Tell me about PCOD
Reading File
Finding Sources
Searching PubMed
polycystic ovary syndrome
Searching the Web
PCOD polycystic ovarian disease overview symptoms causes treatment 2025
Finding Sources
Reading Web Page
https://www.who.int/news-room/fact-sheets/detail/polycystic-…
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information from multiple authoritative textbooks. Let me compile the full answer.
Polycystic Ovarian Disease (PCOD) / Polycystic Ovary Syndrome (PCOS)
A note on terminology: "PCOD" (Polycystic Ovarian Disease) and "PCOS" (Polycystic Ovary Syndrome) are commonly used interchangeably. Clinically, PCOS is the preferred term because the condition is a hormonal syndrome - not all women with it have visible cysts, and having cysts alone does not mean you have PCOS.
What Is It?
PCOS is one of the most common endocrine disorders in women of reproductive age, affecting 5-10% of women worldwide (a 2024 meta-analysis [PMID: 38922413] puts global prevalence even higher). It was first described in 1935 by Stein and Leventhal as the association of amenorrhea, bilateral polycystic ovaries, and obesity.
The core features are:
- Hyperandrogenism (HA) - excess male hormones (clinical or biochemical)
- Ovarian dysfunction - irregular/absent ovulation (oligo- or anovulation)
- Polycystic ovarian (PCO) morphology on ultrasound
It is the most common cause of hirsutism, hyperandrogenism, and anovulatory infertility in developed countries. - Berek & Novak's Gynecology, p. 1919
Causes & Pathophysiology
The exact cause is unknown, but three major mechanisms interact:
1. Hormonal Dysregulation
- The hypothalamic-pituitary axis releases LH in excess relative to FSH
- Elevated LH stimulates ovarian theca cells to overproduce androgens (testosterone, androstenedione)
- This androgen excess disrupts normal follicle development, preventing ovulation
2. Insulin Resistance (IR)
- 65-95% of women with PCOS have insulin resistance and compensatory hyperinsulinemia
- Insulin directly enhances theca cell androgen production (in collaboration with LH)
- Insulin also inhibits the liver's synthesis of Sex Hormone-Binding Globulin (SHBG), increasing free (bioavailable) testosterone
- IR is not just a consequence of obesity - a specific defect in insulin receptor signaling (diminished autophosphorylation) is found in ~50% of PCOS women regardless of weight - Berek & Novak's Gynecology, p. 1927
3. Genetic Factors
- PCOS is inherited as a complex polygenic/multifactorial trait
- Candidate genes include: CYP11A, CYP17, insulin receptor locus (19p13.3), SHBG, IRS-1, IRS-2, TCF7L2, and follistatin
- Theca cells from PCOS women show overexpression of steroidogenic enzymes (CYP11A, 3βHSD2, CYP17), leading to excess testosterone production
Symptoms
Symptoms vary widely from person to person:
| Category | Symptoms |
|---|---|
| Menstrual | Irregular, infrequent, or absent periods (oligomenorrhea/amenorrhea); heavy or painful periods |
| Hyperandrogenic | Hirsutism (excess facial/body hair - occurs in ~70% of US patients); acne and oily skin; male-pattern hair thinning or baldness |
| Metabolic | Weight gain (especially abdominal); acanthosis nigricans (a skin marker of insulin resistance) |
| Reproductive | Difficulty conceiving; infertility |
| Psychological | Anxiety, depression, negative body image |
PCOS typically begins at or near puberty with hirsutism and irregular menses from the time of menarche. In some cases, it can emerge in adulthood alongside the development of obesity. - Goldman-Cecil Medicine
Diagnostic Criteria
PCOS is diagnosed using the Rotterdam 2003 Criteria - 2 out of 3 of the following, after excluding other causes:
- Oligoovulation or anovulation
- Clinical and/or biochemical signs of hyperandrogenism
- Polycystic ovaries on ultrasound
Ultrasound criteria: ≥20 follicles in either ovary measuring 2-9 mm in diameter, and/or ovarian volume >10 mL. A single ovary meeting these criteria is sufficient.
Here is the diagnostic algorithm from Berek & Novak's Gynecology:
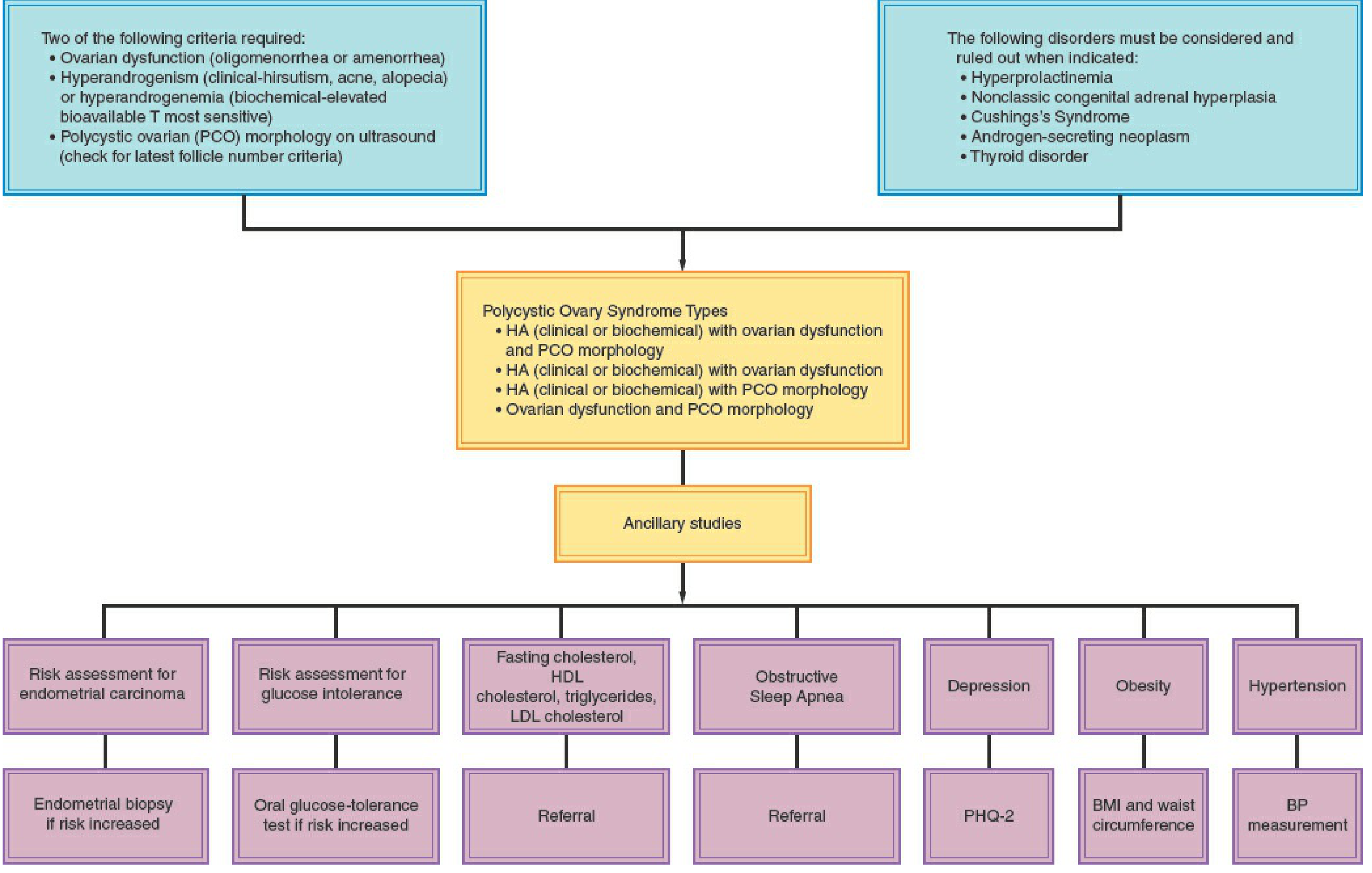
Conditions that must be ruled out before diagnosing PCOS:
- Hyperprolactinemia
- Non-classic congenital adrenal hyperplasia (CAH) - measure basal 17-OHP level
- Cushing's syndrome
- Androgen-secreting neoplasm (adrenal or ovarian)
- Thyroid disorder
Anti-Mullerian Hormone (AMH) has emerged as a reliable biomarker - elevated levels reflect the increased small antral follicle count in PCOS. A 2024 meta-analysis ([PMID: 38944177]) confirmed its value as a diagnostic biomarker, particularly for polycystic ovarian morphology.
Associated Health Risks
PCOS is far more than a reproductive condition. Long-term risks include:
- Type 2 diabetes: 30-45% of obese women with PCOS have glucose intolerance or frank diabetes
- Cardiovascular disease: dyslipidemia, hypertension, atherosclerosis risk
- Metabolic syndrome: diagnosed when 3 of 5 criteria are met (waist >88 cm, TG >150, HDL <50, BP >130/85, fasting glucose 110-126 mg/dL)
- Endometrial hyperplasia/cancer: due to prolonged anovulation causing unopposed estrogen exposure
- Obstructive sleep apnea (especially with obesity)
- Pregnancy complications: gestational diabetes, gestational hypertension, preeclampsia, preterm birth, early miscarriage
- Mental health: significantly increased rates of anxiety and depression
Investigations / Workup
| Test | Purpose |
|---|---|
| Serum testosterone, DHEAS, androstenedione | Confirm biochemical hyperandrogenism |
| LH:FSH ratio | Often elevated (>2:1), though not diagnostic |
| Pelvic ultrasound | Assess ovarian morphology |
| 75 g OGTT (2-hour) | Screen for glucose intolerance/diabetes (preferred over HbA1c alone) |
| Fasting lipid profile | Cardiovascular risk assessment |
| 17-OHP (follicular phase) | Exclude non-classic CAH |
| TSH, prolactin | Exclude thyroid disease and hyperprolactinemia |
| Blood pressure at each visit | Hypertension screening |
Treatment
Treatment is tailored to the individual's goals and symptoms.
For Women NOT Seeking Pregnancy
- Combined oral contraceptive pills (COCPs) - first-line: regulate periods, suppress ovarian androgen production, increase SHBG. Allow 6 months before assessing response for hirsutism/acne.
- Antiandrogens (spironolactone, flutamide): added if inadequate response to COCPs at 6 months
- Progestins (medroxyprogesterone, progesterone, levonorgestrel IUD): endometrial protection against hyperplasia from anovulation
- Metformin: recommended for overweight/obese women to prevent cardiometabolic risk; not recommended alone for hyperandrogenic symptoms or endometrial protection - Harrison's Principles of Internal Medicine 22e
For Women Seeking Pregnancy
- Letrozole (aromatase inhibitor) - first-line for ovulation induction
- Clomiphene citrate (with or without metformin) - selective estrogen receptor modulator; second-line
- Injectable gonadotropins - used carefully by experienced practitioners due to risk of ovarian hyperstimulation syndrome (OHSS)
- Preconception counseling and lifestyle management are strongly advised
Lifestyle Management (All Women With PCOS)
A 2025 systematic review ([PMID: 39861440]) confirms that lifestyle interventions are the cornerstone of PCOS management:
- Weight loss of ≥5-10% in overweight/obese women significantly reduces testosterone, improves SHBG, restores ovulatory function, and reduces IR (a 10 kg weight loss reduces insulin levels by ~40%)
- Structured exercise independently improves insulin resistance
- Behaviour modification and stress management enhance success
- For BMI >40 (or >35 with high-risk conditions), bariatric surgery can be considered
Monitoring Recommendations
All women with PCOS should be screened at diagnosis and at regular intervals for:
- Obesity (BMI and waist circumference)
- Hypertension (blood pressure at every visit)
- Glycaemic control (OGTT preferred over HbA1c)
- Dyslipidaemia (fasting lipid profile; repeat every 2 years if normal)
- Depression and anxiety (PHQ-2 or equivalent)
- Endometrial hyperplasia risk
PCOD vs PCOS: Are They the Same?
Clinically, yes - these terms refer to the same condition. "PCOD" is an older or more colloquial term, particularly common in South Asia, while "PCOS" is the internationally preferred medical term. The distinction matters because:
- Not everyone with PCOS has visible cysts (the follicles are immature, not true cysts)
- The syndrome is fundamentally hormonal, not structural
Sources: Berek & Novak's Gynecology; Harrison's Principles of Internal Medicine 22E; Goldman-Cecil Medicine; WHO PCOS Fact Sheet; PMID: 38922413; PMID: 38944177; PMID: 39861440
This is a shared conversation. Sign in to Orris to start your own chat.