pvns ortho 15 marks
Reading File
Finding Sources
Finding Sources
Searching PubMed
pigmented villonodular synovitis treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Loading Image
Loading Image
I have all the content needed for a comprehensive 15-mark answer. Let me now compile it.
Pigmented Villonodular Synovitis (PVNS)
(Also called Tenosynovial Giant Cell Tumor - Diffuse Type)
Definition
PVNS is a benign, locally aggressive villous or nodular proliferation of the synovium of uncertain aetiology that involves joints, bursae, or tendon sheaths. It results in recurrent haemarthroses and progressive joint destruction if untreated. The current WHO/pathology nomenclature terms it tenosynovial giant cell tumor (TGCT), but PVNS remains widely used clinically.
Epidemiology & Incidence
- Rare condition with an estimated incidence of ~1.8 per million per year
- Most patients are young adults in the 3rd and 4th decades of life, though it can present in childhood
- No strong sex predilection; some series show a slight female predominance
- Knee is the most commonly affected joint (~75-80%), followed by the hip (~15%), and less commonly the ankle, shoulder, wrist, and elbow
Classification / Forms
| Feature | Localized (Focal) Form | Diffuse Form |
|---|---|---|
| Also called | Focal nodular synovitis / Giant cell tumor of tendon sheath | Classic PVNS |
| Distribution | Single pedunculated nodule | Entire synovium of the joint |
| Common site | Anterior knee | Knee, hip, ankle |
| Histology | Identical to diffuse | Same - see below |
| Treatment | Marginal/arthroscopic excision | Total synovectomy |
| Recurrence | 0-8% | Higher (up to 45% diffuse knee) |
Pathogenesis / Aetiology
The exact cause is debated. Two major theories:
- Inflammatory/reactive theory - recurrent hemarthrosis causing reactive synovial hyperplasia
- Neoplastic theory - now favored; chromosomal translocations (especially t(1;2)) lead to overexpression of colony-stimulating factor 1 (CSF1), driving monocyte/macrophage proliferation of the synovium. This forms the basis of targeted CSF1R inhibitor therapy.
Clinical Features
- Monoarticular involvement (almost always a single joint)
- Chronic, insidious onset of pain and swelling of the affected joint
- Serosanguineous or blood-tinged joint aspirate - this is characteristic and an important clinical clue
- Mechanical symptoms (locking, clicking) when intraarticular loose bodies are present
- A palpable soft-tissue mass may be present
- Long diagnostic delay is common due to the nonspecific nature of symptoms
- In long-standing cases: destruction of cartilage and secondary degenerative change with joint space narrowing
Investigations
1. Joint Aspiration
- Aspirate is characteristically serosanguineous or frankly haemorrhagic (Group IV hemorrhagic fluid on classification)
- Not diagnostic on its own; cytology can rule in/out PVNS
2. Plain Radiographs
- Often normal early in the disease
- May show: joint effusion / soft-tissue swelling
- Bone erosion on both sides of the joint (on a background of preserved joint space and normal bone density)
- Importantly, calcification is rare (helps distinguish from synovial chondromatosis)
- In the hip: erosion can produce an "apple core" appearance (narrowing of femoral neck), with subchondral cysts having sclerotic rims (Fig 30.14A & B)
- In large joints (knee): erosions are less frequent because the capsule has greater capacity
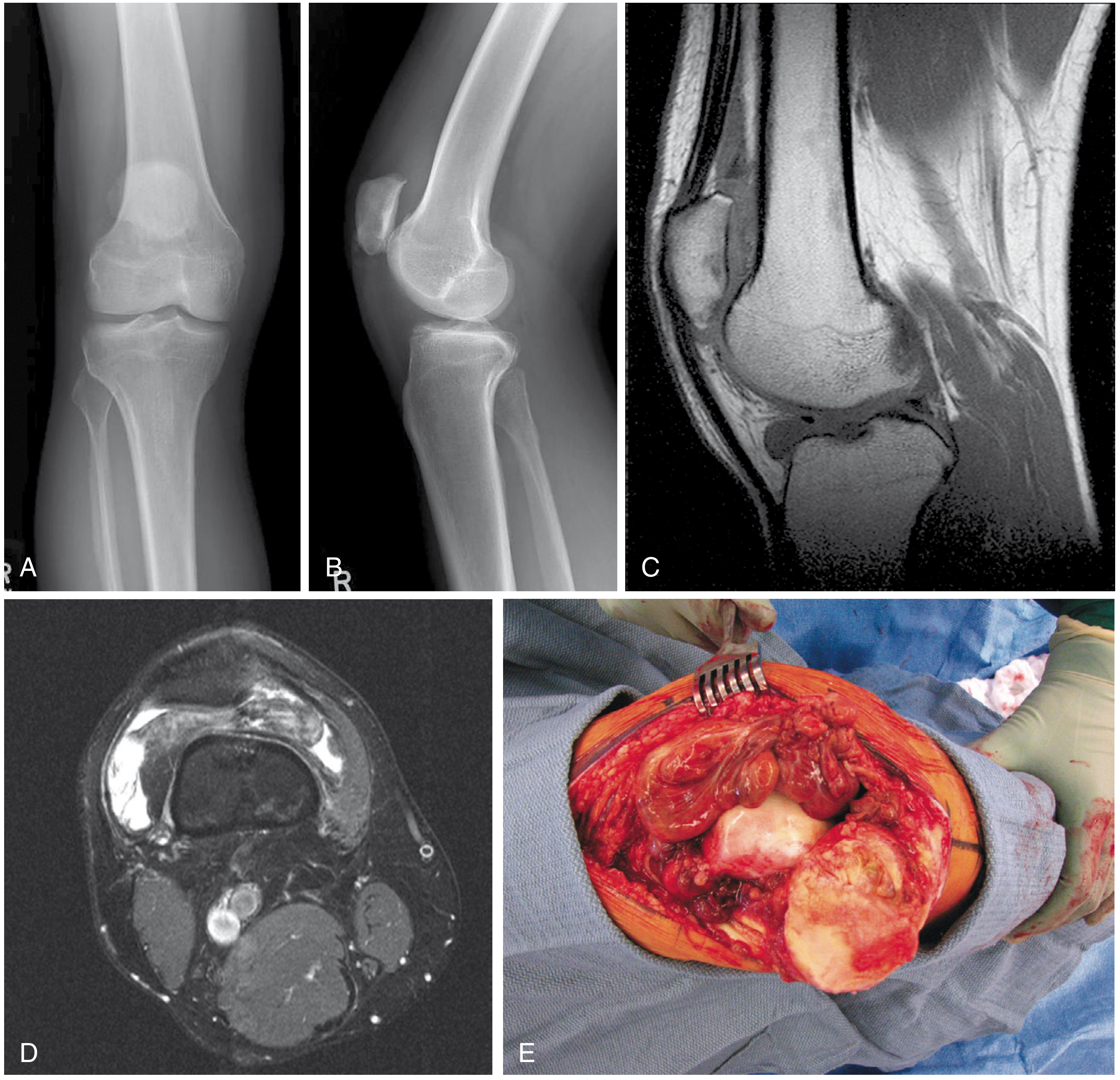
FIGURE 30.14 (Campbell's Operative Orthopaedics): A and B - Plain radiographs of knee PVNS show no soft-tissue abnormality. C - T1-weighted sagittal MRI shows dark intraarticular process. D - T2-weighted axial MRI also shows dark signal. E - Intraoperative photo shows diffuse pigmented villonodular synovitis.
3. MRI - Investigation of Choice
- Provides the best diagnostic clue due to hemosiderin deposition in hypertrophied synovium
- Classic finding: low signal intensity on BOTH T1 and T2 weighted images (dark on both) - this is due to hemosiderin from recurrent hemorrhage
- T2 (gradient-echo) sequences* show characteristic blooming artifact due to hemosiderin - most sensitive
- Bone erosions, subchondral "cysts," and synovial tissue extent clearly delineated
- Joint effusion also well seen
- Post-contrast: synovial proliferation enhances
4. CT
- Non-enhanced CT shows high attenuation within the mass (due to hemosiderin)
- Synovial proliferation enhances with contrast
- Useful for bony detail
Histopathology
Gross: Brownish/rust-colored synovium due to hemosiderin; villi and nodular projections throughout the joint.
Microscopy (H&E): The characteristic features are:
- Bland polyhedral (synoviocyte-like) cells in sheets or papillary projections
- Multinucleated giant cells (osteoclast-type)
- Hemosiderin deposits (golden-brown pigment in macrophages)
- Foamy (lipid-laden) macrophages
- Collagenous stroma with chronic inflammatory infiltrate
- No cytological atypia or high mitotic activity (benign)
The focal form (giant cell tumor of tendon sheath) is histologically identical to the diffuse articular form.
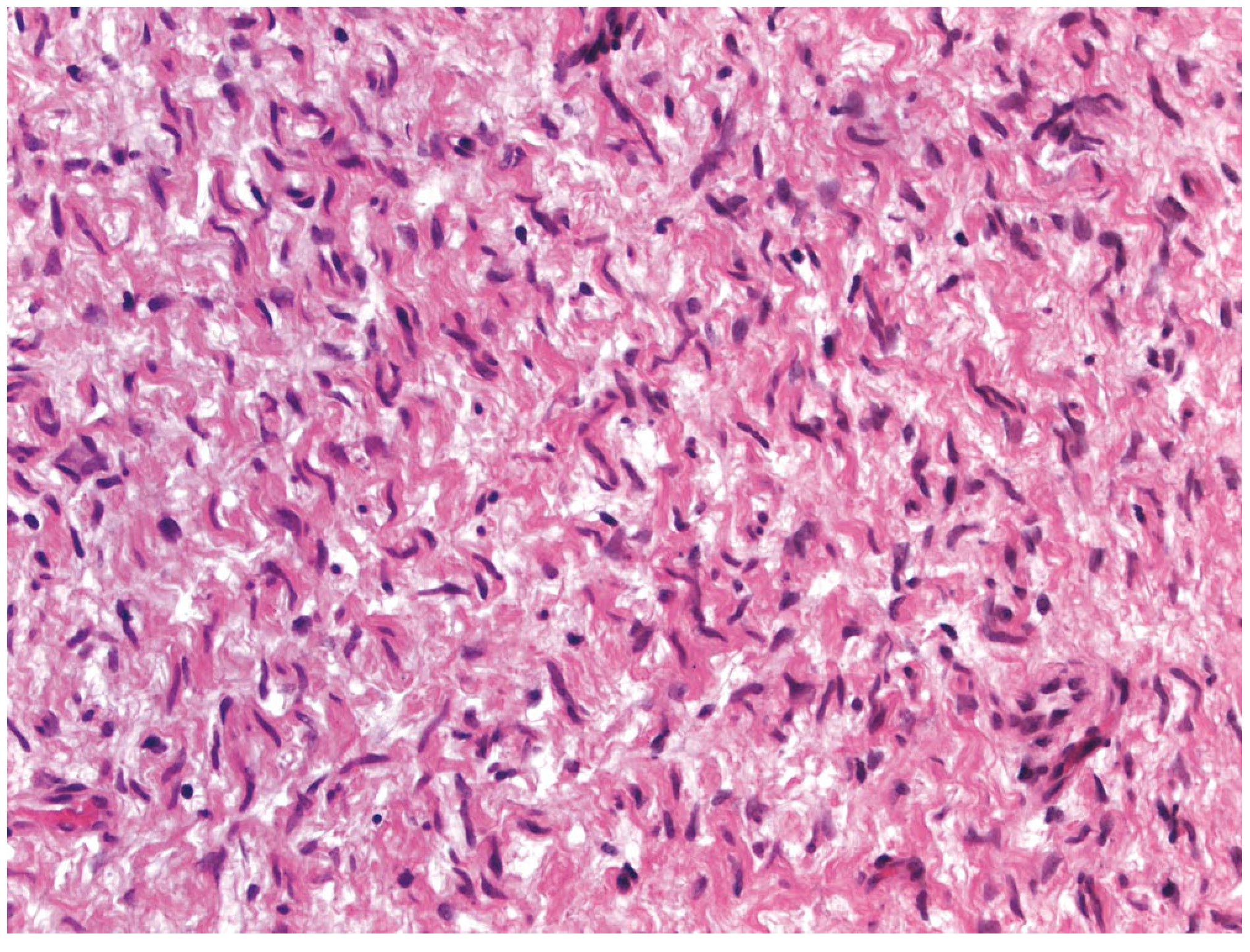
FIGURE 30.13 (Campbell's): PVNS photomicrograph (H&E x20) - bland polyhedral cells surrounded by collagen, with giant cells and hemosiderin present.
Differential Diagnosis
| Condition | Distinguishing Feature |
|---|---|
| Haemophilic arthropathy | Known coagulopathy, similar MRI; no synovial nodules |
| Synovial haemangioma | Phleboliths on imaging; rare |
| Synovial chondromatosis | Calcified loose bodies; MRI shows high signal foci |
| Rheumatoid arthritis | Polyarticular, serology positive |
| Septic arthritis | Fever, raised inflammatory markers, turbid aspirate |
| Lipoma arborescens | High T1 signal (fat) that suppresses on fat-sat sequences |
Treatment
Goals: alleviation of symptoms, minimizing recurrence, and preservation of the joint.
Localized Form
- Arthroscopic or open marginal excision - treatment of choice
- Recurrence rate: 0-8% after arthroscopic excision
- Excellent prognosis
Diffuse Form
- Total synovectomy - either open, arthroscopic, or combined
- Can be done arthroscopically (e.g., posterior trans-septal portal technique for the knee)
- Higher recurrence rates (up to ~45% with incomplete synovectomy)
- If secondary degenerative changes are present: arthroplasty should be strongly considered
- Radiotherapy (adjuvant radiation synovectomy) may be justified in the diffuse form if surgery fails to control the disease
- CSF1R inhibitors (e.g., pexidartinib): clinical trials underway and showing promise - targets the CSF1/CSF1R pathway that drives synovial proliferation; FDA-approved for TGCT not amenable to surgery
Prognosis
- Benign, locally aggressive; no metastatic potential
- Localized form has excellent prognosis with low recurrence
- Diffuse form has significant recurrence rates (varies 10-50% depending on completeness of synovectomy)
- Long-standing disease causes progressive cartilage and bone destruction, resulting in secondary osteoarthritis
- Malignant transformation is extremely rare
Key Points Summary
- PVNS = benign synovial proliferation; now called tenosynovial giant cell tumor
- Young adults; knee most common joint (~75%)
- Monoarticular; blood-tinged aspirate is characteristic
- MRI hallmark: dark on both T1 and T2 due to hemosiderin; blooming on T2* GRE
- Histology: polyhedral cells + multinucleated giant cells + hemosiderin
- Two forms: localized (marginal excision) vs. diffuse (total synovectomy)
- No calcification (distinguishes from synovial chondromatosis)
- Hip involvement causes "apple-core" erosion of femoral neck
- CSF1R overexpression is the underlying molecular driver
- Adjuvant radiotherapy and CSF1R inhibitors available for refractory cases
Sources: Campbell's Operative Orthopaedics 15th Ed 2026 (p.1264-1265); Grainger & Allison's Diagnostic Radiology; Grainger & Allison Vol 2 (p.1910)
pagets disease ortho 5 marks
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I have comprehensive content. Here is a focused 5-mark answer:
Paget's Disease of Bone (Osteitis Deformans)
Definition
A localized, chronic bone-remodeling disorder characterized by excessive, disordered osteoclastic bone resorption followed by compensatory osteoblastic new bone formation, resulting in a structurally disorganized, expanded, fragile skeleton. The new bone is mechanically inferior - larger in volume but weaker in architecture.
Aetiology & Pathogenesis
Two factors - genetic and environmental/viral:
- Genetic: Mutations in SQSTM1 (sequestosome-1, encoding p62 protein) found in ~50% familial and ~10% sporadic cases, leading to increased NF-κB activity and osteoclast hyperactivity. Mutations in RANK (TNFRSF11A) and OPG (TNFRSF11B) account for juvenile Paget's. Positive family history in 15-25% of patients.
- Viral: Paramyxovirus-like inclusions (measles, RSV, canine distemper virus) found in osteoclast nuclei. Viral mRNA detected in pagetic osteoclasts. The declining incidence of Paget's disease coincides with measles vaccination - supporting this theory, though a live virus has never been cultured.
Pathophysiology: Osteoclasts are abnormally large (up to 100 nuclei vs. 3-5 in normal), increased 10-100 fold, and hyperresponsive to RANKL and 1,25(OH)₂D₃. Erosion rate increases sevenfold. Osteoblasts are secondarily recruited in large numbers producing disorganized woven bone.
Phases of Disease (Three Sequential Stages)
| Phase | Predominant Process | Radiological Appearance |
|---|---|---|
| 1. Osteolytic (Active) | Osteoclastic resorption; marked hypervascularization | Advancing lytic wedge - "blade of grass" or "flame-shaped" lesion |
| 2. Mixed (Active) | Simultaneous resorption + formation; woven bone replaces lamellar | Mixed lytic + sclerotic pattern; bone enlargement |
| 3. Sclerotic (Burned-out) | Resorption declines; dense, avascular pagetic bone | Dense, thickened, enlarged bone - "cotton wool" skull |
All three phases may coexist simultaneously at different skeletal sites.
Epidemiology
- Age: Usually >40 years; prevalence increases with age (~3% at autopsy in those >40)
- Sex: Slight male predominance
- Geography: Common in Western Europe (UK, France, Germany), rare in Asia, Africa, Scandinavia
- Distribution: Monostotic in ~15%; polyostotic in ~85%
- Most commonly affected bones: pelvis, vertebrae, skull, femur, tibia
- Often asymptomatic - discovered incidentally on X-ray or elevated ALP
Clinical Features
Symptoms:
- Bone pain (most common) - from lytic expansion, microfractures, hypervascularization
- Bowing of tibia and femur - the classic orthopaedic deformity
- Gait abnormality and secondary osteoarthritis of hip/knee
- Back pain; spinal stenosis from vertebral overgrowth
- Leontiasis ossea (lion face) from skull/facial bone enlargement
- Skull enlargement → increased head size, kyphosis
- Platybasia (invagination of skull base) causing posterior fossa compression
- Deafness from temporal bone involvement (cochlear or ossicular compression)
- Chalk-stick (banana) fractures in long bones - horizontal transverse fractures (not oblique/spiral), typically in the lateral cortex of femur/tibia
Signs of hypervascularization:
- Warm skin overlying pagetic bone (increased local blood flow)
- High-output cardiac failure in severe polyostotic disease (arteriovenous shunt effect)

Severe Paget's disease - tibia is bowed, enlarged, and sclerotic with irregular thickening of both cortical and cancellous bone (Robbins Basic Pathology)
Investigations
| Investigation | Finding |
|---|---|
| Serum ALP | Elevated (best marker of disease activity) |
| Serum Ca²⁺ & PO₄ | Normal (usually) - may rise in immobilization |
| Urinary hydroxyproline / β-CTx | Elevated (markers of bone resorption) |
| Serum P1NP | Elevated (marker of bone formation) |
| X-ray | Bony enlargement, cortical thickening, mixed lytic/sclerotic, deformity |
| Bone scan | Most sensitive for extent of disease; "whole body" involvement mapping |
| CT/MRI | Assess complications (nerve compression, fractures, malignant transformation) |
Histopathology hallmark: Mosaic pattern of lamellar bone - haphazardly arranged cement lines producing a "jigsaw puzzle" pattern due to repeated cycles of disordered remodeling.
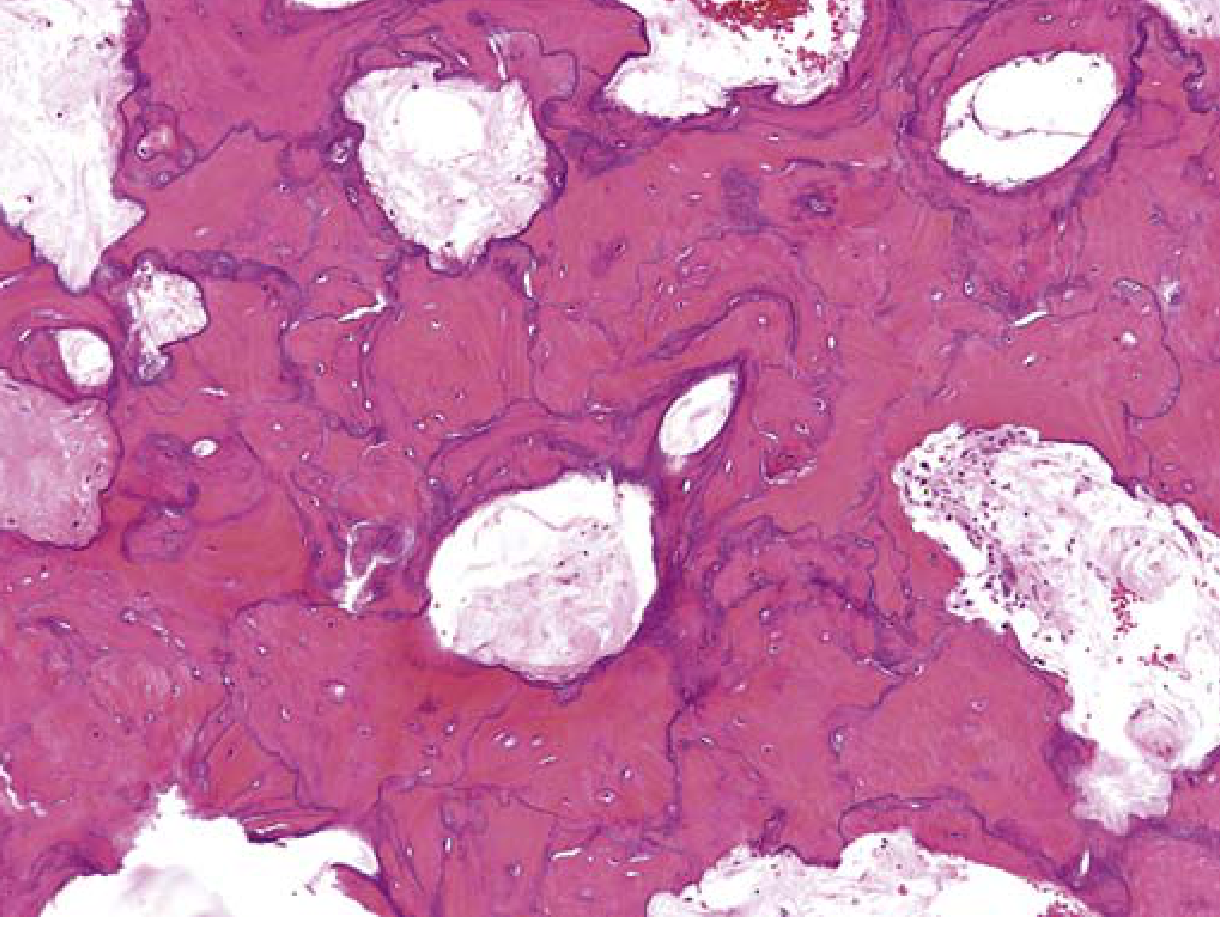
FIG. 19.10 (Robbins): Mosaic pattern of lamellar bone - pathognomonic of Paget's disease.
Complications
- Pathological fractures - chalk-stick / banana fractures; fractures heal normally
- Secondary osteoarthritis - from bony deformity distorting joint mechanics
- Nerve compression - deafness (VIII nerve), spinal stenosis, cranial nerve palsies
- High-output cardiac failure - in severe polyostotic disease
- Malignant transformation to osteosarcoma - <1% overall, but 5-10% in severe polyostotic disease; rapidly fatal; suspect if sudden increase in pain or ALP
Treatment
Indications for treatment: bone pain, nerve compression, prior to orthopedic surgery on pagetic bone, hypercalcemia of immobilization, prevention of progression.
| Drug | Mechanism | Notes |
|---|---|---|
| Bisphosphonates (1st line) | Inhibit osteoclast activity (reduce bone resorption) | Zoledronic acid IV (single infusion) most potent; alendronate, risedronate oral options |
| Calcitonin (2nd line) | Inhibits osteoclasts | Less potent; used if bisphosphonates contraindicated |
Surgical treatment:
- Fracture fixation (intramedullary nailing preferred)
- Osteotomy for severe deformity
- Joint replacement for secondary OA
- Pre-operative bisphosphonate to reduce hypervascularization before elective surgery on pagetic bone
Sources: Robbins & Kumar Basic Pathology (p.775-776); Harrison's Principles of Internal Medicine 22E (p.3355-3356); Miller's Review of Orthopaedics 9th Ed; Rockwood & Green's Fractures in Adults 10th Ed 2025
This is a shared conversation. Sign in to Orris to start your own chat.