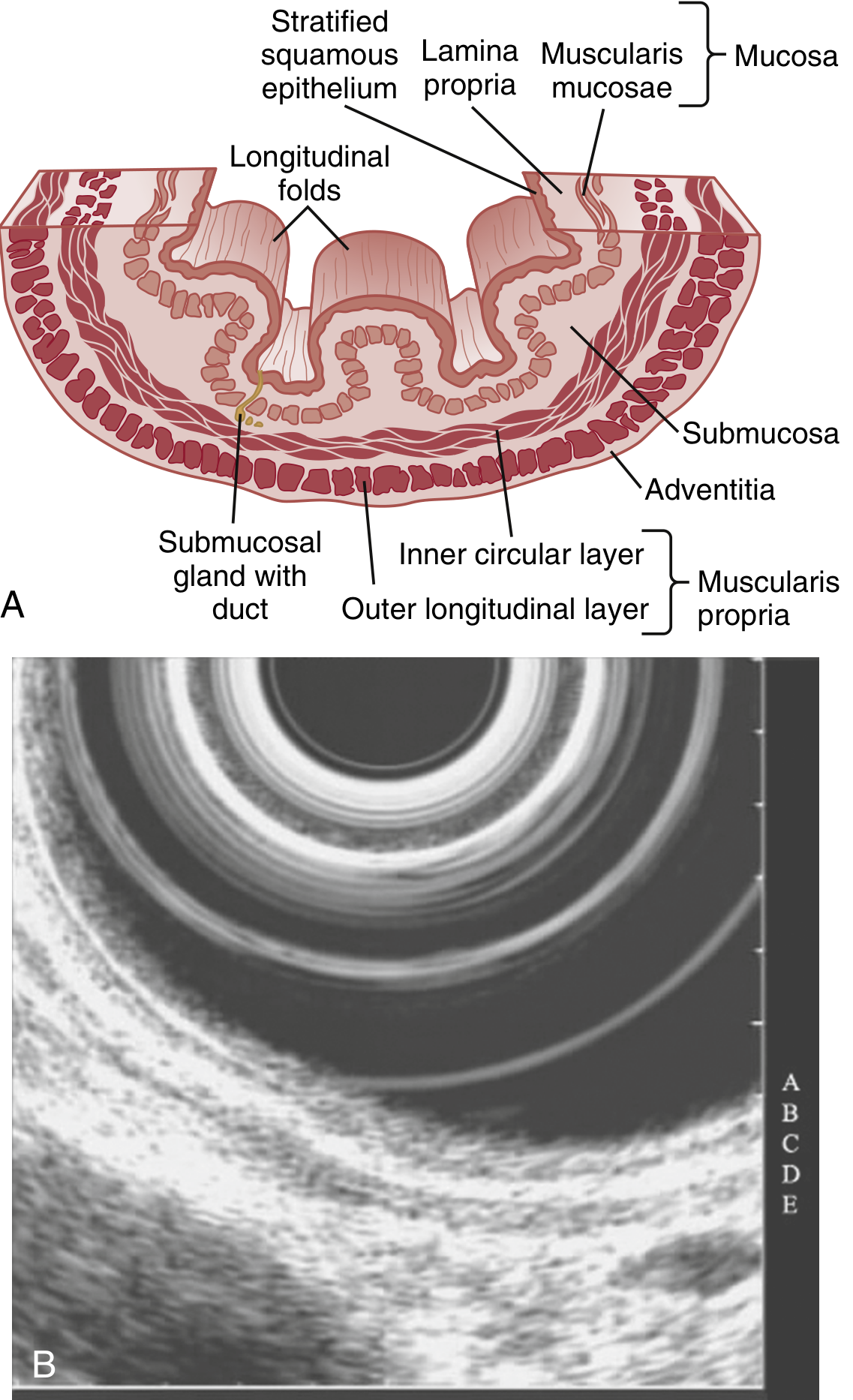
Mucosa
- Lined by non-keratinized stratified squamous epithelium with three sublayers:
- Stratum basale/germinativum — basophilic cylindrical cells with mitotic activity; cell turnover ~5–8 days
- Stratum spinosum/intermedium — cells contain glycogen and membrane-coating granules
- Stratum superficiale/corneum — flat cells parallel to surface with tight junctions and intercellular mucin forming a protective seal
- The lamina propria forms dermal papillae (rete pegs) that project into the epithelium and contain vasculature; they normally extend <⅔ of the mucosal thickness (dilation of intercellular spaces is a marker of GERD and eosinophilic esophagitis)
- Muscularis mucosae — thin layer of smooth muscle separating mucosa from submucosa
- The esophagus contains intraepithelial lymphocytes (cytotoxic T cells) and Langerhans cells; neutrophils/eosinophils indicate inflammation
Submucosa
- Loose connective tissue containing submucosal (Meissner's) plexus, blood vessels, lymphatics, and mucous glands (esophageal glands proper) — their ducts open into the lumen and are unique to the esophagus
Muscularis Propria
- Inner circular + outer longitudinal layers
- Composition varies by level:
- Upper 5–33% — exclusively skeletal muscle
- Middle third — mixed skeletal and smooth muscle
- Lower 50% — exclusively smooth muscle
- Contains the myenteric (Auerbach's) plexus between the layers
Adventitia
- Outermost layer of loose connective tissue (no serosa)
- The absence of serosa allows perforations and malignancies to disseminate more readily and makes surgical repair/anastomosis more difficult
5. Sphincters
Upper Esophageal Sphincter (UES)
- Formed by the cricopharyngeus muscle (a specialized portion of the inferior pharyngeal constrictor)
- Located at the pharyngo-esophageal junction
- Composed of skeletal muscle; contracted at rest → high-pressure zone preventing air entry
- Relaxes during swallowing, vomiting, and belching
Lower Esophageal Sphincter (LES)
- A 2–4 cm length of asymmetrically thickened circular smooth muscle
- Located in the distal esophagus within the diaphragmatic hiatus (right crus)
- Anchored by the phrenoesophageal ligament (from transversalis fascia)
- Contracted at rest → prevents gastric reflux
- Relaxes during swallowing via vagal (non-adrenergic, non-cholinergic) neurotransmission
- Diaphragmatic contractions augment LES pressure during exercise
6. Arterial Supply
The blood supply is segmental, with rich submucosal anastomoses that account for the rarity of esophageal infarction and allow esophageal mobilization to the aortic arch without ischemia.
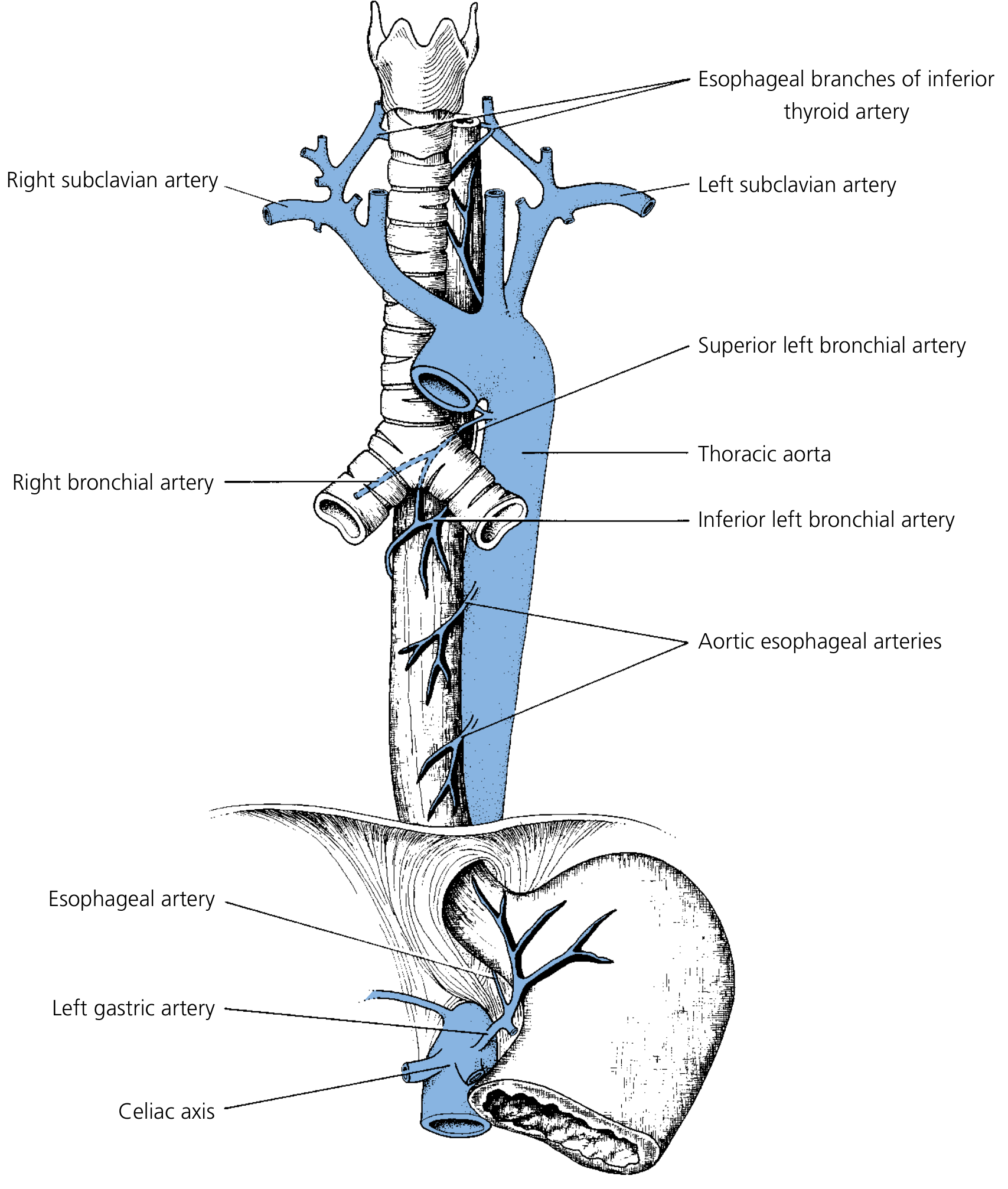
| Segment | Arterial Source |
|---|---|
| Cervical esophagus | Branches of the inferior thyroid artery (primary); accessory supply from common carotid, subclavian, vertebral, and ascending pharyngeal arteries |
| Thoracic esophagus | Direct aortic esophageal branches (typically 2, from thoracic aorta); bronchial arteries (frequently 2 on the right, 1 on the left); right intercostal arteries |
| Abdominal esophagus | Ascending branch of left gastric artery; left inferior phrenic arteries (bilateral); short gastric and splenic arteries |
In the muscular layer, these vessels branch extensively to create an extensive longitudinal vascular plexus — this is why esophageal surgeons can safely mobilize the esophagus over considerable length.
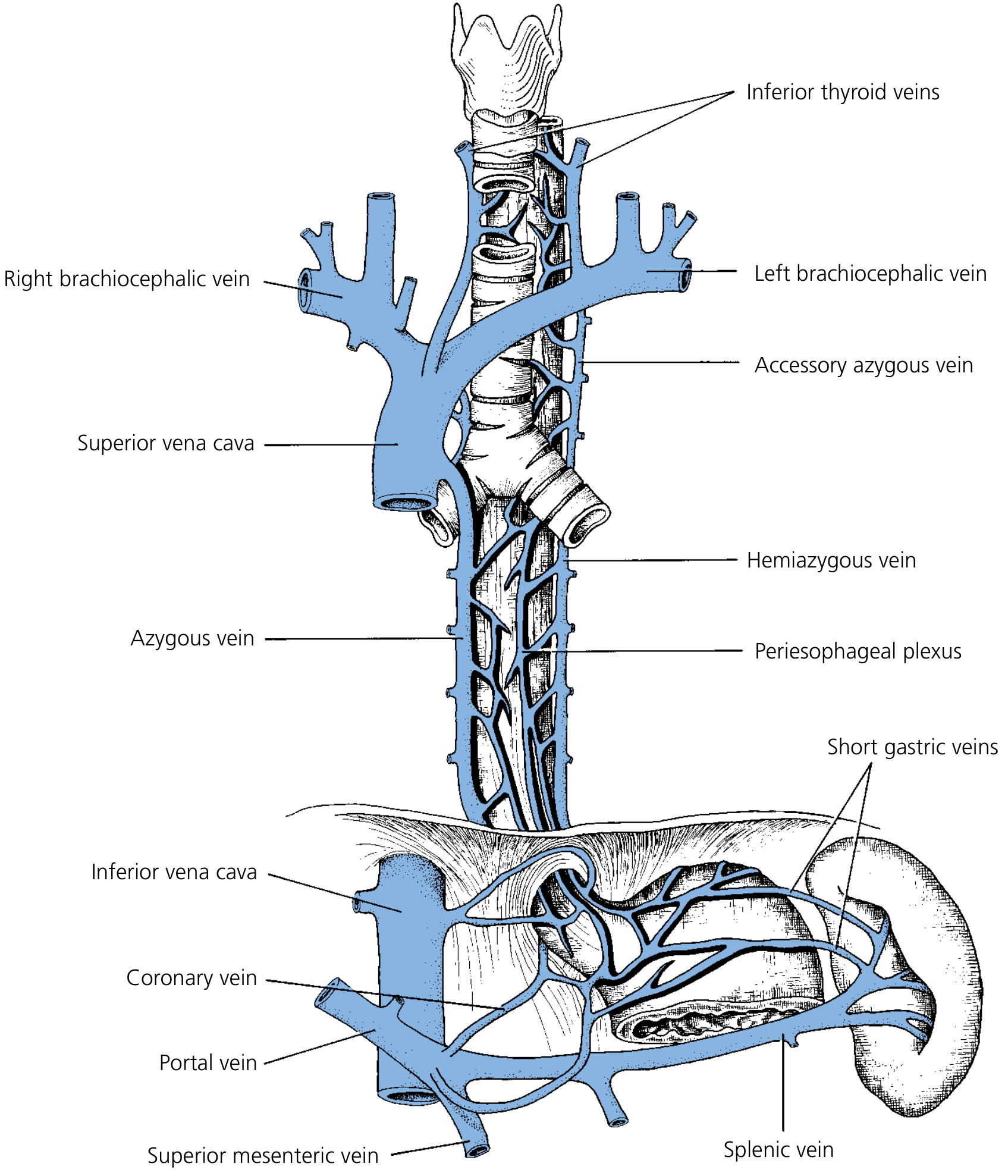
7. Venous Drainage
The venous anatomy is characterized by rich plexuses at multiple depths that create critical portosystemic anastomoses.
Venous Layers (Deep to Superficial)
- Fine intraepithelial channels → subepithelial superficial venous plexus
- Deep intrinsic veins in submucosa — connect with superficial plexus; at the gastroesophageal junction communicate with gastric counterparts
- Perforating veins — connect deep intrinsic veins through the muscularis propria to the adventitial veins
- Adventitial (periesophageal) venous plexus — drains to regional veins
Segmental Drainage
| Segment | Venous Drainage | Systemic Destination |
|---|---|---|
| Cervical | Inferior thyroid vein → brachiocephalic vein | Superior vena cava |
| Thoracic | Azygos vein (right), hemiazygos vein (left), intercostal veins (when hemiazygos absent) | Superior vena cava |
| Abdominal | Left gastric (coronary) vein → portal vein | Hepatic portal system |
Portosystemic Anastomosis & Varices
The distal esophagus is a key watershed zone between the portal and systemic (azygos) circulations. In portal hypertension, retrograde flow through the left gastric vein → esophageal submucosal venous plexus → azygos → superior vena cava causes esophageal varices (most dangerous portosystemic anastomosis due to risk of massive hemorrhage). Varices may extend up to the level of the aortic arch (the upper limit of azygos drainage of the lower esophagus). "Downhill varices" occur above this level, caused by obstruction in the cervical venous system or superior vena cava — the terminology refers to the direction of venous flow relative to the obstruction.
8. Lymphatic Drainage
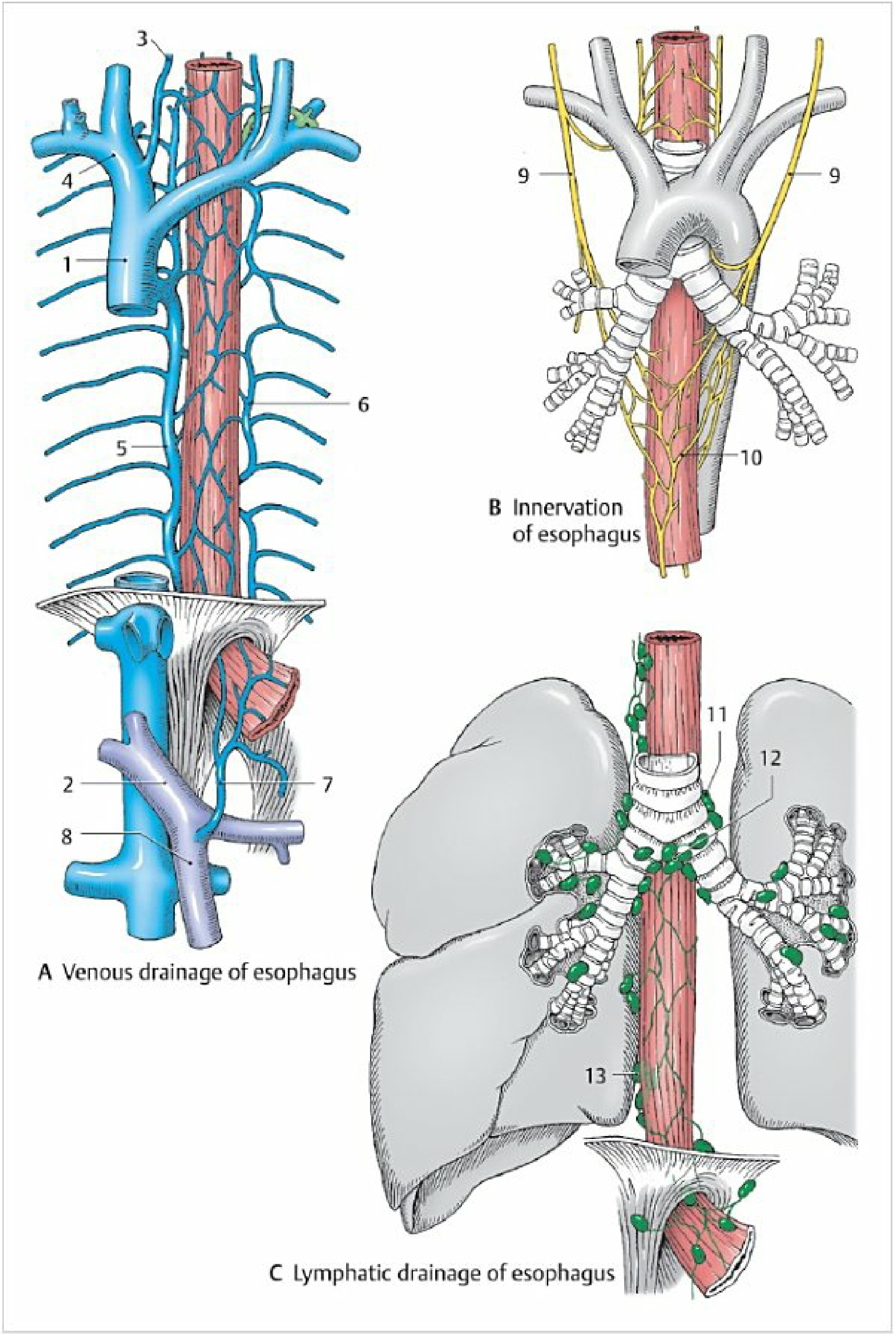
Intramural Lymphatics
Esophageal lymphatic channels form a very dense plexus in the submucosa, just below the muscularis mucosae. Unlike other GI organs, lymph flows primarily in the longitudinal direction (rather than radially) — lymphatics in the thoracic esophagus can travel great distances longitudinally before penetrating the muscularis propria to enter regional nodes. This anatomical arrangement has critical oncological consequences:
Esophageal tumors have a high rate of skip metastases — nodal involvement distant from the primary tumor is common, and lymph node spread is almost always present beyond the local region at the time of diagnosis.
Segmental Lymph Node Drainage
Unlike the arterial supply, the lymphatic drainage of the esophagus is NOT strictly segmental. Multiple interconnections exist between all nodal chains.
| Segment | Primary Nodal Drainage |
|---|---|
| Cervical esophagus | Lower group of deep cervical lymph nodes; paratracheal nodes |
| Upper thoracic esophagus | Paratracheal nodes; tracheobronchial (carinal) nodes; posterior mediastinal nodes |
| Mid-thoracic esophagus | Tracheobronchial nodes; posterior mediastinal nodes; pericardial nodes; internal jugular nodes |
| Lower thoracic esophagus | Posterior mediastinal nodes; prevertebral nodes |
| Abdominal esophagus | Perigastric nodes (along lesser curvature); subphrenic nodes; celiac nodes |
The internal jugular, tracheal, tracheobronchial, posterior mediastinal, and pericardial nodes all drain adjacent esophageal segments. The paraesophageal lymph node chain runs the length of the organ.
Clinical Importance
- Esophageal cancer spreads early and widely via this submucosal lymphatic network
- Tumors near the carina can metastasize both to cervical nodes (upward) and celiac nodes (downward)
- This is why radical esophagectomy for cancer requires removal of extensive nodal fields (three-field lymphadenectomy: cervical + thoracic + abdominal)
- Early metastasis to cervical, paraesophageal, and mediastinal nodes is a hallmark of squamous cell carcinoma
9. Innervation
Parasympathetic (Vagus — CN X)
- UES and cervical esophagus: innervated by recurrent laryngeal nerves (branches of CN X)
- The left recurrent laryngeal nerve loops under the aortic arch; the right loops under the subclavian artery
- Injury → impaired vocal cord movement + cricopharyngeal dysfunction → aspiration risk
- Upper thoracic esophagus: left recurrent laryngeal nerve and both vagus nerves
- Mid/lower thoracic esophagus: the right and left vagus nerves descend on the outer esophageal surface and rotate counter-clockwise:
- Left vagus → anterior vagal trunk
- Right vagus → posterior vagal trunk
- Both travel with the esophagus into the abdomen through the hiatus
- Motor cell bodies for striated muscle: nucleus ambiguus; for smooth muscle: dorsal motor nucleus of vagus
- Vagal afferents (chemical, thermal, mechanical stimuli): cell bodies in nodose ganglia, project to nucleus solitarius
Sympathetic
- Cervicothoracic (stellate) ganglion, thoracic sympathetic trunk, and abdominal aortic plexus
- Both autonomic divisions connect to the enteric nervous system (myenteric and submucosal plexuses)
Clinical Note
Esophageal and cardiac pain share the same afferent visceral sensory pathways, terminating in the first four thoracic spinal cord segments — hence identical chest pain presentations. Esophageal acid reflux can also trigger reflex cough via connections with tracheobronchial innervation.
10. Embryology & Physiology Summary
The esophagus develops from the foregut endoderm. Key physiological features:
- Peristalsis: primary peristalsis (vagally triggered by swallowing); secondary peristalsis (response to esophageal distension, governed by intrinsic enteric nerves)
- UES function: prevents aspiration; relaxes during swallowing (0.5 second coordinated sequence involving CN V, VII, X, XI, XII and C1–C3 motor neurons)
- LES function: maintains a resting pressure of 10–35 mmHg; transient LES relaxations (TLESRs) are the primary mechanism of GERD
Summary Table: Vasculature and Lymphatics at a Glance
| Feature | Cervical | Thoracic | Abdominal |
|---|---|---|---|
| Arterial | Inferior thyroid a. | Aortic branches, bronchial a. | Left gastric a., inf. phrenic a. |
| Venous | Inferior thyroid v. → SVC | Azygos/hemiazygos → SVC | Left gastric v. → portal v. |
| Lymphatic | Deep cervical, paratracheal nodes | Tracheobronchial, posterior mediastinal, pericardial nodes | Perigastric, celiac nodes |
Sources: Gray's Anatomy for Students; Yamada's Textbook of Gastroenterology 7e; Sleisenger & Fordtran's Gastrointestinal and Liver Disease; Mulholland & Greenfield's Surgery 7e; Color Atlas of Human Anatomy Vol. 2
This is a shared conversation. Sign in to Orris to start your own chat.