1st pass metabolism
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
I now have comprehensive information from multiple authoritative sources. Here is the complete answer:
First-Pass Metabolism (Presystemic Elimination)
Definition
First-pass metabolism (also called presystemic elimination or presystemic extraction) is the biotransformation of an orally administered drug in the intestinal wall and/or liver before it reaches the systemic circulation, thereby reducing the amount of active drug available to the body.
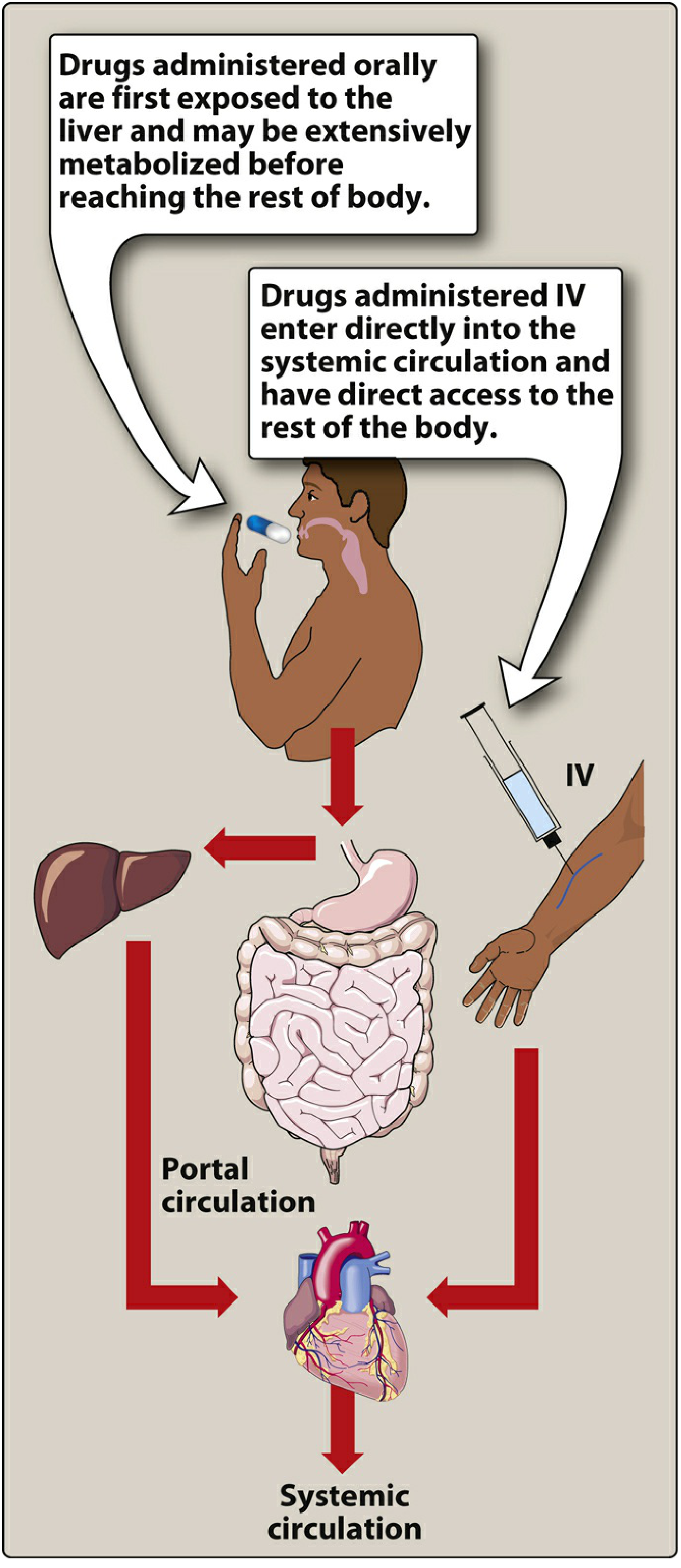
Figure: Oral drugs are exposed to the liver via portal circulation and may be extensively metabolized before reaching systemic circulation. IV drugs bypass this entirely. - Lippincott Illustrated Reviews: Pharmacology
Pathway of First-Pass Metabolism
After oral ingestion, the drug follows this sequence:
- GI lumen - drug is absorbed across the intestinal epithelium (enterocyte)
- Enterocyte - may undergo metabolism by CYP3A4 in the gut wall, or be pumped back into the lumen by P-glycoprotein (efflux transporter)
- Portal vein - absorbed drug enters the portal venous system
- Liver (hepatocyte) - drug may be metabolized by CYP450 enzymes (especially CYP3A4, CYP2D6) or excreted into bile via biliary canaliculi
- Systemic circulation - only the fraction that survives all these steps reaches the bloodstream
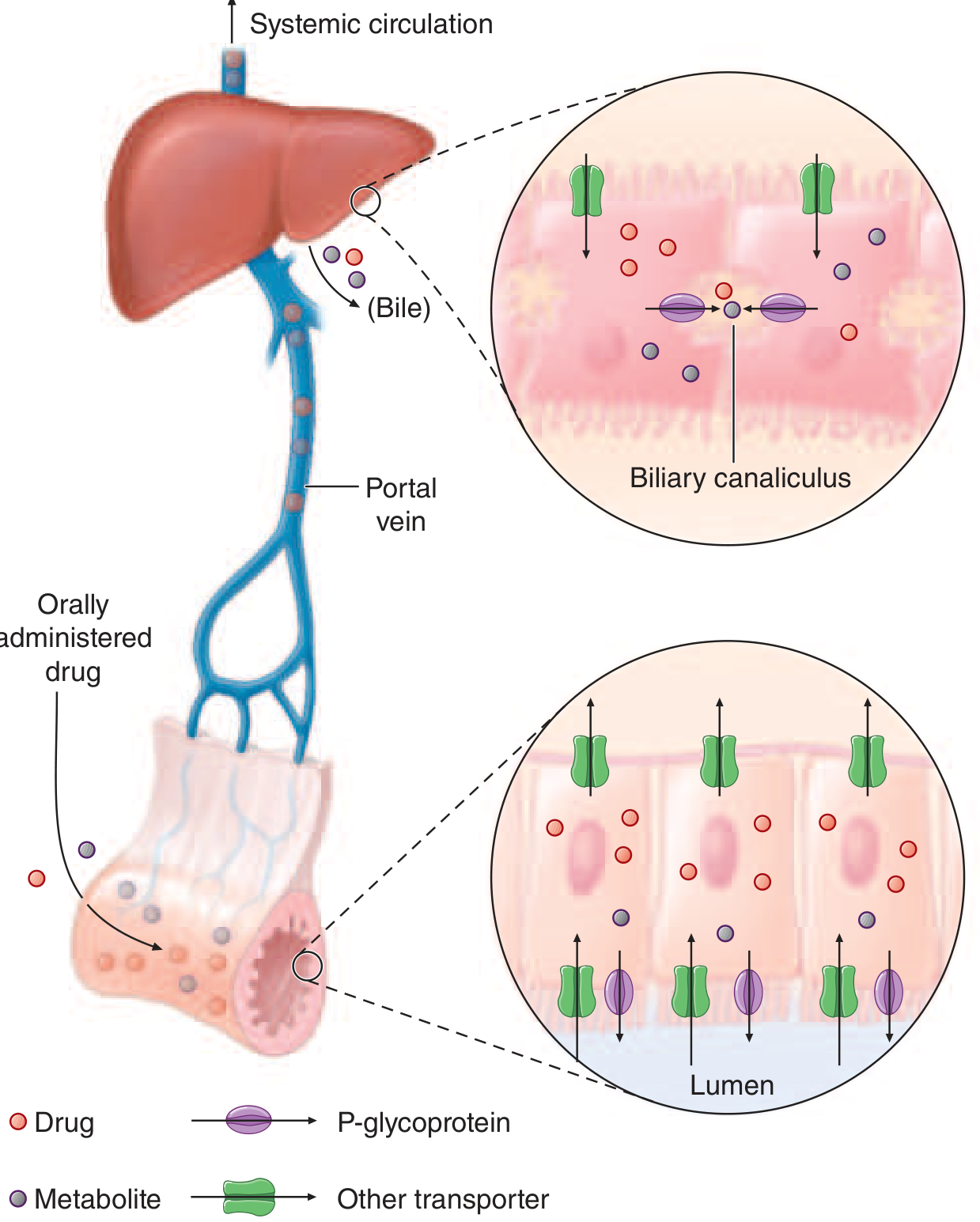
Figure: Presystemic elimination mechanisms - Harrison's Principles of Internal Medicine 22E
Effect on Bioavailability
Bioavailability (F) is the fraction of an administered dose that reaches systemic circulation unchanged. First-pass metabolism is a major reason why oral bioavailability is less than 100%.
Bioavailability (F) = AUC(oral) / AUC(IV) × 100%
The higher the hepatic extraction ratio, the greater the first-pass effect, and the lower the oral bioavailability. For high-extraction drugs, hepatic clearance approaches hepatic blood flow - these drugs have very low oral bioavailability. - Tietz Textbook of Laboratory Medicine
Classic Examples of High First-Pass Drugs
| Drug | First-Pass Effect | Clinical Implication |
|---|---|---|
| Nitroglycerin | >90% cleared | Cannot be given orally; use sublingual/transdermal/IV |
| Lidocaine | Extensive | Not used as oral agent |
| Naloxone | Extensive | IV/intranasal route required |
| Morphine | Significant | Oral dose much higher than IV dose |
| Propranolol | Large | High oral dose given to account for first-pass loss |
| Midazolam | >50% | Bioavailability <50% orally |
| Asenapine | Extensive if swallowed | Formulated as sublingual tablet |
Routes That Bypass First-Pass Metabolism
| Route | Mechanism of Bypass |
|---|---|
| Sublingual | Absorbed directly into systemic (not portal) veins |
| Transdermal | Absorbed into systemic veins, bypasses portal circulation |
| IV/IM/Subcutaneous | Directly enters systemic circulation |
| Inhalation | Bypasses hepatic first pass (but lungs may contribute minor metabolism) |
| Rectal (lower rectum) | Inferior vena cava drainage; ~50% bypass (upper rectal veins drain to portal system) |
- Katzung's Basic and Clinical Pharmacology, 16th Edition
Factors Affecting Extent of First-Pass Metabolism
- Hepatic blood flow - reduced flow (e.g., in cirrhosis, congestive heart failure, portal hypertension) decreases first-pass extraction, raising systemic drug levels and increasing toxicity risk for high-extraction drugs
- Enzyme induction/inhibition - CYP450 inducers (rifampin, phenytoin) increase first-pass and reduce bioavailability; inhibitors (ketoconazole, grapefruit) reduce first-pass and raise bioavailability
- Genetic polymorphisms - CYP2D6 poor metabolizers vs. ultra-rapid metabolizers show dramatically different first-pass effects (e.g., codeine toxicity in ultra-rapid metabolizers)
- Gut wall transporters - P-glycoprotein efflux in enterocytes reduces absorption before the drug even reaches the liver
- Age and disease - liver disease reduces first-pass effect; elderly may have reduced hepatic mass and blood flow
Clinical Significance
- Drugs with high first-pass metabolism have high oral-to-parenteral dose ratios (e.g., morphine oral dose ~3x the IV dose)
- Liver disease can dramatically increase systemic exposure to high-extraction drugs - dose reduction is required
- Drug interactions at CYP3A4 or P-glycoprotein level can unpredictably alter bioavailability of high-first-pass drugs
- Pro-drugs can exploit first-pass metabolism: codeine is converted to morphine in the liver by CYP2D6, making it an active analgesic only after first-pass conversion
Sources: Lippincott Illustrated Reviews: Pharmacology | Goodman & Gilman's Pharmacological Basis of Therapeutics | Harrison's Principles of Internal Medicine 22E | Katzung's Basic and Clinical Pharmacology 16E | Tietz Textbook of Laboratory Medicine 7E
This is a shared conversation. Sign in to Orris to start your own chat.