Beta blockers from shanbagh
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the content needed. Let me compile the comprehensive beta blockers notes.
Note: Shanbhag's Review of Pharmacology is not in the library. The notes below are drawn from Katzung's Basic and Clinical Pharmacology, 16th Edition (Chapter 10: Adrenoceptor Antagonist Drugs) - the standard pharmacology reference that covers identical content to Shanbhag's beta blocker chapter.
Beta Blockers (β-Adrenoceptor Antagonist Drugs)
Chemical Structures
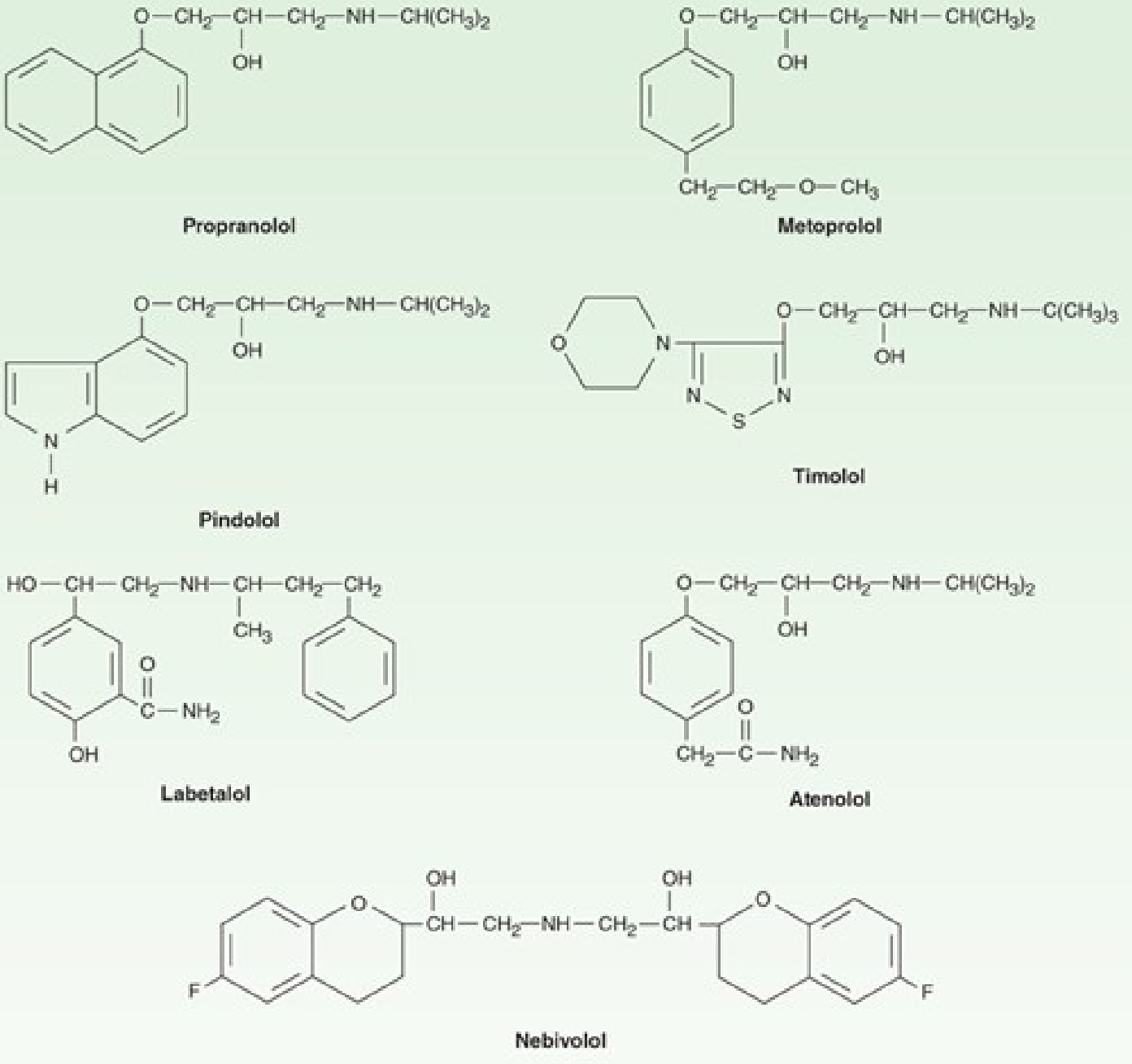
All beta blockers structurally resemble isoproterenol (their chemical template), though they have opposite actions.
Classification
By Receptor Selectivity
| Group | Drugs | Feature |
|---|---|---|
| Non-selective (β1 + β2) | Propranolol, Timolol, Nadolol, Pindolol, Sotalol | Block both β1 and β2 |
| β1-Selective (cardioselective) | Atenolol, Metoprolol, Bisoprolol, Acebutolol, Esmolol, Betaxolol, Nebivolol | Preferential β1 blockade; selectivity is dose-dependent and NOT absolute |
| α + β blockers (mixed) | Labetalol, Carvedilol | Also block α1-adrenoceptors → vasodilation |
By Intrinsic Sympathomimetic Activity (ISA / Partial Agonist Activity)
- With ISA (partial agonists): Pindolol, Acebutolol, Penbutolol, Carteolol, Oxprenolol, Celiprolol
- Without ISA: Propranolol, Atenolol, Metoprolol, Timolol, Nadolol, Bisoprolol, Esmolol, Carvedilol, Nebivolol
Drugs with ISA are less likely to cause bradycardia and adverse plasma lipid changes, but their overall clinical advantage remains uncertain.
By Membrane Stabilizing Activity (MSA / Local Anesthetic Effect)
- With MSA: Propranolol, Acebutolol, Pindolol
- Without MSA: Timolol, Atenolol, Metoprolol, Nadolol, Esmolol
Timolol's lack of MSA makes it preferred for ophthalmic (glaucoma) use - corneal anesthesia is undesirable.
Pharmacokinetic Properties
| Property | Details |
|---|---|
| Absorption | Most are well absorbed orally; peak levels at 1-3 hours |
| Bioavailability | Propranolol has extensive first-pass hepatic metabolism → low (~30%) and highly variable oral bioavailability; betaxolol, penbutolol, pindolol, and sotalol have better bioavailability |
| Distribution | Propranolol is highly lipid-soluble → crosses BBB → useful for migraine, anxiety, tremor |
| Metabolism | Atenolol is renally cleared → dose adjustment needed in renal failure; esmolol is hydrolyzed by RBC esterases → t½ ~10 min |
| Duration | Nadolol has the longest duration of action among this class |
Pharmacodynamics
A. Cardiovascular Effects
- Heart: Negative inotropic + negative chronotropic effects (reduces heart rate and contractility). Prolongs AV node conduction → increased PR interval.
- Blood Pressure: Lowers BP in hypertensive patients via: (1) reduced cardiac output, (2) suppression of renin release, (3) CNS effects. Does NOT cause hypotension in normotensive individuals.
- Peripheral Resistance: Acutely may rise (due to unopposed α-mediated vasoconstriction); falls chronically due to renin suppression.
- Vasodilation exception: Labetalol and Carvedilol cause vasodilation via α1 blockade. Nebivolol causes vasodilation by promoting endothelial nitric oxide (NO) production.
B. Respiratory Effects
- β2 blockade → bronchoconstriction → dangerous in asthma
- β1-selective drugs (metoprolol, atenolol) are safer but not absolutely β1-specific; still generally avoided in asthma
- May be used cautiously in COPD (moderate)
C. Metabolic Effects
- Mask signs of hypoglycemia (tachycardia, tremor) in diabetics - sweating is preserved
- Non-selective agents impair glycogenolysis → prolonged hypoglycemia
- Adverse effects on plasma lipids (except nebivolol, which does not adversely affect lipid profile and may increase insulin sensitivity)
D. Other Effects
- CNS: Lipid-soluble drugs (propranolol) enter CNS → useful for anxiety, tremor, migraine prophylaxis
- Eye: Reduce intraocular pressure by decreasing aqueous humor production (ciliary body is cAMP-dependent)
- Thyroid: β blockers reduce peripheral conversion of T4 to T3; control sympathetic symptoms of hyperthyroidism
E. Effects NOT Related to Beta Blockade
- Membrane stabilizing (local anesthetic) activity: Propranolol
- Partial agonism (ISA): Pindolol, acebutolol, penbutolol
- Inverse agonism: Betaxolol, metoprolol (stabilize inactive β receptor conformation)
- Antioxidant / anti-mitogenic (vascular): Carvedilol - independent of adrenoceptor blockade, contributes to benefit in heart failure
- Ion channel blockade: Sotalol - Class III antiarrhythmic action (IKr blockade) in addition to β blockade
Clinical Uses
| Indication | Key Drugs | Notes |
|---|---|---|
| Hypertension | Atenolol, Metoprolol, Carvedilol | Not first-line for uncomplicated essential HTN; preferred when heart failure, CAD, or post-MI coexist |
| Ischemic Heart Disease / Angina | Metoprolol, Atenolol, Timolol | First-line for stable angina; reduce cardiac O2 demand |
| Acute MI | Metoprolol, Atenolol, Timolol | Reduce infarct size + acute mortality; used chronically post-MI |
| Cardiac Arrhythmias | Esmolol (acute), Sotalol, Propranolol | Slow ventricular rate in AF/flutter; suppress catecholamine-induced ectopics; esmolol for perioperative arrhythmias |
| Heart Failure (chronic) | Metoprolol, Bisoprolol, Carvedilol | Only these three proven to reduce mortality in HFrEF |
| Hypertrophic Obstructive Cardiomyopathy | Propranolol | Slows ejection → reduces outflow obstruction |
| Dissecting Aortic Aneurysm | Propranolol, Esmolol | Reduce aortic wall stress |
| Glaucoma | Timolol, Betaxolol, Levobunolol | Topical; reduce aqueous humor production |
| Hyperthyroidism | Propranolol | Controls palpitations, tachycardia, tremor; also inhibits T4→T3 conversion |
| Migraine prophylaxis | Propranolol, Timolol | CNS-penetrating drugs preferred |
| Essential tremor | Propranolol | |
| Anxiety / situational tremor | Propranolol | |
| Pheochromocytoma | Only AFTER alpha blockade | Beta blockers ALONE are contraindicated - can cause severe HTN crisis from unopposed α stimulation |
| Portal hypertension / varices | Propranolol, Nadolol | Reduce portal pressure |
Contraindications
- Asthma / bronchospasm - absolute contraindication (non-selective especially)
- Bradycardia, AV block (2nd/3rd degree) - risk of complete heart block
- Acute decompensated heart failure - can worsen acutely (though used chronically in stable HF)
- Pheochromocytoma without prior α blockade
- Prinzmetal's (vasospastic) angina - unopposed α-mediated coronary spasm
- Hypotension / cardiogenic shock
- Peripheral arterial disease (relative) - reduces blood flow
Toxicity / Adverse Effects
- Bradycardia, AV block
- Acute cardiac decompensation in patients with underlying HF (especially at initiation)
- Bronchospasm (particularly non-selective agents)
- Fatigue, lethargy, depression (especially lipid-soluble agents, e.g., propranolol)
- Sexual dysfunction
- Cold extremities (from peripheral vasoconstriction)
- Hypoglycemia and masking of its symptoms in diabetics
- Rebound hypertension / angina on abrupt withdrawal - must taper gradually
- Plasma lipid changes (increased triglycerides, reduced HDL) - spared by nebivolol
Individual Drug Highlights (Exam-Important Points)
| Drug | Key Feature |
|---|---|
| Propranolol | Prototype; non-selective; high lipid solubility; highest first-pass metabolism; used for most indications |
| Atenolol | β1-selective; renal excretion (dose adjust in renal failure); longer acting |
| Metoprolol | β1-selective; used in HF (mortality benefit); sustained-release available |
| Bisoprolol | β1-selective; proven mortality benefit in HF |
| Carvedilol | Non-selective β + α1 blocker; antioxidant properties; proven mortality benefit in HF; metabolized by CYP2D6 (interactions with quinidine, fluoxetine) |
| Labetalol | α1 + β blocker (racemic mixture); used in hypertensive emergencies in pregnancy |
| Nebivolol | Most selective β1 blocker; vasodilation via NO release; no adverse lipid/metabolic effects |
| Esmolol | Ultra-short acting (t½ ~10 min); IV only; hydrolyzed by RBC esterases; perioperative arrhythmias/HTN |
| Pindolol | Highest ISA; also 5-HT1A antagonist (may potentiate antidepressants) |
| Sotalol | Non-selective β blocker + Class III antiarrhythmic (IKr blockade); risk of torsades de pointes |
| Timolol | Non-selective; no MSA; topical glaucoma treatment; also post-MI mortality reduction |
| Nadolol | Longest duration of action; renal excretion |
| Acebutolol | β1-selective + ISA + MSA; also has antiarrhythmic properties |
Key Points for MCQs
- Prototype = Propranolol
- Only β1-selective drugs for heart failure with proven mortality benefit: Metoprolol, Bisoprolol (+ Carvedilol which is non-selective)
- Drug of choice in pregnancy-related hypertension: Labetalol (α+β blocker)
- Ultra-short acting β blocker: Esmolol (t½ 10 min, RBC esterase metabolism)
- Longest acting: Nadolol
- Most β1-selective: Nebivolol
- NO-mediated vasodilation: Nebivolol
- Only β blocker used in glaucoma without corneal anesthesia risk: Timolol (no MSA)
- Pheochromocytoma: Alpha blockade FIRST, then beta blockade
- Abrupt withdrawal causes rebound HTN and angina - always taper
- Sotalol = β blocker + Class III antiarrhythmic; risk of torsades
- Sweating is preserved even when β blockers mask other hypoglycemia symptoms
- ISA drugs: Pindolol > Acebutolol > Penbutolol > Carteolol (less bradycardia, less lipid changes)
Source: Katzung's Basic and Clinical Pharmacology, 16th Edition, Chapter 10 - Adrenoceptor Antagonist Drugs
This is a shared conversation. Sign in to Orris to start your own chat.