Rheumatic heart disease pathology explain with pictures
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Finding Sources
Loading Image
I now have comprehensive textbook content and high-quality pathology images. Let me compile the full answer.
Rheumatic Heart Disease (RHD) - Pathology with Images
1. Overview
Rheumatic heart disease is the cardiac sequela of acute rheumatic fever (ARF), itself triggered by group A beta-hemolytic streptococcal pharyngitis. It is the leading cause of acquired valvular heart disease in children and young adults worldwide, especially in low- and middle-income countries. It predominantly causes deforming mitral stenosis - RHD is essentially the only cause of acquired mitral stenosis.
2. Pathogenesis - Molecular Mimicry
The immune response to Group A Streptococcus M-protein cross-reacts with host cardiac proteins:
- Antibodies against streptococcal M proteins also recognize cardiac myosin, laminin, and tropomyosin in the myocardium and valves
- These cross-reactive antibodies bind valvular endothelium, upregulating adhesion molecules (VCAM-1, ICAM-1) that facilitate CD4+ T cell infiltration into the valve
- Cytokines from T cells drive macrophage activation, forming Aschoff bodies
- The characteristic 2-3 week delay in symptom onset after infection reflects the time needed to generate this immune response - by this point, no live streptococci remain in the lesions
- Only ~1-3% of infected patients develop ARF, suggesting genetic susceptibility
3. Acute Rheumatic Fever - Pancarditis
ARF causes inflammation of all three heart layers (pancarditis):
Pericarditis
- Fibrinous exudate on pericardium
- Usually resolves without sequelae ("bread-and-butter" pericarditis)
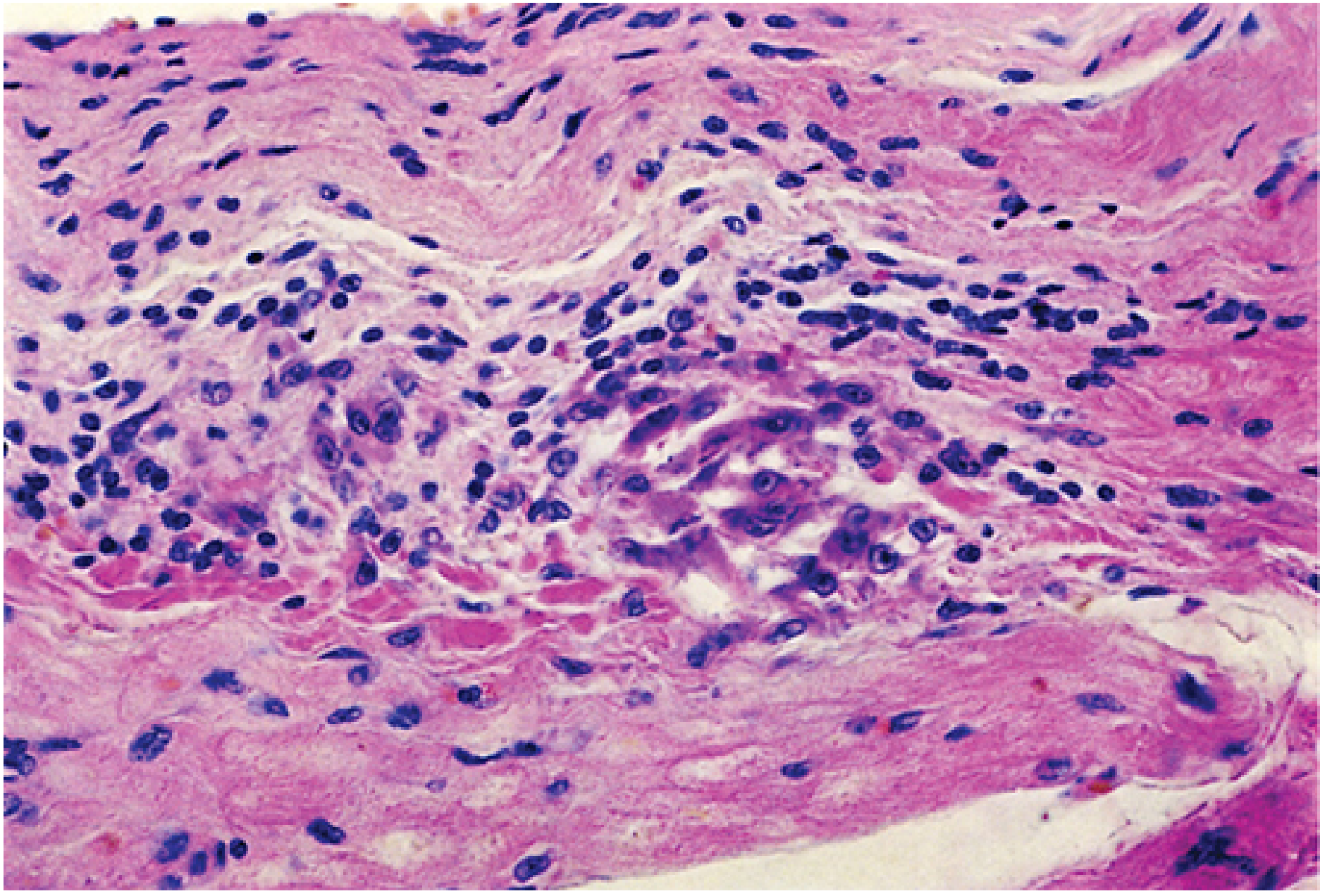
Myocarditis - Aschoff Bodies
The Aschoff body is the pathognomonic lesion of rheumatic fever:
- Collections of lymphocytes (mostly T cells), scattered plasma cells, and plump activated macrophages called Anitschkow cells (caterpillar cells)
- Anitschkow cells have abundant cytoplasm with nuclei showing centrally condensed chromatin in a wavy ribbon pattern - the "caterpillar nucleus"
- Zones of fibrinoid necrosis surround the cellular infiltrate
- Found in the interstitial connective tissue of the myocardium
Endocarditis / Valvulitis (Acute)
- Fibrinoid necrosis along the valve leaflet closure lines
- Formation of small 1-2 mm vegetations called verrucae along the lines of leaflet closure
- These vegetations cause little hemodynamic disturbance acutely
4. Gross and Microscopic Pathology - Key Images
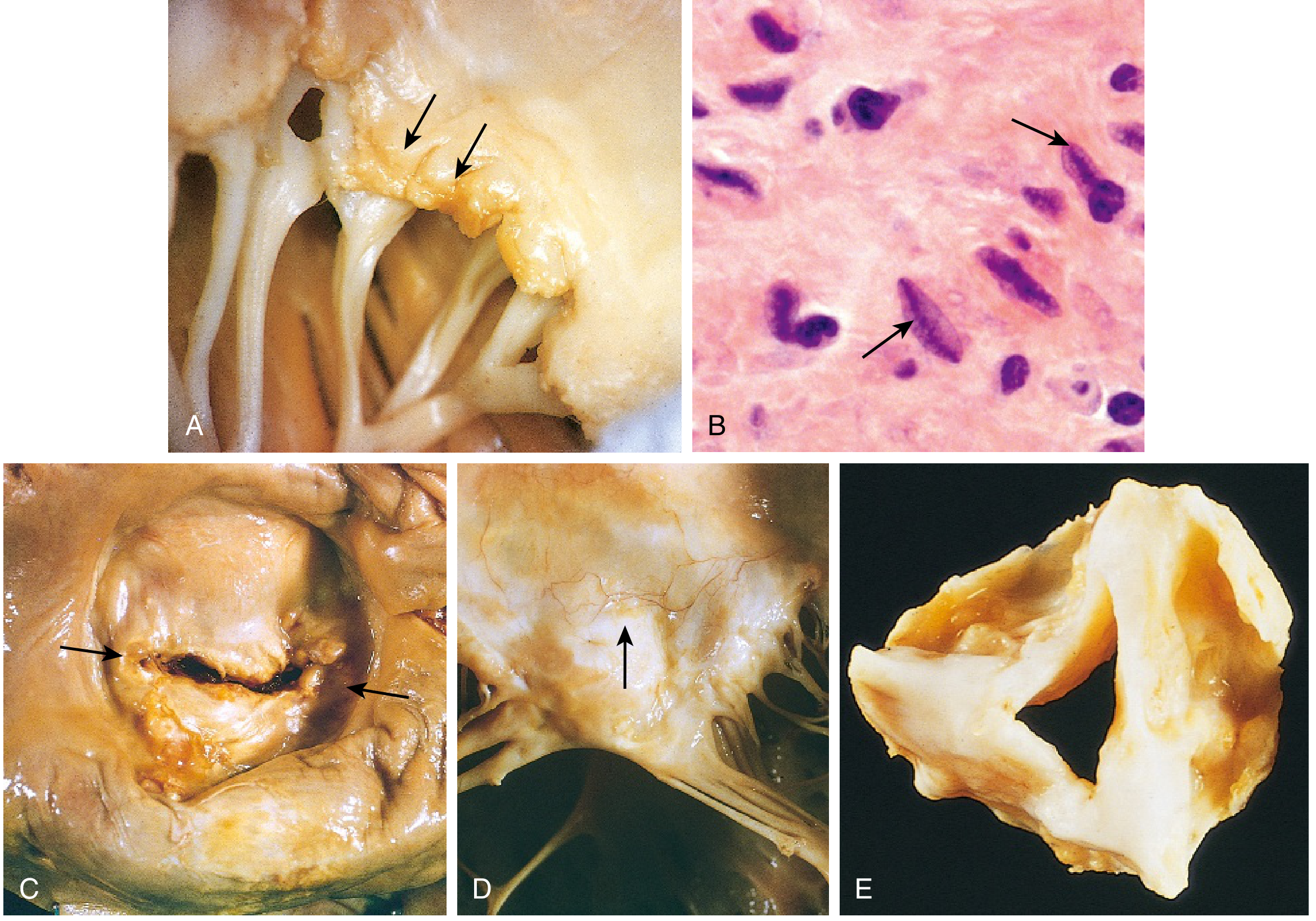
- (A) Acute rheumatic mitral valvulitis superimposed on chronic RHD - small verrucous vegetations visible along the line of leaflet closure (arrows); chordae tendineae already fibrous and fused from previous episodes
- (B) Microscopic Aschoff body - activated macrophages (Anitschkow cells) with prominent nucleoli and central wavy "caterpillar" chromatin (arrows)
- (C) Chronic mitral stenosis viewed from above - diffuse fibrous thickening, commissural fusion (arrows), and marked left atrial dilation
- (D) Anterior leaflet of rheumatic mitral valve showing neovascularization (arrow) - a hallmark of chronic inflammation/healing
- (E) Rheumatic aortic stenosis specimen - thickening and distortion of cusps
5. Chronic Rheumatic Heart Disease
As Aschoff bodies heal and scar, the valves undergo permanent destructive remodeling:
| Feature | Detail |
|---|---|
| Leaflet thickening | Fibrosis replaces normal leaflet architecture |
| Commissural fusion | Fibrous bridging between adjacent leaflets |
| Chordae tendineae | Thickening, shortening, and fusion |
| Calcification | Progressive; can create "buttonhole" stenosis |
| Neovascularization | New vessels in leaflets (grossly and microscopically visible) |
The "Fish Mouth" / "Buttonhole" Valve

6. Valves Affected - Order of Frequency
| Valve Involvement | Frequency |
|---|---|
| Mitral alone | ~70% of cases |
| Mitral + Aortic (combined) | ~25% of cases |
| Tricuspid | Less frequent, less severe |
| Pulmonic | Almost never affected ("escapes injury") |
The mitral valve is predominately affected because it bears the highest hemodynamic stress.
7. Consequences of Chronic RHD
Mitral stenosis is the dominant functional consequence:
- Left atrial dilation due to pressure overload from obstructed inflow
- Atrial fibrillation from atrial dilation and fibrosis
- Left atrial mural thrombus - from AF + dilation (risk of systemic embolism and stroke)
- Pulmonary hypertension from passive venous congestion
- Right ventricular hypertrophy and eventual failure
- Left ventricle is typically normal in pure mitral stenosis
8. Summary Diagram of Pathologic Progression
Group A Strep pharyngitis
↓
Molecular mimicry (M-protein vs. cardiac myosin/laminin)
↓
ACUTE RHEUMATIC FEVER (2-3 weeks later)
↓
PANCARDITIS
├── Pericarditis (fibrinous, usually resolves)
├── Myocarditis (Aschoff bodies + Anitschkow cells)
└── Valvulitis (verrucae on line of closure)
↓ (repeated attacks → progressive scarring)
CHRONIC RHD
├── Leaflet fibrosis and thickening
├── Commissural fusion → stenosis
├── Chordal fusion and shortening
└── "Fish mouth" mitral valve
↓
COMPLICATIONS
├── LA dilation → AF → thrombus → embolism
├── Pulmonary hypertension
└── Right heart failure
Sources: Robbins & Kumar Basic Pathology, pp. 366-367 | Sabiston Textbook of Surgery, p. 2535 | Firestein & Kelley's Textbook of Rheumatology, pp. 300-315 | Sherris & Ryan's Medical Microbiology
This is a shared conversation. Sign in to Orris to start your own chat.