Anal fissure
Reading File
Finding Sources
Searching PubMed
"anal fissure"[MeSH Terms] AND treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Searching Images
anal fissure anatomy diagram
Loading Image
Loading Image
Here is a comprehensive overview of anal fissure drawn from authoritative surgical and gastroenterology textbooks.
Anal Fissure
Definition
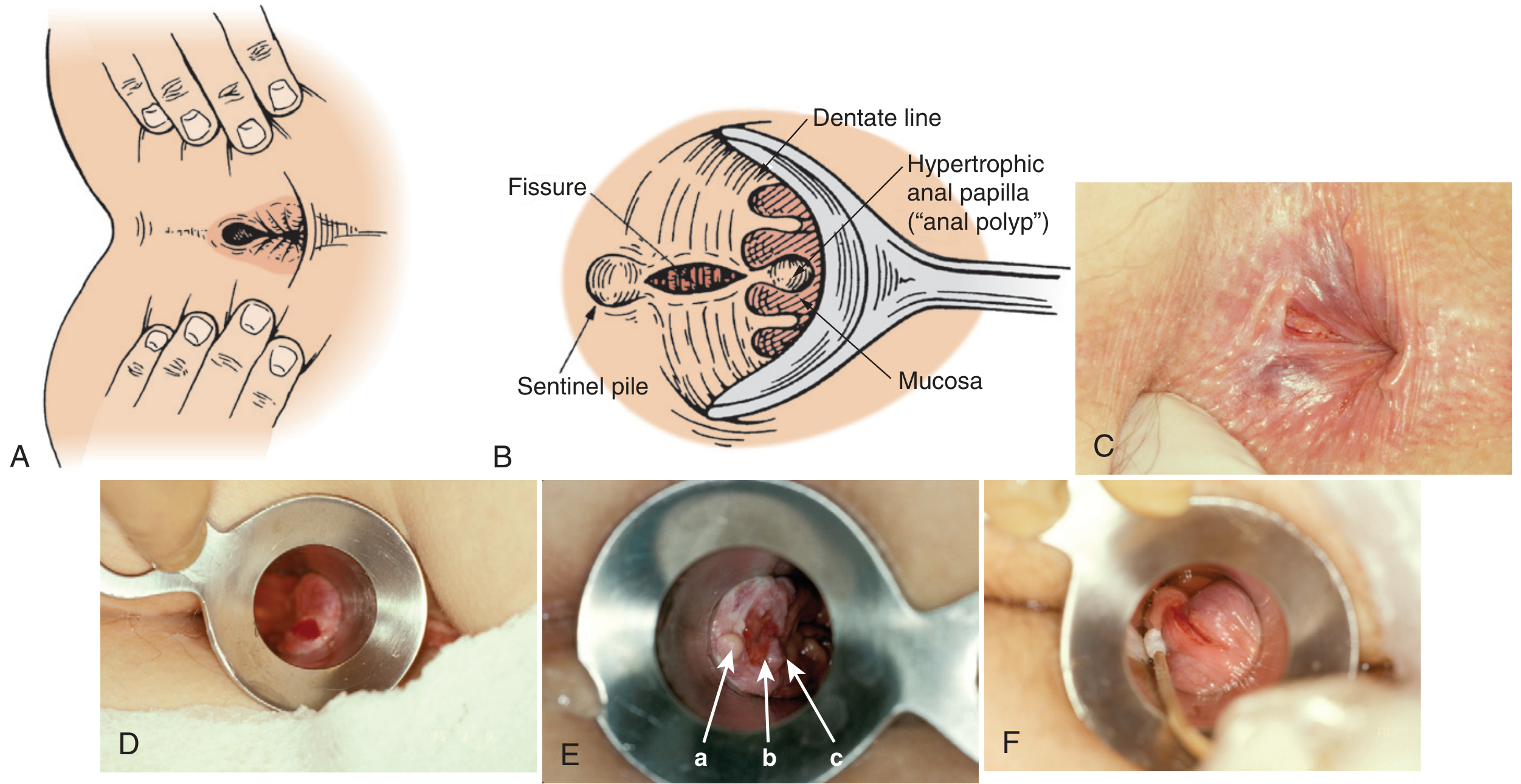
An anal fissure is a painful linear tear (ulcer) in the anoderm of the distal anal canal, beginning at the anal verge and extending proximally toward the dentate line.
Classification
| Feature | Acute | Chronic |
|---|---|---|
| Duration | < 6–8 weeks | > 6–8 weeks (some sources say > 3 months) |
| Appearance | Shallow tear in anoderm | Deep ulcer with exposed internal sphincter fibers at base |
| Associated findings | None | Sentinel pile (skin tag) distally + hypertrophied anal papilla proximally |
| Response to conservative Rx | Most heal | Only ~50% heal |
Pathophysiology
Trauma (hard stool, diarrhea, anal intercourse) → tear in anoderm → pain → internal anal sphincter (IAS) spasm → reduced blood flow → relative ischemia → impaired healing → further tearing. This pain–spasm–ischemia cycle perpetuates chronicity.
Location
- Posterior midline: ~75–90% of cases (relatively poor blood supply)
- Anterior midline: ~10%, more common in females
- Off midline (<1%): atypical — must exclude secondary causes
Atypical (off-midline) fissures raise concern for: Crohn's disease, anal cancer, tuberculosis, HIV, syphilis, herpes, leukemia.
Clinical Features
Symptoms:
- Severe, sharp anal pain with defecation — classically described as "passing razor blades" or "pieces of glass"
- Post-defecation throbbing and anal spasm lasting minutes to hours
- Bright-red rectal bleeding — typically mild, on toilet paper or streaking stool
- Chronic fissure: unrelenting pain; in severe cases, patients avoid eating to avoid defecation
Examination:
- Diagnosis is often made on history alone
- Gentle buttock separation may reveal the fissure or sentinel tag
- Focal pressure with a cotton-tip applicator at the posterior/anterior anal canal reproduces pain
- DRE and anoscopy are often deferred (too painful); markedly elevated sphincter tone is typical
- Examination under anesthesia (EUA) if diagnosis unclear or malignancy suspected

Management
Step 1 — Conservative (all fissures)
- High-fiber diet (≥30 g/day) + 6–8 glasses of water + fiber supplements (3–6 g/day)
- Warm sitz baths — pain relief in >90% of acute fissures
- 5% lidocaine ointment applied to the fissure (not via rectal tube or suppository)
- Stool softeners / bulk agents
- Commercially available anorectal creams: minimal benefit; steroids not for long-term use
- Avoid: rectal tube applicators, suppositories, anal dilators, silver nitrate, electrocautery
Step 2 — Pharmacological sphincter relaxants (for persistent/chronic fissures)
| Agent | Mechanism | Efficacy | Key Side Effect |
|---|---|---|---|
| Topical nitroglycerin (0.2–0.5%) | NO donor → IAS relaxation + vasodilation | ~50% healing | Severe headache; up to 20% stop therapy |
| Topical calcium channel blockers (diltiazem, nifedipine 2%) | IAS relaxation | Similar to NTG | Fewer headaches — preferred first-line topical |
| Topical bethanechol | Muscarinic agonist | Second-line | — |
| Topical arginine | NO donor | Second-line | — |
Topical diltiazem/nifedipine have no commercial US formulation — must be compounded.
Step 3 — Botulinum Toxin (BTX) injection
- Mechanism: blocks ACh release from presynaptic terminals → temporary IAS paralysis (~3 months)
- Dose: 20–100 IU
- Efficacy: similar to topical agents as first-line; modest improvement as second-line after failed topicals
- Side effects: transient flatus incontinence, rarely urinary retention, heart block, allergic reaction
- Can be done in-office or under sedation
Step 4 — Surgery: Lateral Internal Sphincterotomy (LIS)
The definitive treatment for chronic fissures failing medical therapy.
- Goal: divide ~30% of internal sphincter fibers laterally → reduce tone → promote healing
- Healing rate: 88–100% (superior to all medical therapies)
- Technique: open (radial incision exposing IAS) or closed (narrow-bladed scalpel via intersphincteric groove) — both have equivalent results
- Fecal incontinence risk: 8–30%, usually minor (flatus); most in first 30 days
- Avoid LIS in: baseline incontinence, females with obstetrical sphincter injuries, prior anorectal surgery, documented sphincter defects
Differential Diagnosis
- Hemorrhoids (distinguish by history; hemorrhoids rarely cause pain like fissures)
- Perianal abscess / fistula
- Crohn's disease perianal involvement
- Anal cancer / squamous cell carcinoma
- STIs: syphilis, herpes, gonorrhea, HIV-related ulcers
- Tuberculosis, leukemic infiltrates
Summary Algorithm
Anal fissure
│
├── Acute (<6–8 wk)
│ └── Conservative: fiber, sitz baths, topical lidocaine
│ ├── Heals → done
│ └── Fails → move to chronic protocol
│
└── Chronic (>6–8 wk)
├── Topical CCB (diltiazem/nifedipine) ← preferred first-line
├── Topical NTG (if CCB unavailable/failed)
├── BTX injection (second-line or office alternative)
└── LIS (gold standard if all else fails)
Sources: Sabiston Textbook of Surgery, 21e; Schwartz's Principles of Surgery, 11e; Pfenninger and Fowler's Procedures for Primary Care, 3e
This is a shared conversation. Sign in to Orris to start your own chat.