Hey 👋
Hey! How can I help you today?
Can you give me 10 most common heart disease with ecg
Reading File
Finding Sources
Finding Sources
Searching Images
ECG electrocardiogram heart disease patterns common
Finding Sources
Finding Sources
Searching Images
atrial fibrillation ECG 12 lead
Searching Images
STEMI ST elevation myocardial infarction ECG
Searching Images
complete heart block third degree AV block ECG
Searching Images
Wolff-Parkinson-White syndrome delta wave ECG
Searching Images
ventricular tachycardia VT ECG wide complex tachycardia
Searching Images
left ventricular hypertrophy ECG Sokolow-Lyon criteria
Searching Images
pulmonary embolism ECG S1Q3T3 right heart strain
I now have excellent ECG images for all 10 conditions. Here's a comprehensive guide:
10 Most Common Heart Diseases & Their ECG Findings
1. 🫀 ST-Elevation Myocardial Infarction (STEMI)
ECG Hallmarks:
- ST-segment elevation ≥1 mm in ≥2 contiguous leads (convex/tombstone morphology)
- Hyperacute T-waves (tall, peaked) — earliest sign
- Reciprocal ST depression in opposing leads
- Pathological Q waves develop within hours (necrosis marker)
- Lead localization: V1–V4 = anterior (LAD); II, III, aVF = inferior (RCA); I, aVL, V5–V6 = lateral (LCx)

2. 🫀 Non-ST Elevation ACS / Unstable Angina (NSTEMI/UA)
ECG Hallmarks:
- ST-segment depression (horizontal or downsloping) — most common
- T-wave inversions — symmetric, deep (especially lateral leads)
- Wellens' syndrome (critical LAD stenosis): biphasic or deeply inverted T-waves in V2–V3 with no ST elevation
- No pathological Q waves (no transmural necrosis)
- Normal ECG possible in up to 5% of NSTEMIs
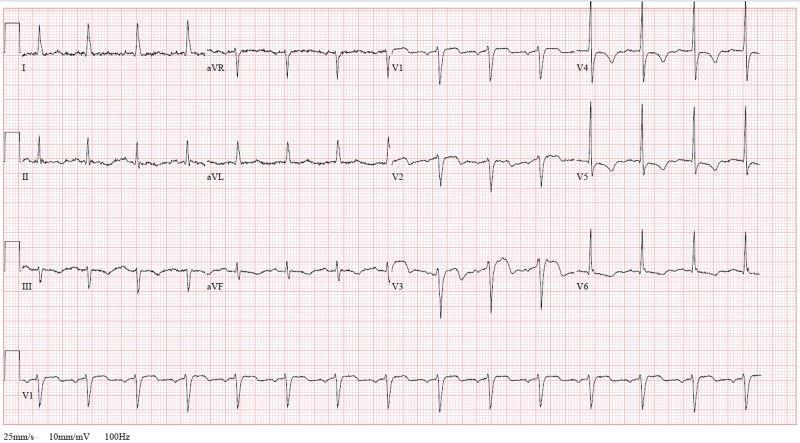
3. 🫀 Atrial Fibrillation (AF)
ECG Hallmarks:
- Absent P waves — replaced by fine irregular fibrillatory (f) waves, best seen in V1
- Irregularly irregular RR intervals — the hallmark finding
- Narrow QRS (unless aberrant conduction or pre-existing BBB)
- Rate may be: controlled (<100 bpm) or rapid ventricular response (>100 bpm)

4. 🫀 Complete (Third-Degree) AV Heart Block
ECG Hallmarks:
- Complete AV dissociation — P waves and QRS complexes are completely independent
- Regular P-P intervals and regular RR intervals, but no fixed PR relationship
- Slow escape rhythm: narrow QRS (junctional, 40–60 bpm) or wide QRS (ventricular, 20–40 bpm)
- P waves "march through" QRS complexes without conducting

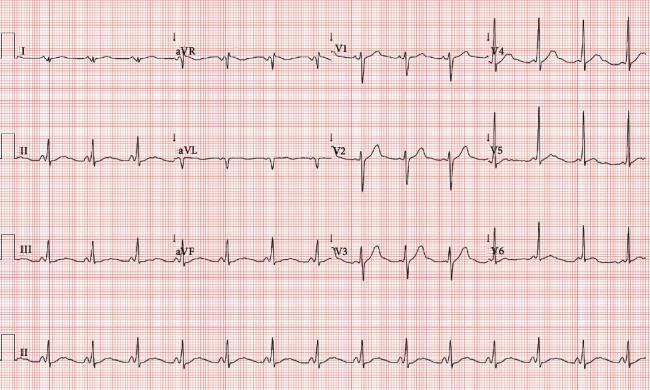
5. 🫀 Left Ventricular Hypertrophy (LVH) / Hypertensive Heart Disease
ECG Hallmarks:
- High-voltage QRS: Sokolow-Lyon criteria — S in V1 + R in V5/V6 ≥35 mm
- Cornell criteria: R in aVL + S in V3 ≥28 mm (men) / ≥20 mm (women)
- LV strain pattern: ST depression + T-wave inversion in I, aVL, V5–V6
- Left axis deviation
- Caused by: hypertension, aortic stenosis, HCM
6. 🫀 Ventricular Tachycardia (VT)
ECG Hallmarks:
- Wide complex tachycardia (QRS >120 ms) at rate 100–250 bpm
- AV dissociation — P waves independent of QRS (pathognomonic of VT)
- Fusion beats and capture beats (strong VT indicators)
- Concordance across precordial leads (all positive or all negative)
- Axis deviation (often northwest axis)
- Brugada criteria help distinguish VT from SVT with aberrancy

7. 🫀 Wolff-Parkinson-White (WPW) Syndrome
ECG Hallmarks (classic triad):
- Short PR interval (<120 ms) — rapid conduction via accessory pathway (Bundle of Kent)
- Delta wave — slurred, slow upstroke at the beginning of QRS
- Wide QRS complex (>120 ms) due to ventricular pre-excitation
- Secondary ST/T-wave changes (discordant to QRS)
- Can mimic STEMI or LBBB; risk of sudden death with AF
8. 🫀 Pulmonary Embolism (PE) / Acute Cor Pulmonale
ECG Hallmarks:
- S1Q3T3 pattern — S wave in lead I, Q wave in lead III, T-wave inversion in lead III (classic but only ~20% sensitive)
- Sinus tachycardia — most common finding
- Right heart strain: T-wave inversions in V1–V4
- Incomplete/complete RBBB — sudden right ventricular pressure overload
- Rightward axis deviation

9. 🫀 Left Bundle Branch Block (LBBB)
ECG Hallmarks:
- Wide QRS (≥120 ms)
- Broad, notched ("M-shaped") R waves in I, aVL, V5–V6
- Deep rS or QS pattern in V1
- Absence of septal Q waves in lateral leads
- Discordant ST/T changes (ST and T in opposite direction to QRS)
- New LBBB + chest pain = STEMI equivalent (Sgarbossa criteria apply)
(LBBB is commonly caused by CAD, cardiomyopathy, hypertension, aortic stenosis)
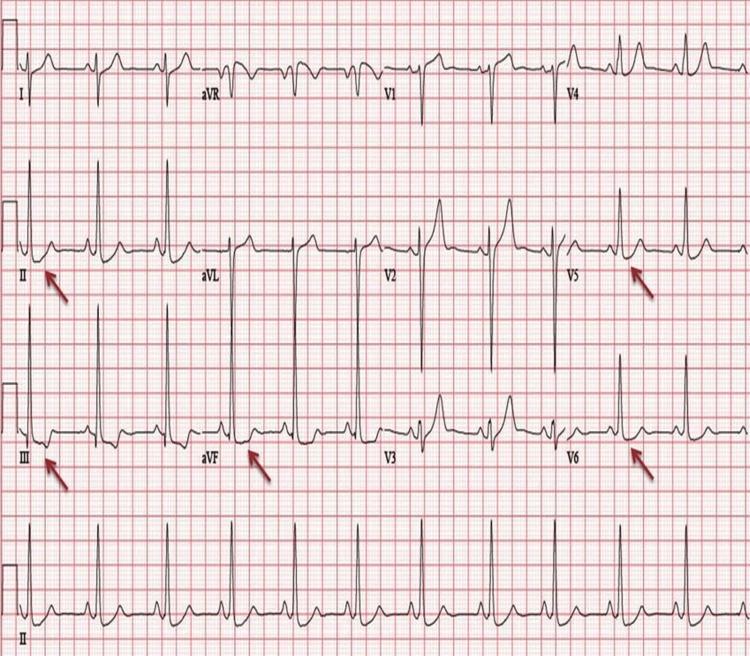
10. 🫀 Pericarditis
ECG Hallmarks (evolve through 4 stages):
- Stage 1: Diffuse, saddle-shaped (concave) ST elevation in most leads; PR depression (hallmark); ST elevation in aVR is absent/depressed
- Stage 2: ST returns to baseline; T-waves flatten
- Stage 3: T-wave inversions (widespread)
- Stage 4: Normalization
- Key distinction from STEMI: diffuse (not regional), concave elevation, PR depression, no reciprocal changes (except aVR)
(Large effusion/tamponade may show electrical alternans — alternating QRS height)
Quick Reference Summary Table
| # | Condition | Key ECG Pattern |
|---|---|---|
| 1 | STEMI | ST elevation, Q waves, reciprocal changes |
| 2 | NSTEMI/UA | ST depression, T inversions, Wellens' pattern |
| 3 | Atrial Fibrillation | Absent P waves, irregularly irregular |
| 4 | 3rd Degree AV Block | Complete AV dissociation, escape rhythm |
| 5 | LVH / HTN Heart Dz | High voltage, strain pattern (ST↓ + T inv lateral) |
| 6 | Ventricular Tachycardia | Wide QRS, AV dissociation, fusion beats |
| 7 | WPW Syndrome | Short PR, delta wave, wide QRS |
| 8 | Pulmonary Embolism | S1Q3T3, sinus tach, RBBB, RV strain |
| 9 | LBBB | Wide QRS, M-shaped R wave in laterals, rS in V1 |
| 10 | Pericarditis | Diffuse concave ST elevation, PR depression |
Clinical tip: Always interpret ECGs in the clinical context. A single ECG finding rarely makes a diagnosis alone — correlate with history, symptoms, and other investigations.
This is a shared conversation. Sign in to Orris to start your own chat.