Young 20yr old patient palpitations
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
Finding Sources
Finding Sources
Loading Image
Reading File
I now have rich, authoritative content from Braunwald's, Harrison's, and Fuster's to build a thorough answer. Let me compile this into a well-structured response.
Palpitations in a 20-Year-Old: ECG Interpretation & Arrhythmias
First Step: What Are Palpitations Telling You?
Palpitations in a young patient are common and most often benign, but the ECG is your primary tool to rule out dangerous causes. The key question is: does this palpitation represent a life-threatening arrhythmia?
Low-risk features (generally benign):
- Isolated palpitations, not exercise-induced
- No structural heart disease
- No syncope or chest pain
- No family history of sudden cardiac death (SCD)
- Normal 12-lead ECG in sinus rhythm
Higher-risk features (warrant urgent workup):
- Syncope or presyncope with palpitations
- Exercise-triggered episodes
- Family history of sudden death in a young person
- Wide-complex tachycardia on ECG
- Associated chest pain or dyspnea
(Braunwald's Heart Disease, Assessment of the Patient with Palpitations)
The Most Common Arrhythmias in a Young Patient
1. Premature Beats (PACs / PVCs) - Most Common
The most frequent cause of palpitations. The patient feels a "skipped beat" - actually the forceful post-extrasystolic contraction after the compensatory pause, not the premature beat itself.
- ECG: Early beat (narrow = PAC, wide = PVC), followed by a pause
- Clinical course: Usually benign in a structurally normal heart
- Management: Reassurance; avoid triggers (caffeine, nicotine, stimulants)
2. AVNRT - Atrioventricular Nodal Reentrant Tachycardia (Most Common SVT)
The single most common cause of paroxysmal SVT in young people. Caused by a reentrant circuit within the AV node using a "dual pathway."
Typical presentation:
- Sudden onset, sudden termination ("like a light switch")
- Rapid heart rate 120-200 bpm (too fast to count)
- May respond to Valsalva maneuver
- Polyuria after termination (ANP release)
- Women are more commonly affected; often misdiagnosed as panic attacks
ECG features of typical (slow-fast) AVNRT:
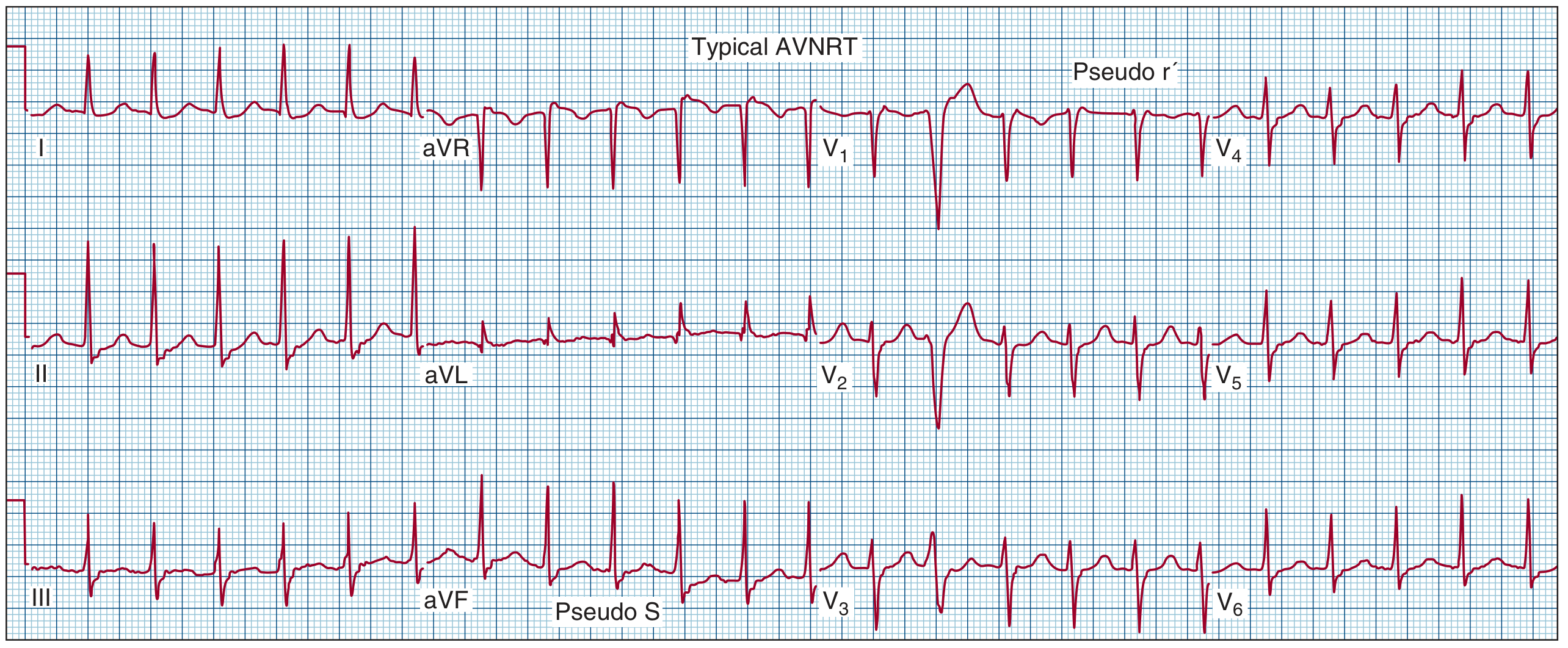
- Narrow QRS tachycardia, regular, rate 120-200 bpm
- P wave hidden within or just after QRS (short RP interval)
- Hallmark signs: pseudo r' in V1 and pseudo S in II, III, aVF - these are actually retrograde P waves buried at the end of the QRS
- RP interval < PR interval (fast retrograde = short RP)
(Fuster and Hurst's The Heart, 15th Ed, Clinical Features and ECG Characteristics)
3. AVRT / WPW Syndrome - Accessory Pathway Tachycardia
More common in young patients than older adults. An accessory pathway (bundle of Kent) bypasses the AV node. This matters because in AF with WPW, the accessory pathway can conduct at 250-300+ bpm and trigger ventricular fibrillation.
Sinus rhythm ECG findings (WPW pattern):
- Short PR interval (< 120 ms) - preexcitation
- Delta wave - slurred upstroke to QRS (earliest ECG clue)
- Widened QRS complex
- Secondary ST-T changes
During tachycardia:
- Orthodromic AVRT (most common): Narrow QRS, retrograde P after QRS (RP > 70 ms, distinguishes from AVNRT)
- Antidromic AVRT: Wide QRS (conduction down accessory path), regular - can mimic VT
DANGER SIGN: Irregular wide-complex tachycardia in a young patient = preexcited AF. Do NOT give AV nodal blocking drugs (adenosine, verapamil, digoxin) - these accelerate conduction through the accessory pathway and can cause VF.
4. Atrial Flutter / AF - Less Common in Young but Possible
- Flutter: Regular sawtooth P waves (300 bpm atrial rate), 2:1 or 3:1 block, ventricular rate ~150 bpm
- AF: Irregularly irregular rhythm, no distinct P waves, fibrillatory baseline
- In a young patient with AF, always look for an underlying cause: WPW, hyperthyroidism, alcohol, structural heart disease
5. Inherited Channelopathies - Must Not Miss
These cause life-threatening arrhythmias in otherwise healthy young people:
| Condition | ECG Clue | Arrhythmia Risk |
|---|---|---|
| Long QT Syndrome (LQTS) | QTc > 450 ms (men), > 460 ms (women) | Torsades de pointes, VF |
| Brugada Syndrome | Coved ST elevation in V1-V3 | VF, nocturnal sudden death |
| CPVT | Normal resting ECG | Exercise-triggered bidirectional VT |
| ARVC | Epsilon wave, T-wave inv V1-V3, LBBB morphology VT | VT/VF, especially with exercise |
(Braunwald's Heart Disease - Causes of Sudden Death; Goodman & Gilman's - Genetic Arrhythmia Diseases)
A family history of sudden unexplained death (especially in a young relative) should raise suspicion for these conditions immediately.
ECG Approach: Narrow vs. Wide Complex Tachycardia
Step 1: Is the QRS narrow (<120 ms) or wide (>=120 ms)?
Narrow QRS Tachycardia - origin is supraventricular:
- Look at P wave morphology and relation to QRS
- P before QRS with normal PR → sinus tachycardia or atrial tachycardia
- P buried in QRS / pseudo r' or S → AVNRT
- P just after QRS (short RP) → AVNRT or AVRT
- P well before next QRS (long RP) → atrial tachycardia or atypical AVNRT
- No P visible, irregular → AF
Wide QRS Tachycardia - treat as VT until proven otherwise:
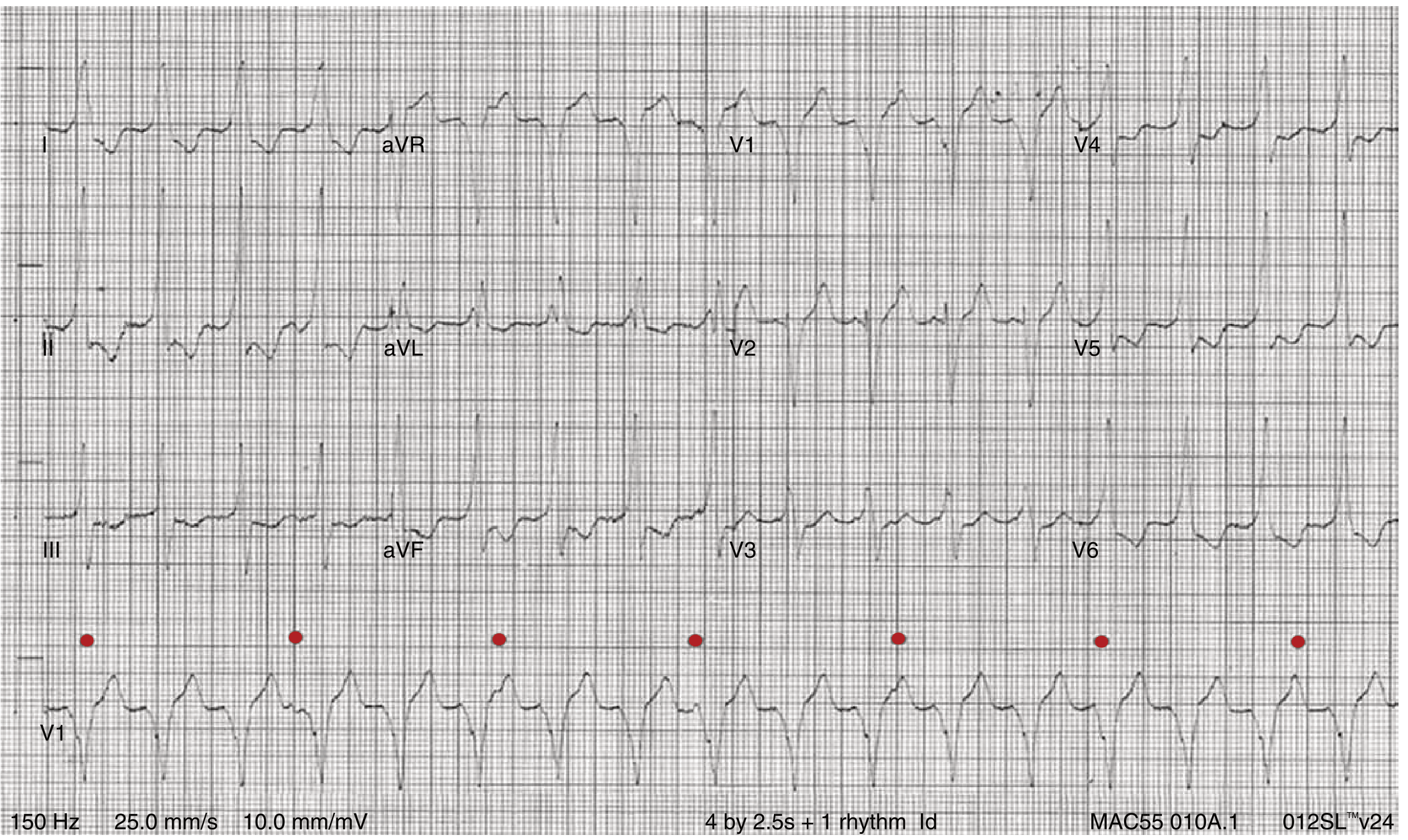
- AV dissociation (P waves independent of QRS, as shown above) = VT diagnosed
- Capture beats or fusion beats = VT
- Concordance in all precordial leads = VT
- Very broad QRS >160 ms = VT
- In a young patient with structural heart disease, VT must be actively excluded
(Braunwald's Heart Disease, Fig 61.2 - VT with AV dissociation; Harrison's Principles 22nd Ed)
Initial Workup
- 12-lead ECG in sinus rhythm - look for preexcitation (WPW), prolonged QT, Brugada pattern, ARVC changes
- Blood tests - TFTs, electrolytes (K+, Mg2+), FBC (anaemia)
- Echocardiogram - exclude structural heart disease (MVP, HCM, ARVC)
- Ambulatory monitoring:
- Daily symptoms: 24-48h Holter
- Weekly symptoms: 2-week event recorder
- Monthly or less: Implantable loop recorder
- Exercise ECG - if symptoms are exertional (rules out CPVT, ARVC)
Treatment Summary for AVNRT/AVRT (Most Likely in a 20-year-old)
| Setting | Treatment |
|---|---|
| Acute, stable | Valsalva maneuver → IV adenosine 6mg (then 12mg) |
| Acute, unstable | Synchronised DC cardioversion |
| Recurrent symptomatic | Catheter ablation (>95% success rate, first-line) |
| Medical suppression | Beta-blocker or non-DHP calcium channel blocker |
| WPW + AF | IV procainamide or ibutilide - NEVER adenosine/verapamil/digoxin |
(Braunwald's Heart Disease; Harrison's 22nd Ed, 2025)
Bottom line for a 20-year-old with palpitations: The most common ECG arrhythmia is AVNRT presenting as paroxysmal SVT. Your job is to rule out the dangerous mimics - WPW with AF, LQTS, Brugada, ARVC, and VT - using the 12-lead ECG in sinus rhythm and the clinical context. A normal sinus rhythm ECG does not exclude WPW (may need exercise testing or EP study) or channelopathies.
This is a shared conversation. Sign in to Orris to start your own chat.