Congenital heart disease
Reading File
Asking for Preferences
Pathology mbbs
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Reading File
I now have comprehensive content from both Robbins textbooks. Let me compose the complete MBBS-level pathology answer.
Congenital Heart Disease - Pathology (MBBS)
Source: Robbins & Kumar Basic Pathology (9780323790185) and Robbins, Cotran & Kumar Pathologic Basis of Disease (9780443264528)
Definition & Incidence
Congenital heart diseases (CHD) are abnormalities of the heart or great vessels present at birth. They account for 20-30% of all birth defects and affect nearly 1% of live births (~40,000 infants/year in the US). Incidence is higher in premature infants and stillborns (~25% of stillborns have cardiac malformations).
Twelve entities account for 85% of all CHD:
| Malformation | Incidence per million live births | % |
|---|---|---|
| Ventricular septal defect (VSD) | 4482 | 42 |
| Atrial septal defect (ASD) | 1043 | 10 |
| Pulmonary stenosis | 836 | 8 |
| Patent ductus arteriosus (PDA) | 781 | 7 |
| Tetralogy of Fallot | 577 | 5 |
| Coarctation of aorta | 492 | 5 |
| AV septal defect | 396 | 4 |
| Aortic stenosis | 388 | 4 |
| Transposition of great arteries | 388 | 4 |
| Truncus arteriosus | 136 | 1 |
| Total anomalous pulmonary venous connection | 120 | 1 |
| Tricuspid atresia | 118 | 1 |
Etiology & Pathogenesis
Faulty embryogenesis during gestational weeks 3-8 (when major cardiovascular structures develop) is the underlying mechanism. The cause is unknown in ~90% of cases.
Risk factors include:
- Prematurity
- Family history (genetic)
- Maternal conditions: diabetes, hypertension, obesity, phenylketonuria, thyroid disorders, connective tissue disorders
- Maternal drugs: phenytoin, retinoic acid, alcohol, smoking
- Assisted reproductive technology (IVF)
- Genetic/chromosomal associations: Trisomy 21 (Down - AV septal defect, VSD), Trisomy 18, Trisomy 13, Turner syndrome (coarctation of aorta)
- In utero infections: rubella (classically - PDA, pulmonary artery stenosis)
Classification (Hemodynamic Basis)
CHD is classified into three groups based on hemodynamic consequences:
1. Left-to-Right Shunts (Acyanotic - initially)
2. Right-to-Left Shunts (Cyanotic - "blue babies")
3. Obstructive Lesions (no shunt)
Group 1: Left-to-Right Shunts
These are the most common type. Blood flows from the high-pressure left side to the low-pressure right side. They are not cyanotic initially, but prolonged left-to-right shunting leads to:
- Increased pulmonary blood flow → pulmonary hypertension
- Right ventricular hypertrophy → right heart failure
- Eventually shunt reversal (right-to-left) → late-onset cyanosis = Eisenmenger syndrome (irreversible)
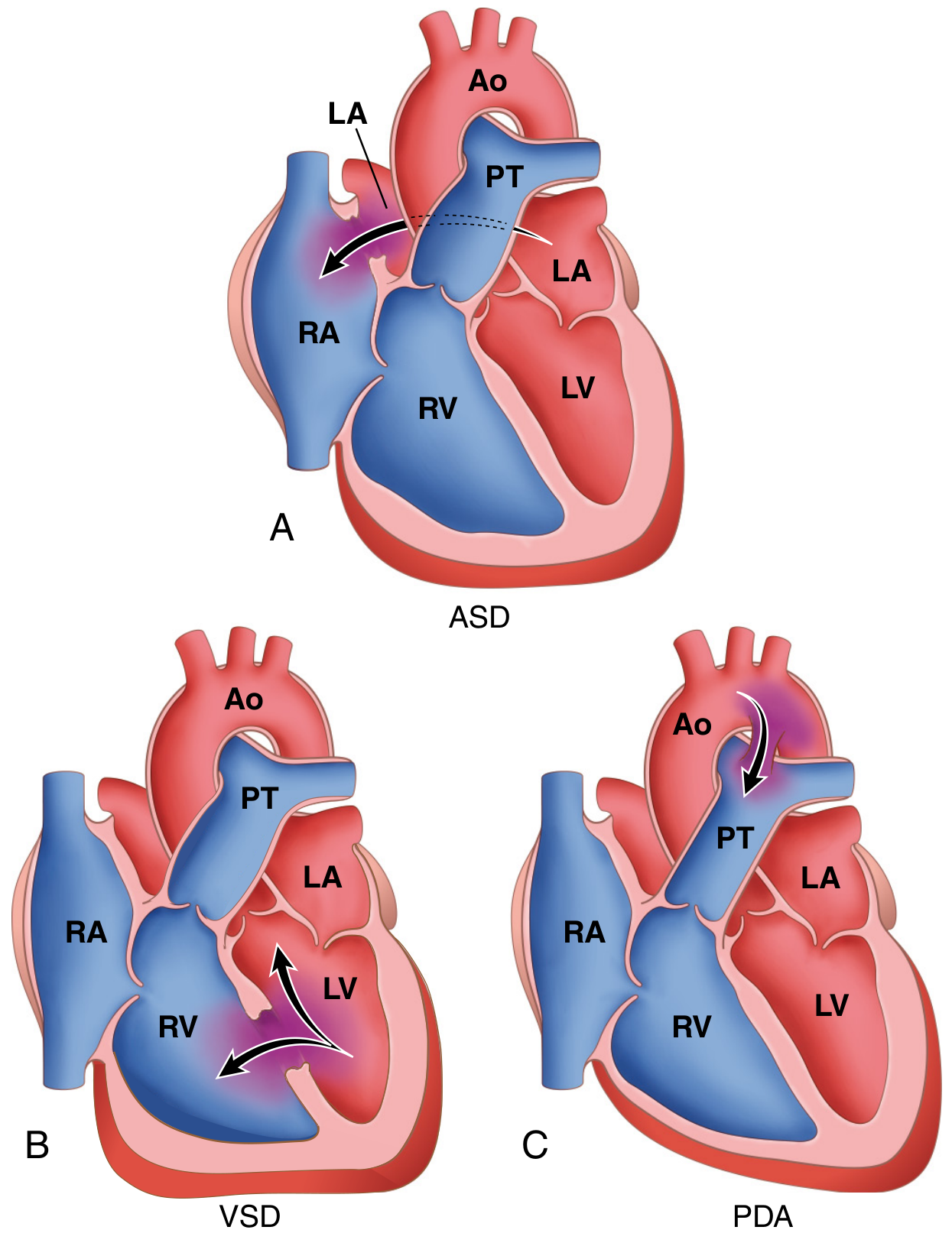
Atrial Septal Defect (ASD)
Pathology:
- Secundum ASD (90%) - deficient septum secundum formation at the center of the atrial septum; not associated with other anomalies
- Primum ASD (5%) - adjacent to AV valves; associated with AV valve abnormalities and VSD
- Sinus venosus defect (5%) - near entrance of superior vena cava; may be associated with anomalous pulmonary venous return
Clinical Features:
- Usually asymptomatic until adulthood (most common CHD diagnosed in adults, since ASDs rarely close spontaneously)
- Left-to-right shunt → pulmonary flow 2-8x normal
- Murmur due to increased flow through pulmonary valve
- Well tolerated; irreversible pulmonary hypertension is unusual
- Risk of paradoxical embolization, atrial arrhythmias
Treatment: Surgical or intravascular closure before heart failure or pulmonary vascular disease develops.
Ventricular Septal Defect (VSD)
- Most common CHD overall (42%)
- ~90% are in the membranous (perimembranous) portion of the interventricular septum
- Remaining are muscular VSDs
- Most small VSDs close spontaneously in childhood (this is why ASD - not VSD - is the most common defect found in adults)
Clinical Features:
- Small VSDs: asymptomatic; may produce a loud systolic murmur ("maladie de Roger")
- Large VSDs: left-to-right shunt → volume/pressure overload of pulmonary circulation
- Progresses faster to Eisenmenger syndrome than ASD (due to higher flow volumes and pressures)
- Small/medium VSDs: risk of infective endocarditis (jet lesion damages right ventricular endothelium)
- Early surgical correction is indicated for large VSDs
Patent Ductus Arteriosus (PDA)
- The ductus arteriosus connects the left pulmonary artery to the aorta just distal to the left subclavian artery
- In fetal life: diverts blood from pulmonary artery to aorta (bypassing unoxygenated lungs)
- Normally closes within 1-2 days of birth in response to: ↑ arterial oxygenation, ↓ pulmonary vascular resistance, ↓ prostaglandin E2
- Becomes the ligamentum arteriosum after closure
- Delayed/absent closure occurs with hypoxia (respiratory distress syndrome, other heart disease)
- Accounts for ~7% of CHD; 90% are isolated defects
Clinical Features:
- Harsh "machinery-like" murmur (continuous, throughout systole and diastole)
- High-pressure left-to-right shunt
- Small PDA: often asymptomatic
- Large PDA: Eisenmenger syndrome, congestive heart failure
- Risk of infective endocarditis
- Treatment: Isolated PDAs should be closed early (pharmacologically with indomethacin in premature infants - blocks prostaglandin synthesis; surgical ligation in others)
Group 2: Right-to-Left Shunts (Cyanotic CHD)
Poorly oxygenated blood flows directly from right to left, bypassing the pulmonary circulation → early cyanosis. Complications include:
- Clubbing (hypertrophic osteoarthropathy)
- Polycythemia (erythrocytosis due to chronic hypoxemia)
- Paradoxical embolization (venous thrombus → systemic arterial circulation → stroke, etc.)
Tetralogy of Fallot (TOF)
Most common cause of cyanotic CHD (~5% of all CHD).
Four Cardinal Features (all due to anterosuperior displacement of the infundibular septum):
- Ventricular septal defect (large, membranous)
- Obstruction of right ventricular outflow (subpulmonic stenosis - variable severity)
- Overriding of the aorta over the VSD
- Right ventricular hypertrophy (secondary to obstruction)
Mnemonic: VOORH or "PROV" (Pulmonary stenosis, RV hypertrophy, Overriding aorta, VSD)
Morphology:
- Heart is enlarged and "boot-shaped" (coeur en sabot) on X-ray - due to RV hypertrophy
- Proximal aorta is dilated; pulmonary trunk is hypoplastic
- RV wall markedly hypertrophied (may exceed LV thickness)
- Large VSD near the membranous portion of the interventricular septum
Clinical Features:
- Cyanosis from birth (if severe pulmonary stenosis) or after infancy
- Severity of symptoms depends on degree of right ventricular outflow obstruction
- If pulmonary stenosis is mild → may not be cyanotic initially ("pink tet")
- "Tet spells" (hypercyanotic spells): paroxysmal episodes of severe cyanosis; child characteristically squats to relieve symptoms (squatting ↑ systemic vascular resistance → reduces right-to-left shunt)
- Polycythemia, clubbing
- Right-sided aortic arch in ~25% of cases
- Pulmonary atresia may occur as the extreme form
- Prognosis without surgery: poor; most die in childhood
- Surgical repair is possible and yields good long-term outcomes
Transposition of the Great Arteries (TGA)
- Aorta arises from the right ventricle and the pulmonary artery arises from the left ventricle - complete reversal
- Results from failure of the aortopulmonary septum to spiral during development
- Creates two separate, parallel circuits (systemic and pulmonary) that are not interconnected - incompatible with life unless a communication exists
- Survival depends on a mixing defect - PFO, ASD, VSD, or PDA must be present
Clinical Features:
- Severe cyanosis from birth
- Right ventricle becomes the systemic ventricle → right ventricular hypertrophy
- Without intervention, most infants die within months
- Balloon atrial septostomy (Rashkind procedure) is performed emergently to create/enlarge ASD
- Definitive: arterial switch operation (Jatene procedure) in the neonatal period
Group 3: Obstructive Lesions
Coarctation of the Aorta
- Narrowing (stenosis) of the aorta, most often near the ligamentum arteriosum (juxtaductal position)
- Association: Turner syndrome (45,X)
- Two classic forms:
| Feature | Infantile (preductal) | Adult (postductal/juxtaductal) |
|---|---|---|
| Location | Proximal to ductus arteriosus | Distal to ductus arteriosus |
| Cyanosis | Yes (differential cyanosis - lower limbs) | No |
| Age of presentation | Infancy | Adulthood |
| Ductus | Usually patent | Usually closed |
Clinical Features (adult/juxtaductal form):
- Hypertension in upper extremities; hypotension in lower extremities
- Weak/absent femoral pulses
- Intercostal "notching" on chest X-ray - due to collateral circulation through intercostal arteries (dilated and tortuous)
- "3 sign" on chest X-ray (indentation of aorta at coarctation site)
- Headache, epistaxis (hypertension in upper body)
- Claudication in lower limbs
- Risk of: aortic rupture, infective endocarditis, intracranial hemorrhage (from berry aneurysms - associated with bicuspid aortic valve)
Associated anomaly: Bicuspid aortic valve is present in ~50% of cases.
Treatment: Surgical repair or balloon dilation/stenting. Excellent results if done early.
Eisenmenger Syndrome
A common complication of uncorrected left-to-right shunts (VSD > ASD, PDA):
- Chronic high-flow/high-pressure pulmonary circulation → irreversible pulmonary hypertension → pulmonary vascular resistance exceeds systemic vascular resistance → shunt reversal (right-to-left) → late cyanosis
- Once established, the structural defects are no longer surgically correctable
- This is the main reason for early intervention in large left-to-right shunts
Summary Table - Key Exam Points
| Defect | Shunt Type | Cyanosis | Key Feature | Murmur |
|---|---|---|---|---|
| VSD | L→R | No (initially) | Most common CHD | Pansystolic, LLSB |
| ASD | L→R | No | Most common in adults | Systolic ejection; wide fixed S2 split |
| PDA | L→R | No | "Machinery" murmur | Continuous machinery murmur |
| TOF | R→L | Yes (early) | Most common cyanotic CHD; boot-shaped heart | Ejection systolic |
| TGA | R→L | Yes (severe) | Parallel circuits; needs mixing defect | Variable |
| Coarctation | Obstruction | No (unless preductal) | Rib notching; BP differential; Turner syndrome | Systolic, interscapular |
High-Yield Associations for Exams
- VSD = most common CHD overall
- ASD = most common CHD in adults
- TOF = most common cyanotic CHD; "boot-shaped heart"
- TGA = most common cyanotic CHD presenting on day 1 of life (severe cyanosis at birth)
- Coarctation = associated with Turner syndrome and bicuspid aortic valve
- Rubella → PDA, pulmonary artery stenosis
- Down syndrome (Trisomy 21) → AV septal defect, VSD
- PDA closure → indomethacin (premature infants); kept open with prostaglandins (PGE1) in duct-dependent lesions like TGA/pulmonary atresia
- Eisenmenger syndrome = irreversible pulmonary hypertension from uncorrected L→R shunt → R→L shunt → late cyanosis
Sources: Robbins & Kumar Basic Pathology, p. 347-360; Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 502-520
This is a shared conversation. Sign in to Orris to start your own chat.