Severe oesophagitis in endoscopy causes and management
Reading File
Finding Sources
Searching PubMed
"esophagitis" AND "endoscopy" AND management
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Searching Images
severe esophagitis endoscopy Los Angeles grade C D
Loading Image
Loading Image
Loading Image
I now have everything needed for a comprehensive, well-illustrated answer. Here it is:
Severe Oesophagitis at Endoscopy: Causes & Management
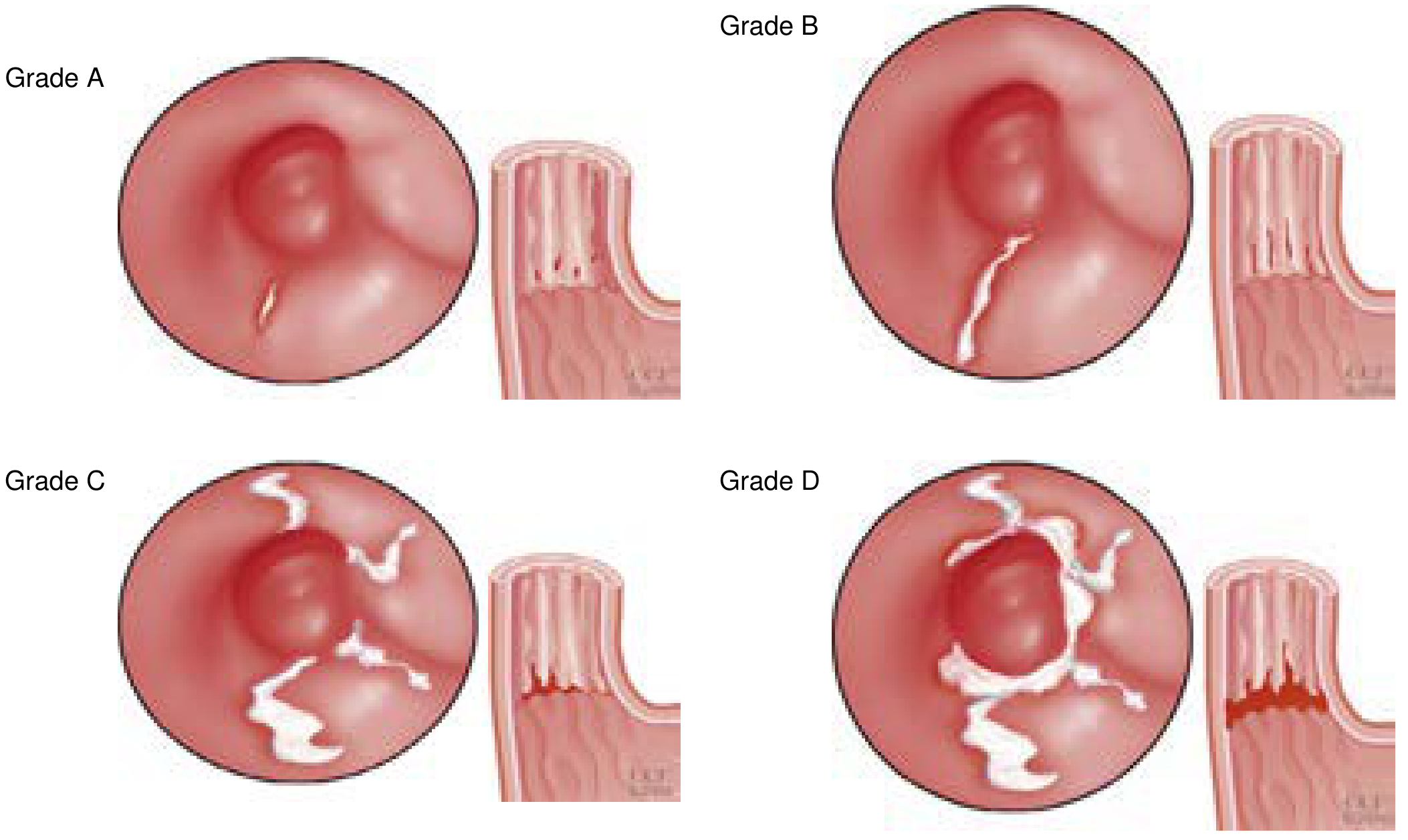
Endoscopic Grading — Los Angeles Classification
The Los Angeles (LA) classification is the standard grading system used at endoscopy. Severe oesophagitis corresponds to Grades C and D:
| Grade | Endoscopic Finding |
|---|---|
| A | Mucosal break(s) <5 mm, not extending between fold tops |
| B | Mucosal break(s) >5 mm, not extending between fold tops |
| C | Mucosal break(s) extending between tops of ≥2 folds but <75% of circumference |
| D | Mucosal break(s) involving ≥75% of the esophageal circumference |
Causes of Severe Oesophagitis
1. Gastro-oesophageal Reflux Disease (GERD) — Most Common
- Reflux of acidic gastric contents (and sometimes duodenal bile) onto squamous mucosa
- Risk factors reducing lower oesophageal sphincter (LOS) tone: obesity, hiatal hernia, alcohol, tobacco, CNS depressants, pregnancy, delayed gastric emptying
- Histology: eosinophil and neutrophil infiltration, basal zone hyperplasia, elongation of lamina propria papillae
- Severe grades (C/D) are independent risk factors for haemorrhagic esophagitis (along with cirrhosis, anticoagulant use, poor performance status)
- Complications: ulceration, haematemesis/melaena, stricture, Barrett's oesophagus
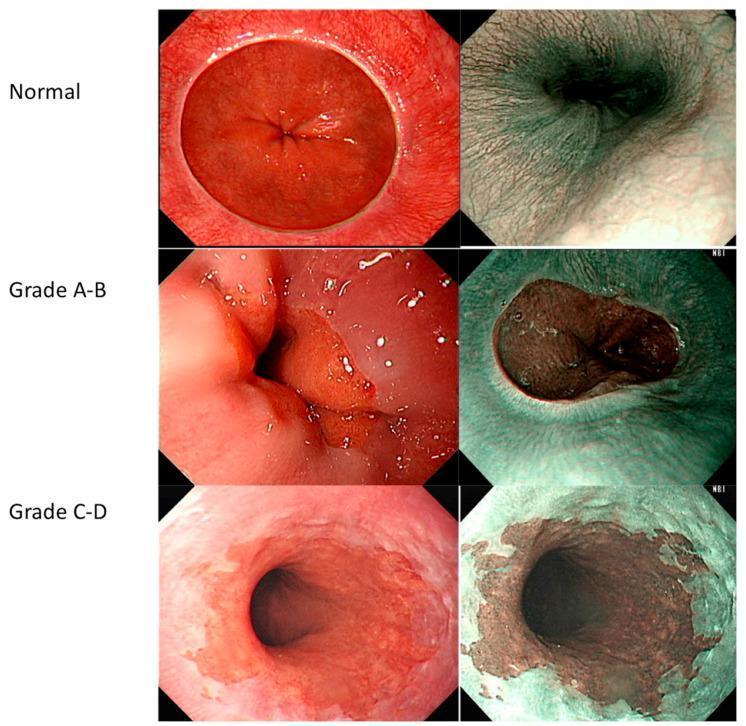
Special case — Zollinger-Ellison syndrome / MEN1: hypersecretion of gastric acid produces LA grade D oesophagitis with concurrent hypertrophic gastric folds and postbulbar duodenal ulcers (illustrated in image panel above)
2. Infectious Oesophagitis
Predominantly in immunocompromised patients (HIV, transplant, chemotherapy), but can occur in the immunocompetent:
| Organism | Endoscopic Appearance | Biopsy Site | Notes |
|---|---|---|---|
| Candida | Adherent grey-white pseudomembranes/plaques | Plaque surface — brush cytology or pinch biopsy | Most common fungal cause; PAS-D stain highlights hyphae |
| HSV | Punched-out ulcers, ulcer margins show herpetic inclusions | Ulcer margin (squamous epithelial cells infected) | Multinucleate cells with nuclear inclusions |
| CMV | Shallower, broad ulcerations | Ulcer base (mesenchymal/columnar cells infected) | Nuclear + cytoplasmic inclusions; 3+ biopsies from base needed |
3. Eosinophilic Oesophagitis (EoE)
- Chronic immune-mediated disease; food antigen driven
- Endoscopic features: rings (trachealization), linear furrows, white exudates/plaques, mucosal tears, oedema, narrow-calibre lumen
-
90% of patients show ≥1 endoscopic abnormality
- Histology: ≥15 eosinophils/HPF (often much higher); eosinophilic microabscesses; surface layering
- Typically refractory to PPIs; patients are often atopic
4. Pill-Induced Oesophagitis
- Pill fails to transit into stomach, causing direct mucosal injury
- Common offending drugs: doxycycline/tetracyclines, bisphosphonates (alendronate), NSAIDs/aspirin, potassium chloride, ferrous sulphate, quinidine
- Predisposing factors: taking pills without water, supine position, elderly, reduced motility, extrinsic compression
- Range: mild irritation → frank ulceration → haemorrhage → stricture
- Clinical presentation: sudden onset retrosternal pain and odynophagia — often diagnosable from history alone
5. Chemical / Caustic Oesophagitis
- Corrosive acids or alkalis, alcohol, excessively hot fluids, heavy smoking
- Severe cases → haemorrhage, stricture, perforation
- Morphology: non-specific ulceration and acute inflammation
6. Radiation-Induced Oesophagitis
- Complication of radiotherapy to mediastinum/thorax; degree of injury proportional to total dose
- Mucosa becomes inflamed, friable, haemorrhagic
- Vascular damage adds an ischaemic component
7. Other Causes
- Graft-versus-host disease (GvHD) — post-BMT
- Crohn's disease — rare oesophageal involvement
- Desquamative skin diseases — bullous pemphigoid, epidermolysis bullosa
Management by Cause
GERD — Severe Erosive (Grade C/D)
Medical (first-line):
- High-dose PPI (e.g. omeprazole 40 mg daily or twice daily) — standard treatment; reduces gastric acidity and allows mucosal healing
- Duration: 8–12 weeks for severe erosive disease, then reassess
- Repeat endoscopy after treatment is mandatory to exclude underlying Barrett's oesophagus
- Lifestyle: weight loss, head-of-bed elevation, dietary modification, avoid precipitants
For haemorrhage from erosive oesophagitis:
- EGD is essential for diagnosis; endoscopic haemostatic therapy generally has no role unless a focal ulcer with a stigma of recent haemorrhage (SRH) is found
- If discrete visible vessel/clot: injection, thermal coagulation, or clipping
- For diffuse LA-D haemorrhagic oesophagitis where endoscopic haemostasis is not feasible: balloon tamponade (Minnesota tube) can achieve temporary haemostasis
Surgical (antireflux surgery — ARS):
- Indicated for: persistent symptoms despite optimal PPI therapy, patient preference, or severe/recurrent complications
- Pre-operative workup: manometry (to guide fundoplication type), pH monitoring, barium swallow
- Nissen fundoplication (360°) for normal motility; Toupet fundoplication (270° partial) for ineffective oesophageal motility
- All patients should be on maximal PPI therapy before ARS is considered
Complications requiring additional management:
- Peptic stricture: serial endoscopic dilatation before or instead of surgery
- Barrett's oesophagus: surveillance endoscopy programme; eradication if dysplasia present
Infectious Oesophagitis
| Organism | Treatment |
|---|---|
| Candida | Fluconazole (systemic) — preferred over topical nystatin for oesophageal disease |
| HSV | Aciclovir (IV in immunocompromised; oral in immunocompetent) |
| CMV | Ganciclovir (IV) or valganciclovir (oral maintenance) |
- Endoscopy with biopsies and brushings is critical — the specific agent determines therapy
- In HIV patients with oesophageal ulcers, empirical fluconazole can be trialled before endoscopy if Candida is clinically suspected
Eosinophilic Oesophagitis
- Biopsy protocol: 2–4 biopsies from at least two levels (proximal + distal) regardless of endoscopic appearance; fixed in 10% buffered formalin
- PPI trial first (to exclude PPI-responsive oesophageal eosinophilia)
- Dietary elimination — six-food elimination diet (milk, wheat, egg, soy, nuts, seafood) or targeted allergy testing
- Swallowed topical corticosteroids — fluticasone (MDI swallowed) or budesonide (viscous oral suspension) — first-line pharmacotherapy
- Oesophageal dilatation — for symptomatic strictures or narrow-calibre oesophagus (high risk of mucosal tears — warn patients; start with small diameter)
- Dupilumab — biologic (anti-IL-4/IL-13) approved for EoE in adults and adolescents refractory to other therapies
Pill-Induced Oesophagitis
- Stop the offending drug (switch to liquid formulation or alternative agent if possible)
- Sucralfate suspension — mucosal protective coating
- PPIs for acid suppression and symptom relief
- Counsel on prevention: take pills with full glass of water, remain upright for ≥30 min after ingestion
- Most cases resolve spontaneously in 1–2 weeks; severe ulceration → follow up endoscopy to exclude stricture
Caustic/Chemical Oesophagitis
- Supportive care; nothing by mouth initially
- IV PPIs, IV fluids
- Endoscopy within 24–48 h to assess severity (use grading system: I–IIIb)
- Severe burns (grade IIb–III): nasogastric tube feeding, IV antibiotics (if aspiration/perforation risk), surgical consultation
- Do NOT induce emesis — worsens mucosal injury
- Long-term: endoscopic dilatation for strictures; surgical oesophageal resection for severe/refractory cases
Key Takeaways
- LA grade C/D = severe oesophagitis requiring aggressive management and mandatory follow-up endoscopy after treatment
- GERD is the most common cause; high-dose PPI for 8–12 weeks is standard
- Biopsies are essential — they differentiate GERD (eosinophils predominantly distal), EoE (eosinophils throughout, ≥15/HPF), infectious (specific inclusions/organisms), and malignancy
- Immunocompromised patients presenting with odynophagia: always consider Candida, HSV, CMV — treat empirically if clinically obvious, but endoscopy with targeted biopsies is the gold standard
- Pill-induced oesophagitis is underdiagnosed — history (new medication, no water, supine ingestion) is diagnostic
— Robbins & Kumar Basic Pathology; Sleisenger and Fordtran's Gastrointestinal and Liver Disease; Clinical Gastrointestinal Endoscopy 3e; Current Surgical Therapy 14e; Rosen's Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.