Here is a comprehensive gynaecology reference covering all conditions you listed, organized by etiology, pathophysiology, diagnosis, and treatment.
Inflammatory Diseases of the Female Reproductive Tract
PART I — PELVIC INFLAMMATORY DISEASE (PID) & ITS COMPONENTS
Overview of PID
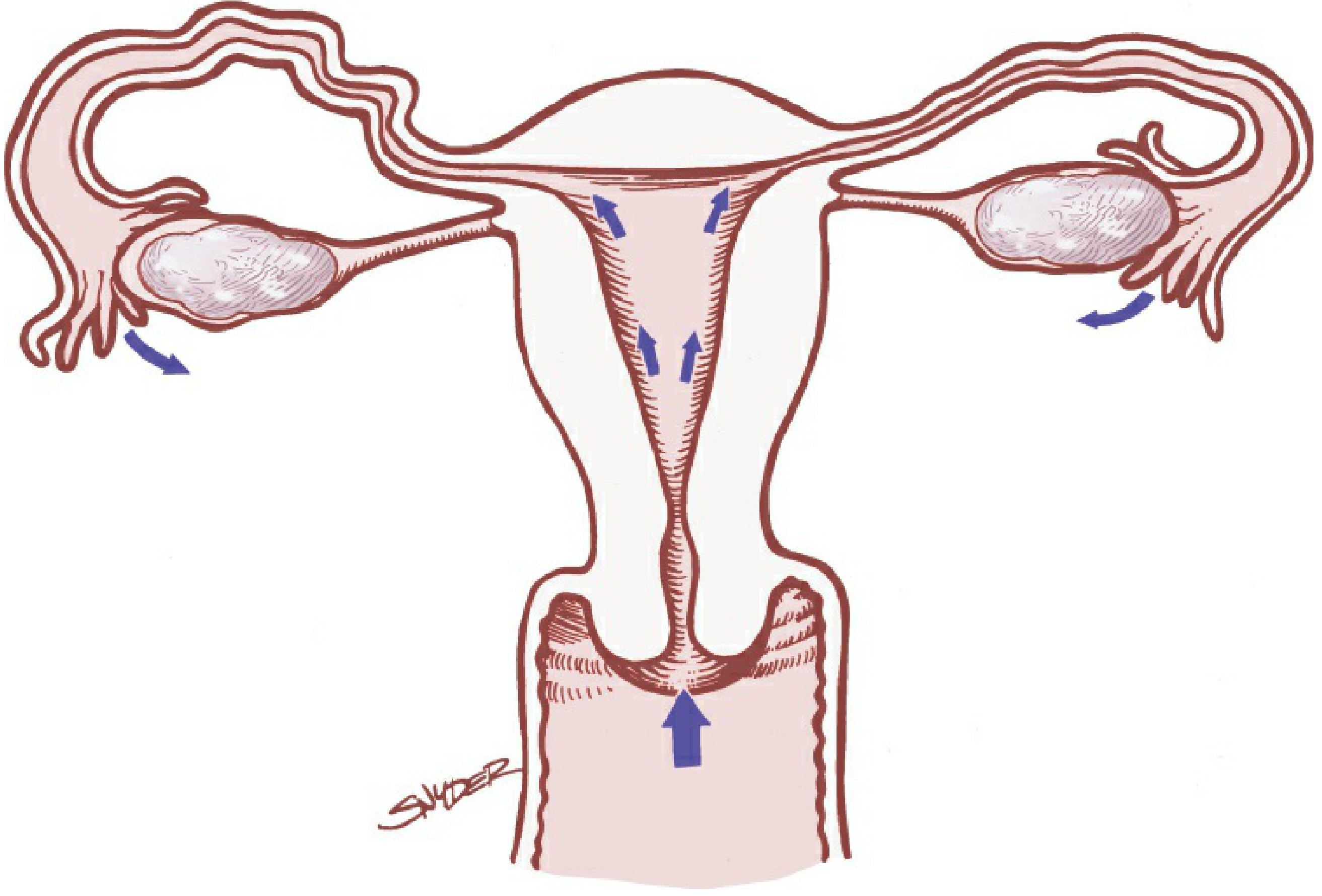
Pelvic inflammatory disease refers to ascending infection from the cervix or vagina to involve the endometrium and/or fallopian tubes. Infection can extend beyond the reproductive tract to cause pelvic peritonitis, generalized peritonitis, perihepatitis, perisplenitis, or pelvic abscess.
Fig. 15-1 — Micro-organisms originating in the endocervix ascend into the upper reproductive tract. (Berek & Novak's Gynecology)
1. Etiology of PID
| Organism | Role |
|---|
| Neisseria gonorrhoeae | Primary cause; dominant in high-incidence settings |
| Chlamydia trachomatis | Primary cause; immunopathology drives damage |
| Mycoplasma genitalium | Increasingly recognised; associated with endometritis & salpingitis |
| Anaerobes (Prevotella spp., peptostreptococci) | 1/4 to 1/3 of cases, especially in BV-associated PID |
| Facultative organisms (E. coli, H. influenzae, Group B Strep) | Polymicrobial contribution |
Risk factors: endocervical infection or BV, recent IUD insertion, vaginal douching, menstruation (facilitates ascending spread), multiple sexual partners. Oral contraceptives are protective. Tubal sterilisation prevents salpingitis.
2. Cervicitis
Etiology:
- The cervix has two epithelial zones. The ectocervical squamous epithelium is susceptible to Trichomonas vaginalis, Candida, and HSV. The endocervical glandular epithelium is specifically targeted by N. gonorrhoeae and C. trachomatis.
- C. trachomatis accounts for ~40% of cervicitis cases in STI clinics.
Pathophysiology:
- Infection causes mucopurulent endocervical discharge. Friability of the ectropion (zone of ectopy) is a hallmark. Inflammatory cells (neutrophils) flood the submucosa and glandular epithelium.
- Untreated, infection ascends into the uterus and tubes.
Diagnosis:
- Yellow-green "mucopus" on endocervical swab against a white background
- Gram stain: >30 neutrophils/HPF; intracellular gram-negative diplococci = presumptive gonorrhoea; if negative = presumptive chlamydial cervicitis
- NAAT (nucleic acid amplification test) on vaginal/endocervical swab — gold standard for N. gonorrhoeae, C. trachomatis, and T. vaginalis
- Mycoplasma genitalium detected in 10–30% of clinical cervicitis
Treatment:
| Organism | Regimen |
|---|
| N. gonorrhoeae | Ceftriaxone 500 mg IM single dose |
| C. trachomatis | Doxycycline 100 mg PO BD × 7 days, OR Azithromycin 1 g PO single dose |
| Dual therapy (both) | Ceftriaxone + Doxycycline (standard empiric approach) |
Concurrent BV must be treated, as it sustains cervicitis if left unaddressed. All sexual partners must receive equivalent treatment.
3. Endometritis
Etiology: Ascending infection from cervicitis (gonorrhoea, chlamydia, M. genitalium, anaerobes). Can be iatrogenic — following D&C, IUD insertion, hysterosalpingography, termination of pregnancy, or parturition (postpartum endometritis).
Pathophysiology:
- Organisms breach the cervical barrier and invade endometrial glands and stroma
- Neutrophilic infiltration of the endometrium; plasma cells in the stroma on histopathology are the hallmark of chronic endometritis
- Menstruation facilitates ascent by disrupting the cervical mucus plug
Clinical features: Uterine tenderness, abnormal uterine bleeding, purulent discharge. Less fever and peritoneal signs than salpingitis — this differentiates isolated endometritis from higher ascent.
Diagnosis: Endometrial biopsy showing histopathologic evidence of inflammation (plasma cell stromal infiltration); NAAT for gonorrhoea/chlamydia.
Treatment: Same antibiotic regimen as PID (see below).
4. Urethritis
Etiology: N. gonorrhoeae, C. trachomatis, Ureaplasma urealyticum, Trichomonas vaginalis.
Pathophysiology: Direct infection of urethral mucosa; in women, often co-exists with cervicitis. Urethral discharge, dysuria. The infection is frequently asymptomatic.
Diagnosis: NAAT on urine (first-catch) or urethral swab; Gram stain (intracellular diplococci for gonorrhoea).
Treatment: Ceftriaxone 500 mg IM + Doxycycline 100 mg BD × 7 days (covers both gonorrhoea and chlamydia).
5. Cystitis (in the context of PID spectrum)
Etiology in STI context: Typically E. coli (commonest overall), but Chlamydia trachomatis and N. gonorrhoeae can cause urethritis mimicking cystitis. True cystitis from STIs is uncommon; it is usually ascending bacteriuria.
Pathophysiology: Bacteria colonise the periurethral area, ascend the urethra, adhere to urothelium via fimbriae/pili, trigger an inflammatory response.
Diagnosis: Urinalysis (pyuria, bacteriuria, nitrites), urine culture and sensitivity, NAAT if STI suspected.
Treatment: Nitrofurantoin 100 mg BD × 5 days or Trimethoprim 200 mg BD × 7 days for uncomplicated cystitis. Adjust if STI aetiology confirmed.
6. Salpingitis
Etiology: N. gonorrhoeae, C. trachomatis, M. genitalium, anaerobes (Prevotella, peptostreptococci), E. coli.
Pathophysiology:
- Organisms ascend from the endometrium into the fallopian tube lumen
- Acute: intense neutrophilic infiltration of the tubal mucosa and wall → mucosal destruction, tubal adhesions
- Chlamydial salpingitis involves immunopathology — repeated exposure triggers greatest tissue damage, even with minimal symptoms
- Chronic/recurrent: fibrosis → tubal occlusion → infertility or ectopic pregnancy
- Progression: pyosalpinx (pus-filled tube) → tubo-ovarian abscess (TOA)
Diagnosis:
- Clinical: adnexal tenderness + cervical motion tenderness + uterine tenderness (CDC minimum criteria)
- Elevated CRP/ESR, leukocytosis, fever
- Transvaginal ultrasound (TVUS): thickened, fluid-filled tubes; TOA
- Laparoscopy: gold standard (tubal erythema, oedema, purulent exudate)
- NAAT for N. gonorrhoeae, C. trachomatis
Treatment: See PID treatment table below.
Sequelae:
- Infertility (tubal occlusion): 11% after 1 episode → 23% after 2 → 54% after 3+ episodes
- Ectopic pregnancy: 7× increased risk
- Chronic pelvic pain
- Recurrent PID
7. Oophoritis
Etiology: Usually an extension of salpingitis — gonorrhoea, chlamydia, anaerobes. Rarely haematogenous spread (mumps oophoritis).
Pathophysiology: Direct extension from inflamed tube → ovarian surface → cortical infiltration by neutrophils. Can form tubo-ovarian complex with adherent tube and ovary or progress to true TOA.
Diagnosis: TVUS showing complex adnexal mass; CT scan for TOA delineation. NAAT for causative organisms.
Treatment: Same as PID (broad-spectrum antibiotics including anaerobic cover).
8. Salpingo-Oophoritis (Tubo-Ovarian Disease)
The combined inflammation of both fallopian tube and ovary. This is the most advanced local form of PID before peritonitis.
Tubo-Ovarian Abscess (TOA): A serious complication. Requires IV antibiotics (Regimen B: Clindamycin + Gentamicin preferred for anaerobic coverage). Drainage via posterior colpotomy or CT-guided aspiration if no response in 72 h. Surgery (salpingo-oophorectomy) reserved for life-threatening rupture.
PID Treatment Summary Table
| Setting | Regimen |
|---|
| Outpatient | Ceftriaxone 500 mg IM once + Doxycycline 100 mg PO BD × 14 days + Metronidazole 500 mg PO BD × 14 days |
| Inpatient – Regimen A | Cefotetan 2 g IV q12h OR Cefoxitin 2 g IV q6h + Doxycycline 100 mg IV/PO q12h |
| Inpatient – Regimen B | Clindamycin 900 mg IV q8h + Gentamicin (2 mg/kg loading, then 1.5 mg/kg q8h) |
Indications for hospitalisation: Uncertain diagnosis (exclude appendicitis/ectopic), pregnancy, suspected abscess, severe illness/vomiting, HIV infection, failed outpatient therapy, adolescents (some guidelines).
Source: Harrison's Principles of Internal Medicine 22E (2025); Berek & Novak's Gynecology
PART II — SEXUALLY TRANSMITTED INFECTIONS (STIs)
1. Chlamydia trachomatis
Etiology: Obligate intracellular gram-negative bacterium. Serovars D–K cause genital tract disease.
Pathophysiology:
- Infects only columnar/transitional epithelium (endocervix, fallopian tubes, urethra, rectum)
- Elementary bodies (EB) — infectious, extracellular — attach to and enter epithelial cells
- Reticulate bodies (RB) — intracellular, replicating form — replicate inside inclusions then release new EBs
- Host immune response (especially CD4+ T cells) drives inflammation; repeated infection causes progressive tubal scarring more than primary infection
- Most infections are asymptomatic in women (~70–80%)
Clinical features: Mucopurulent cervicitis, urethritis, PID, perihepatitis (Fitz-Hugh–Curtis syndrome), infertility
Diagnosis: NAAT (urine or vaginal/endocervical swab) — gold standard. Culture rarely used. Serology not useful for acute infection.
Treatment:
- First-line: Doxycycline 100 mg PO BD × 7 days (preferred)
- Alternative: Azithromycin 1 g PO single dose
- Treat sexual partners. Test of cure if symptoms persist.
2. Neisseria gonorrhoeae
Etiology: Gram-negative diplococcus. Infects only glandular/columnar epithelium.
Pathophysiology:
- Pili (fimbriae) mediate attachment to non-ciliated columnar epithelial cells
- Endocytosis → intracellular replication → release through basolateral surface → local spread
- Lipooligosaccharide (LOS) triggers intense neutrophilic inflammation → purulent discharge
- IgA protease evades mucosal immunity
- High rates of antibiotic resistance (fluoroquinolone resistance now widespread)
Clinical features: Purulent cervicitis, urethritis, bartholin gland abscess, PID, disseminated gonococcal infection (DGI — septic arthritis, skin lesions, tenosynovitis)
Diagnosis:
- NAAT — gold standard
- Gram stain: intracellular gram-negative diplococci (less sensitive in women)
- Culture on Thayer-Martin medium (chocolate agar + antibiotics) — needed for sensitivity testing
Treatment:
- Ceftriaxone 500 mg IM single dose (1 g if weight >150 kg)
- Dual therapy with Doxycycline if chlamydia not excluded
- No fluoroquinolones — widespread resistance
- No longer use cefixime as first-line (increasing resistance)
3. Candida albicans
Etiology: Dimorphic fungus; part of normal vaginal flora. Vulvovaginal candidiasis (VVC) occurs when host defences are altered.
Pathophysiology:
- Predisposing factors: antibiotics (disturb normal lactobacilli flora), diabetes mellitus, pregnancy, immunosuppression (HIV, corticosteroids), OCP use
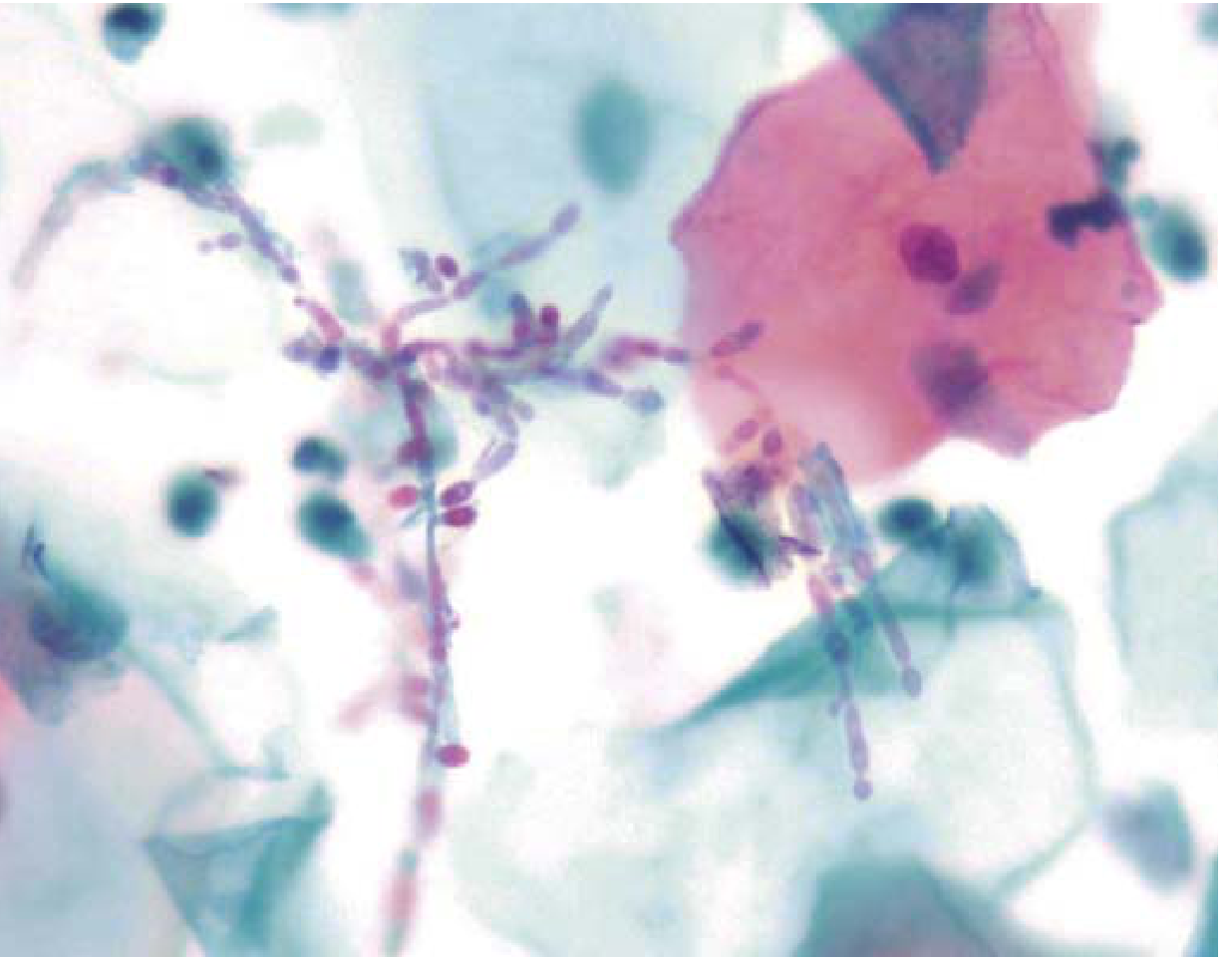
- Transition from yeast to hyphal/pseudohyphal form — invasive form that penetrates epithelium
- Adhesins (Als proteins) bind to vaginal epithelial cells → triggers host inflammatory cascade → intense pruritus, erythema
Papanicolaou test showing Candida hyphal forms (pseudohyphae and budding yeast). (Robbins & Kumar Basic Pathology)
Clinical features: Intense vulvovaginal pruritus, thick "cottage cheese" curdy white discharge (non-offensive), dyspareunia, erythema, satellite lesions
Diagnosis:
- Vaginal pH: <4.5 (normal — distinguishes from BV and trichomoniasis)
- Wet mount/KOH prep: pseudohyphae and budding yeast
- Culture on Sabouraud's agar
- NAAT available
Treatment:
- Uncomplicated: Clotrimazole intravaginal (1–3 days) or Fluconazole 150 mg PO single dose
- Recurrent (≥4 episodes/year): Fluconazole 150 mg PO weekly × 6 months
- Complicated/severe: Fluconazole 150 mg PO q72h × 3 doses
- Avoid in pregnancy: use only topical azoles
4. Trichomonas vaginalis
Etiology: Flagellated protozoan. The most common curable STI worldwide.
Pathophysiology:
- Attaches to vaginal epithelium via surface lectins and adhesins
- Triggers neutrophilic inflammation; disrupts vaginal lactobacilli → raises pH
- Produces cysteine proteinases and ROS that damage epithelial cells
- Increases HIV susceptibility (mucosal disruption and inflammation)
Diagnosis:
- Vaginal pH: >4.5
- Wet mount: motile trichomonads (pear-shaped, flagellated organisms, characteristic oval nucleus and red cytoplasmic granules — see eFig. 17.3 in Robbins)
- NAAT: highest sensitivity/specificity (gold standard)
- Pap smear may show organisms incidentally
Treatment:
- Metronidazole 2 g PO single dose (or 500 mg BD × 7 days)
- Tinidazole 2 g PO single dose (better tolerated)
- Treat sexual partners simultaneously
- Avoid alcohol during and 24–72 h after metronidazole/tinidazole
5. Human Immunodeficiency Virus (HIV)
Etiology: RNA retrovirus (lentivirus). HIV-1 (global pandemic); HIV-2 (West Africa, less virulent).
Pathophysiology:
- Sexual transmission via mucosal route — virus enters via micro-abrasions or directly through M-cells/dendritic cells in genital mucosa
- Targets CD4+ T lymphocytes, macrophages, and dendritic cells via gp120 binding to CD4 + CCR5/CXCR4 co-receptors
- Reverse transcriptase converts RNA → DNA → integrates into host genome (provirus)
- Progressive CD4+ depletion → AIDS (CD4 <200/μL) → opportunistic infections
- STIs (especially ulcerative ones — HSV, syphilis) dramatically increase HIV transmission per act
Gynaecological manifestations: Recurrent/severe VVC, HPV-related cervical dysplasia (accelerated), PID (more severe, higher TOA rate), abnormal menstruation
Diagnosis:
- 4th-generation HIV Ag/Ab combo test (detects p24 antigen + antibodies) — screening
- Confirmatory: HIV-1/2 antibody differentiation immunoassay
- RNA viral load (PCR) — monitors treatment response and acute infection
- CD4+ count — staging
Treatment:
- Antiretroviral therapy (ART) — initiated immediately upon diagnosis regardless of CD4 count
- Standard first-line: Tenofovir + Emtricitabine + Dolutegravir (or Bictegravir)
- Pre-exposure prophylaxis (PrEP): Tenofovir/Emtricitabine for high-risk HIV-negative individuals
- Post-exposure prophylaxis (PEP): within 72 hours of exposure × 28 days
6. Human Papillomavirus (HPV)
Etiology: Double-stranded DNA virus. >200 genotypes. In gynaecology:
- High-risk (oncogenic): Types 16 & 18 — 70% of cervical carcinomas and CIN
- Low-risk: Types 6 & 11 — genital condylomata (warts), no malignant potential
Pathophysiology:
- HPV infects immature squamous cells at the transformation zone (squamocolumnar junction) of the cervix
- High-risk HPV proteins E6 (binds p53 → degradation; upregulates telomerase) and E7 (binds RB → releases E2F → cell cycle progression) disable tumour suppressors
- High-risk HPV integrates into the host genome → genomic instability → CIN → invasive carcinoma
- Low-risk HPV remains episomal (no integration) → condylomata without malignant transformation
- Most HPV infections are transient and cleared by immune response within months; persistent infection → CIN
Diagnosis:
- Pap smear (cervical cytology): koilocytes (perinuclear halo + nuclear atypia), dyskaryosis
- HPV DNA test / HPV genotyping (co-test with Pap)
- Colposcopy + directed biopsy for CIN confirmation
- Visual inspection with acetic acid (VIA): acetowhite areas
Treatment:
- No antiviral treatment for HPV itself
- CIN 1: Observation (often regresses spontaneously)
- CIN 2/3: LLETZ/LEEP (loop excision) or cone biopsy
- Condylomata: Podophyllin, trichloroacetic acid, imiquimod cream, cryotherapy
- Prevention: HPV vaccine (9-valent Gardasil — covers types 6, 11, 16, 18, 31, 33, 45, 52, 58); recommended for ages 9–26; most effective before sexual debut
7. Herpes Simplex Virus (HSV)
Etiology: HSV-2 — primary cause of genital herpes (also HSV-1 increasingly). HSV-2 accounts for the majority of genital ulcers in industrialised countries.
Pathophysiology:
- After primary infection, HSV travels via sensory nerve axons to sacral dorsal root ganglia (S2–S4) → establishes latency
- Reactivation: virus travels back along peripheral nerves → recurrent genital lesions
- Maternal–neonatal transmission during vaginal delivery → potentially fatal neonatal herpes
- HSV ulcers significantly increase susceptibility to and transmission of HIV
- Recurrence is more frequent and severe with HSV-2; HSV-1 genital infections recur less
Clinical features:
| Phase | Features |
|---|
| Primary | Painful grouped vesicles/ulcers, inguinal lymphadenopathy, systemic flu-like symptoms, dysuria, urinary retention |
| Recurrent | Milder ulcers, shorter duration, preceded by prodrome (tingling/burning) |
| Asymptomatic | Viral shedding without lesions — major source of transmission |
Diagnosis:
- PCR of lesion swab — gold standard (most sensitive)
- Viral culture (Tzanck smear — multinucleated giant cells, less sensitive)
- Type-specific serology (IgG): HSV-1 vs HSV-2 antibodies — useful for counselling
- NAAT is preferred over culture
Treatment:
| Indication | Regimen |
|---|
| Primary episode | Aciclovir 400 mg TDS × 7–10 days OR Valaciclovir 1 g BD × 7–10 days |
| Recurrent episode | Aciclovir 800 mg TDS × 5 days OR Valaciclovir 500 mg BD × 3 days |
| Suppressive therapy | Valaciclovir 500 mg OD daily (reduces recurrence by ~70%) |
| Neonatal risk (late pregnancy) | Aciclovir 400 mg TDS from 36 weeks; caesarean delivery if active lesions at onset of labour |
Quick Comparison Summary
| STI | Organism | Discharge | pH | Key Diagnostic Test | Treatment |
|---|
| Gonorrhoea | N. gonorrhoeae | Purulent, yellow-green | Normal | NAAT / Gram stain | Ceftriaxone 500 mg IM |
| Chlamydia | C. trachomatis | Mucopurulent or none | Normal | NAAT | Doxycycline 7 days |
| Candidiasis | C. albicans | White, curdy, thick | <4.5 | KOH prep (pseudohyphae) | Fluconazole 150 mg PO |
| Trichomoniasis | T. vaginalis | Frothy, yellow-green | >4.5 | NAAT / Wet mount (motile flagellates) | Metronidazole 2 g PO |
| HSV | Herpes simplex virus | None (ulcers) | — | PCR of lesion swab | Aciclovir/Valaciclovir |
| HPV | Human papillomavirus | None (warts/CIN) | — | Pap smear + HPV DNA test | LLETZ / Vaccine |
| HIV | HIV-1/2 | — | — | 4th-gen Ag/Ab combo test | ART (TDF + FTC + DTG) |
Sources: Harrison's Principles of Internal Medicine 22E (2025); Berek & Novak's Gynecology; Robbins & Kumar Basic Pathology 10E