Pulmonary receptors full details for md exam answer 15 marks
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Finding Sources
I now have all the material needed for a complete 15-mark MD exam answer. Here it is:
Pulmonary Receptors
Introduction
The lungs and airways contain three major groups of sensory receptors, all conveying afferent signals centrally via the vagus nerve (CN X) to the nucleus tractus solitarius (NTS) in the medulla. These receptors play key roles in controlling breathing pattern, protecting airways, and mediating several important reflexes.
The three groups are:
- Slowly Adapting Pulmonary Stretch Receptors (SARs / PSRs)
- Rapidly Adapting Receptors (RARs) - "Irritant Receptors"
- C-Fiber Receptors (J Receptors / Juxtacapillary Receptors)
1. Slowly Adapting Pulmonary Stretch Receptors (SARs)
Location
- Located in the smooth muscle of the tracheobronchial tree, from the extrathoracic trachea down through the intrapulmonary bronchi.
Fiber type
- Afferent signals travel via myelinated vagal fibers - hence rapid conduction.
Stimulus
- Activated by lung inflation (mechanical stretch of airway walls).
- Discharge increases with lung inflation and decays very slowly over time (hence "slowly adapting").
- Not significantly stimulated by chemical stimuli (exception: hypocapnia can activate them).
Reflex - The Hering-Breuer Reflex
This is the most important reflex mediated by SARs and was described by Hering and Breuer in 1868 as one of the first examples of negative feedback in physiology.
Inflation reflex (Hering-Breuer inflation reflex):
- Sustained lung inflation activates SARs → vagal afferents signal the medulla → inspiratory activity is terminated (phrenic motor neuron output is inhibited) → expiration begins.
- This prevents over-inflation of the lungs and helps regulate tidal volume.
- It also increases respiratory frequency by shortening inspiration, maintaining constant alveolar ventilation.
Deflation reflex (Hering-Breuer deflation reflex):
- Marked deflation of the lung → decreases the duration of expiration → promotes the next inspiration.
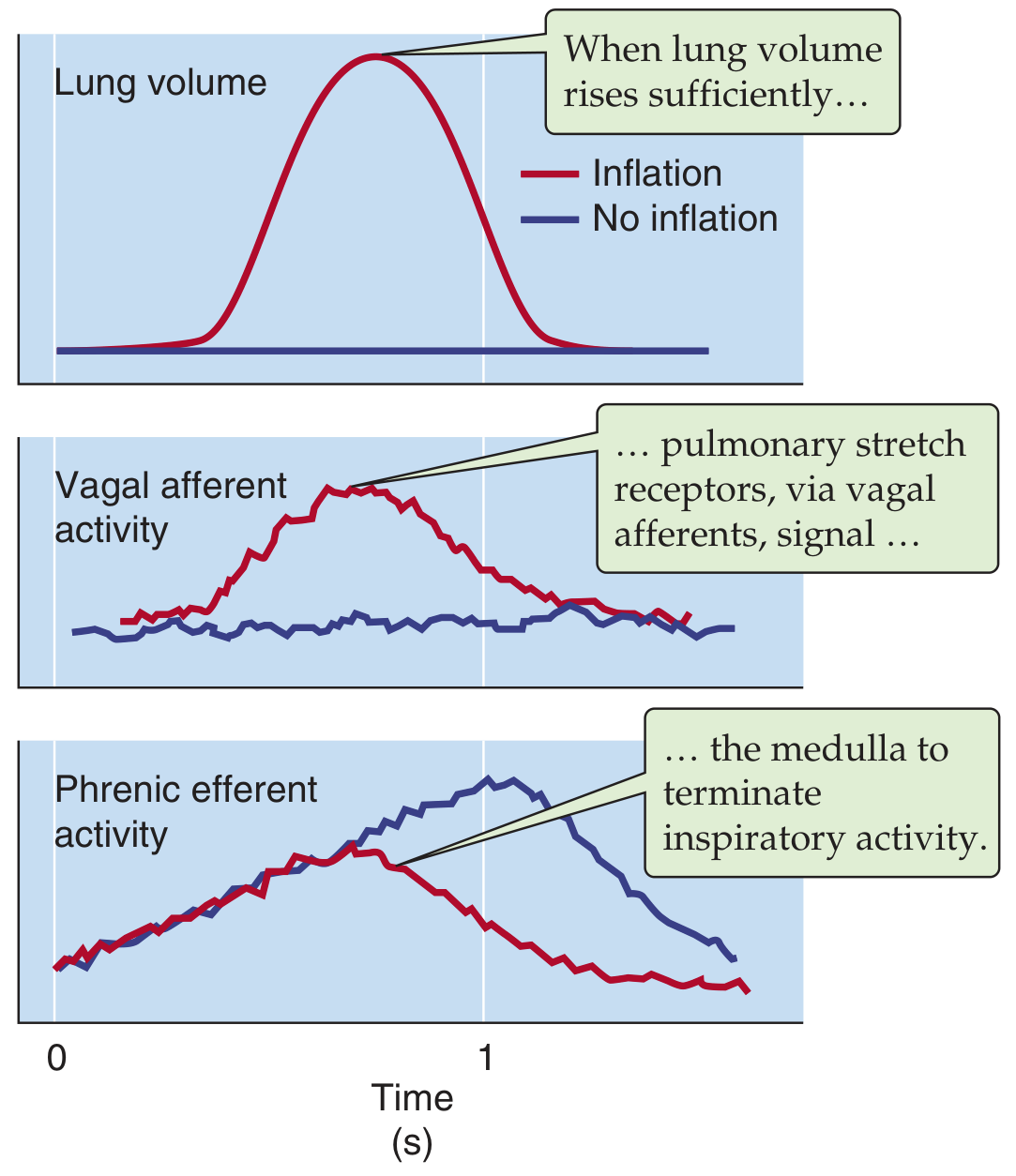
Figure: Hering-Breuer reflex. Lung inflation (red) triggers vagal afferent activity, which terminates phrenic efferent (inspiratory) activity earlier than without inflation (blue). (Medical Physiology, Boron & Boulpaep)
Clinical Significance
- In human adults, this reflex operates mainly above tidal volume range - it is particularly active in pathological over-inflation and in newborn infants where it helps regulate normal breathing.
- Feedback from SARs may also help the medulla select the optimal combination of tidal volume and respiratory frequency to minimize work of breathing.
2. Rapidly Adapting Receptors (RARs) - "Irritant Receptors"
Location
- Located throughout the tracheobronchial tree, primarily in the epithelial and submucosal layers of the larger airways (trachea and large bronchi).
Fiber type
- Afferent signals travel via myelinated vagal fibers (same as SARs but different receptors).
Stimulus
- Respond to sudden, sustained lung inflation with a rapid increase in firing rate that decreases to 20% or less of initial rate within 1 second (hence "rapidly adapting").
- Also stimulated by rapid lung deflation.
- Unlike SARs, RARs are highly sensitive to a wide range of chemical irritants:
- Histamine, serotonin, prostaglandins, bradykinin
- Ammonia, cigarette smoke, ether
- Dust and particulates
- Mucus, edema fluid
- This chemical sensitivity gave them the name "irritant receptors."
- They also increase firing as rate of airflow increases.
Reflexes Mediated
| Location of stimulation | Reflex response |
|---|---|
| Trachea/large airways | Cough, bronchoconstriction, mucus secretion |
| Lung parenchyma | Hyperpnea (increased breathing) |
| During lung deflation | Increased respiratory frequency (Head's paradoxical reflex in newborns) |
Bronchoconstriction in asthma: RARs respond to histamine released during asthmatic episodes. In some cases histamine directly stimulates the receptor; in others, it first triggers bronchoconstriction (volume change) which then activates the stretch receptor.
Clinical Significance
- These receptors detect pathophysiological processes in the airway: chemical irritation, mucosal congestion, inflammation, and edema.
- They drive the cough reflex - a critical airway defense mechanism.
- They contribute to bronchoconstriction seen in asthma and anaphylaxis.
- Laryngeal narrowing and cough triggered by inhaled irritants are primarily RAR-mediated.
3. C-Fiber Receptors (J Receptors / Juxtacapillary Receptors)
Location
- Nerve endings of unmyelinated C fibers situated in alveolar walls and conducting airways, close to pulmonary capillaries - hence the name "juxtacapillary (J) receptors" (proposed by Paintal).
- Two subgroups:
- Pulmonary C fibers - near pulmonary capillaries in alveolar walls
- Bronchial C fibers - near bronchial circulation in the airways
Fiber type
- Unmyelinated (C fibers) - slow conduction velocity.
- Travel centrally via the vagus nerve.
Stimulus
- Stimulated by hyperinflation of the lung.
- Also stimulated by increases in pulmonary vascular pressure and capillary pressure (pulmonary vascular congestion, pulmonary edema).
- Respond to exogenously and endogenously released chemicals:
- Capsaicin (classical J receptor stimulant - used experimentally)
- Phenyl diguanide
- Bradykinin, serotonin, prostaglandins
- Substances released during pulmonary embolism and congestion
Reflex - Pulmonary Chemoreflex (Bezold-Jarisch-like reflex)
Stimulation of J receptors produces the pulmonary chemoreflex:
- Apnea (brief cessation of breathing)
- Followed by rapid, shallow breathing
- Bradycardia
- Hypotension (fall in blood pressure)
- Bronchoconstriction
- Increased mucus secretion
A similar cardiovascular response is seen with cardiac C-fiber stimulation (the Bezold-Jarisch reflex of the heart).
C-Fiber Triad
Stimulation of C-fiber endings elicits a defensive triad:
- Rapid and shallow breathing
- Bronchoconstriction
- Increased mucus secretion into airways
These responses enhance turbulence in the airway, favoring deposition of foreign particles in mucus higher up in the bronchial tree where mucus-secreting cells are concentrated.
Clinical Significance
- Pulmonary edema: J receptors are stimulated by elevated pulmonary capillary pressure → rapid, shallow breathing (tachypnea) of left heart failure is partly J-receptor mediated.
- Pulmonary embolism: J receptors activated by released endogenous substances → reflex tachypnea.
- Exercise: Uncomfortable sensations from J receptor activation may contribute to the feeling of dyspnea and fatigue during intense exercise.
- Dyspnea in lung disease: Atelectasis, congestion, and inflammation all stimulate C fibers.
Comparison Table
| Feature | SARs (Slowly Adapting) | RARs (Rapidly Adapting / Irritant) | C-Fiber / J Receptors |
|---|---|---|---|
| Fiber type | Myelinated | Myelinated | Unmyelinated (C fibers) |
| Location | Airway smooth muscle, extrathoracic to intrapulmonary bronchi | Epithelial/submucosal, large airways | Alveolar walls, near capillaries |
| Stimulus | Sustained lung inflation | Lung inflation/deflation, irritants, chemicals | Hyperinflation, congestion, chemicals (capsaicin) |
| Adaptation | Very slow (sustained discharge) | Very rapid (< 1 sec) | Slowly (but primarily chemical) |
| Key reflex | Hering-Breuer inflation/deflation reflex | Cough, bronchoconstriction, hyperpnea | Pulmonary chemoreflex (apnea → tachypnea, bradycardia, hypotension) |
| Chemical sensitivity | Low (hypocapnia only) | High (histamine, bradykinin, smoke etc.) | High (capsaicin, bradykinin, prostaglandins) |
Additional Receptors
Chest Wall and Respiratory Muscle Receptors
- Muscle spindles in intercostal muscles and the diaphragm detect changes in thoracic cage volume.
- Joint receptors in costovertebral joints and tendon organs in respiratory muscles project centrally via spinal nerves (not vagus).
- These are important during exercise, posture change, and in pathological conditions with decreased lung or chest compliance.
- Input from proprioceptors in muscles, tendons, and joints stimulates inspiratory neurons - this helps increase ventilation during exercise.
Nasopharyngeal and Upper Airway Receptors
- Afferent signals from the upper airways travel via CN IX (glossopharyngeal nerve).
- Stimulation produces cough, sneeze, and bronchoconstriction.
Afferent Pathway Summary
All thoracic pulmonary receptors (SARs, RARs, C fibers) → vagus nerve (CN X) → nucleus tractus solitarius (NTS) in the medulla → modulation of the respiratory central pattern generator (rCPG) in the ventral respiratory group (VRC).
Clinical Correlations
| Condition | Receptor involved | Response |
|---|---|---|
| Asthma | RARs (histamine-mediated) | Bronchoconstriction, cough |
| Pulmonary edema | J receptors (↑ capillary pressure) | Rapid, shallow breathing (tachypnea) |
| Pulmonary embolism | J receptors (endogenous chemicals) | Tachypnea, hypotension |
| Inhalation of smoke/dust | RARs | Cough, laryngeal narrowing |
| Over-inflation on ventilator | SARs | Hering-Breuer - terminates inspiration |
| Dyspnea in heart failure | J receptors + RARs | Breathlessness, rapid breathing |
Sources
- Ganong's Review of Medical Physiology, 26th ed., Ch. 36 - "Responses Mediated by Receptors in the Airways & Lungs"
- Medical Physiology (Boron & Boulpaep) - "Stretch and Chemical/Irritant Receptors in the Airways and Lung Parenchyma"
- Fishman's Pulmonary Diseases and Disorders - "Mechanoreceptors"
- Murray & Nadel's Textbook of Respiratory Medicine - "Controller Feedback"
This is a shared conversation. Sign in to Orris to start your own chat.