Shoulder test for impingement
Reading File
Finding Sources
Searching the Web
shoulder impingement tests Neer Hawkins Kennedy clinical examination
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Here is a complete overview of the clinical tests for shoulder impingement:
Shoulder Impingement Tests
Subacromial impingement syndrome involves compression of the rotator cuff (most often the supraspinatus) and subacromial bursa between the humeral head and the coracoacromial arch. Several provocative tests are used together, since no single test is both highly sensitive and specific.
1. Neer Impingement Sign
Technique: The examiner stabilizes the scapula with one hand (preventing scapular rotation), then raises the patient's straightened arm in full forward flexion to overhead.
Positive: Pain in the arc between 70-120 degrees of forward flexion.
Mechanism: Drives the greater tuberosity and supraspinatus under the anterior acromion, reproducing anterior impingement.
Accuracy: Sensitivity 75-89%; Specificity 30-40% (high sensitivity but poor specificity - good for ruling out).
2. Hawkins-Kennedy Test
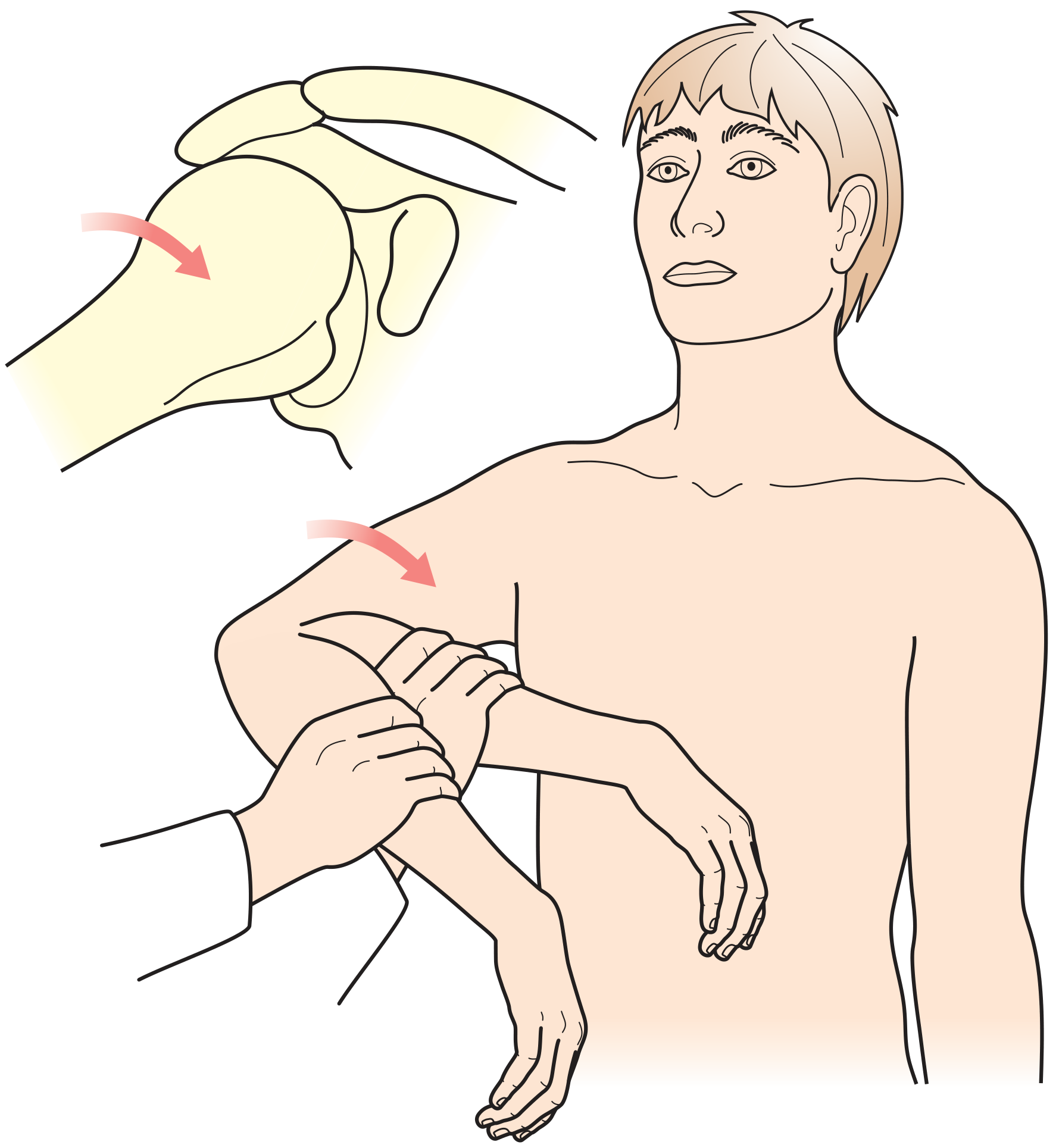
Technique: Position the shoulder at 90° of forward flexion and 90° of elbow flexion. The examiner then forcibly internally rotates the shoulder (bringing the forearm downward).
Positive: Pain on internal rotation.
Mechanism: Drives the greater tuberosity and anterior rotator cuff underneath the acromion and coracoacromial ligament, compressing the supraspinatus tendon and subacromial bursa.
Accuracy: Sensitivity 91-92%; Specificity 25-44% (most sensitive of the impingement tests, but again low specificity).
3. Painful Arc Test
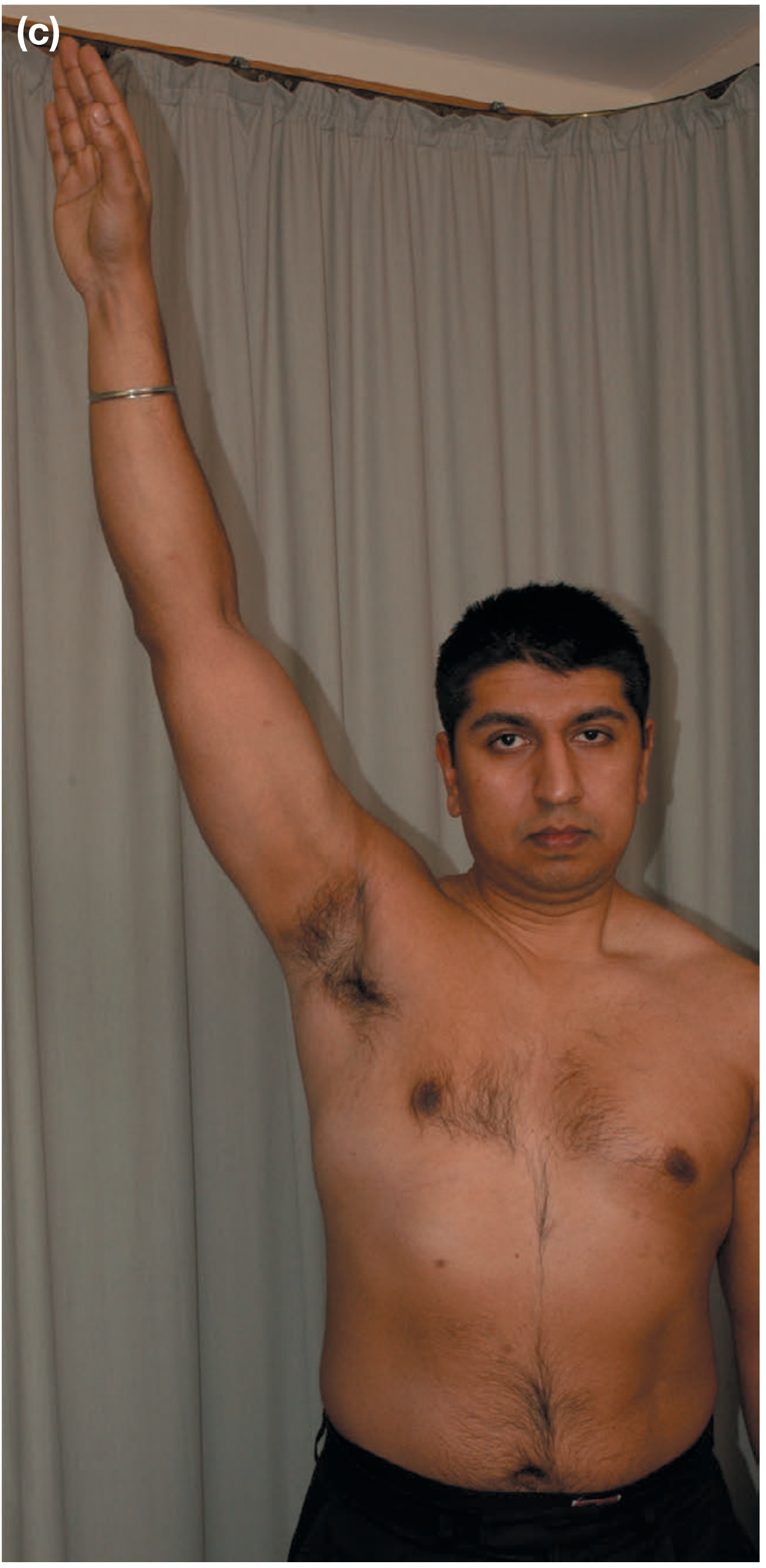
Technique: Ask the patient to actively abduct both arms from the sides overhead.
Positive: Pain specifically in the arc from 60° to 120° of abduction. Pain outside this range is less indicative of impingement.
Mechanism: At 60-120°, the greater tuberosity passes beneath the acromion and coracoacromial ligament - the narrowest point of the subacromial space.
4. Jobe's Test (Empty Can Test)

Technique: Patient abducts the arm to 90° in the scapular plane with the thumb pointing downward ("empty can" position - as if pouring out a can). The examiner applies downward resistance at the distal forearm/wrist.
Positive: Pain and/or weakness against resistance.
Mechanism: Isolates the supraspinatus and loads the tendon in the position of maximum impingement. Weakness (rather than just pain) raises suspicion for a rotator cuff tear.
Additional Rotator Cuff Muscle Tests
These help localize which muscle is affected:
| Muscle | Test | Technique |
|---|---|---|
| Infraspinatus / Teres minor | External rotation resistance | Elbow at 90° against the side; resist external rotation |
| Subscapularis | Lift-off test | Hand behind the back; push dorsum of hand away from back against resistance |
Neer Impingement Test (Diagnostic Injection)
A useful confirmatory maneuver: inject 10 mL of lidocaine into the subacromial space. If this significantly reduces pain on repeat provocative testing (Neer test), it confirms subacromial impingement as the source (positive "impingement test"). This distinguishes pain from impingement vs. intrinsic rotator cuff tear (injection reduces pain but not weakness from a true tear).
Diagnostic Summary
| Test | Sensitivity | Specificity | Best Use |
|---|---|---|---|
| Hawkins-Kennedy | 91-92% | 25-44% | Screening / rule out |
| Neer sign | 75-89% | 30-40% | Screening / rule out |
| Painful arc | Moderate | Moderate | Supports impingement |
| Empty can (Jobe) | Moderate | Higher | Supraspinatus tear |
Because all individual tests have low specificity, combining a positive Hawkins test + painful arc + weakness on external rotation gives the highest diagnostic accuracy for impingement syndrome. A positive drop-arm sign (inability to slowly lower the arm) shifts suspicion toward a complete rotator cuff tear.
Sources: Bailey and Love's Short Practice of Surgery 28th Ed., Tintinalli's Emergency Medicine, Textbook of Family Medicine 9e
This is a shared conversation. Sign in to Orris to start your own chat.