Different Surgical approaches to elbow explain it with appropriate images and diagrams
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive content from Campbell's Operative Orthopaedics covering all the major surgical approaches to the elbow. Let me now compile a thorough, well-illustrated answer.
Surgical Approaches to the Elbow
Source: Campbell's Operative Orthopaedics 15th Edition (2026)
The elbow can be accessed from multiple directions depending on the pathology, required exposure, and structures at risk. The major approaches are grouped below.
Summary Table of Surgical Approaches
| Category | Approach (Author) | Tissue Plane Used |
|---|---|---|
| Posterior | Campbell | Midline triceps split or aponeurosis tongue |
| Posterior | Wadsworth (Extensile Posterolateral) | Triceps aponeurosis tongue + full-thickness deep head |
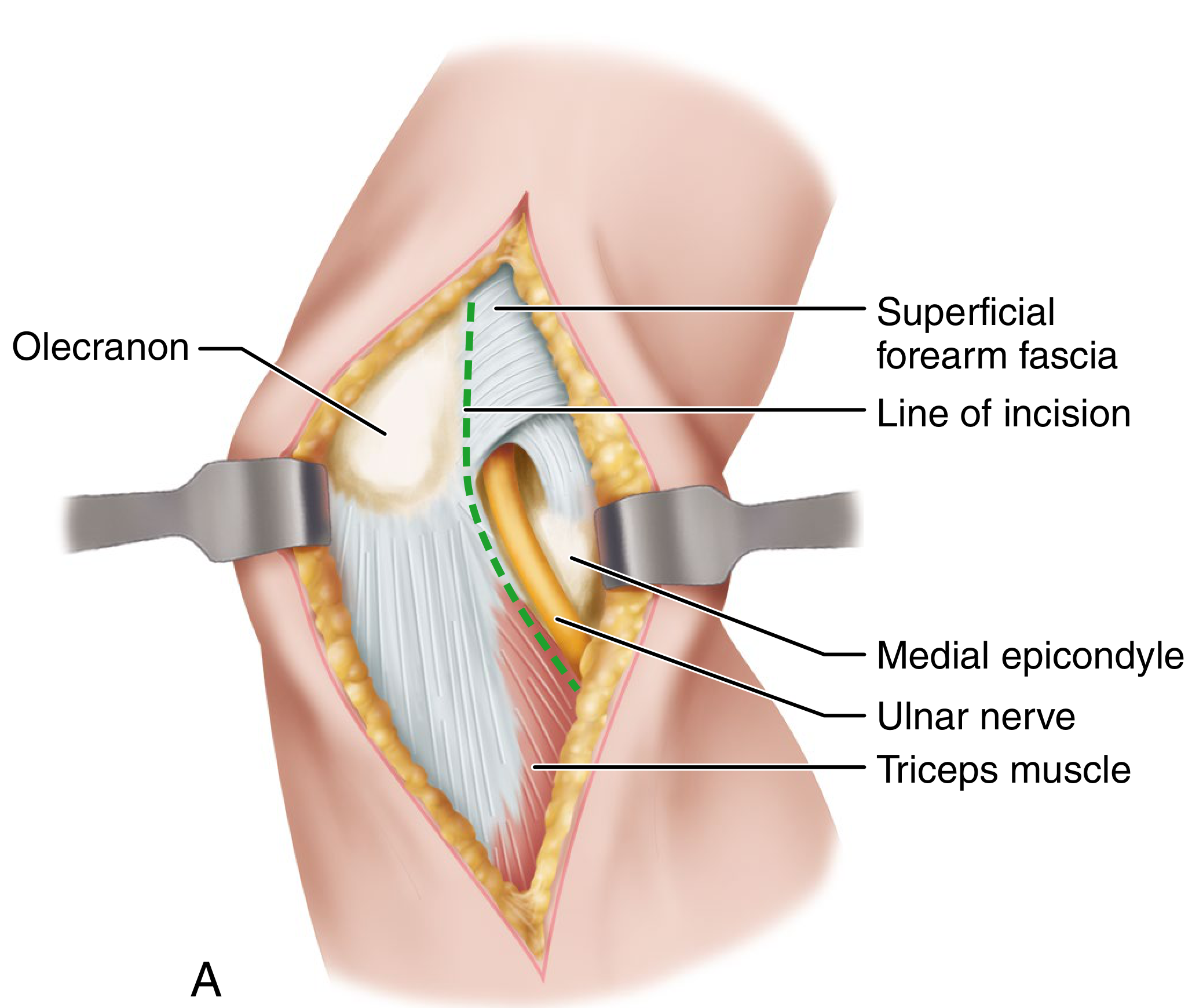
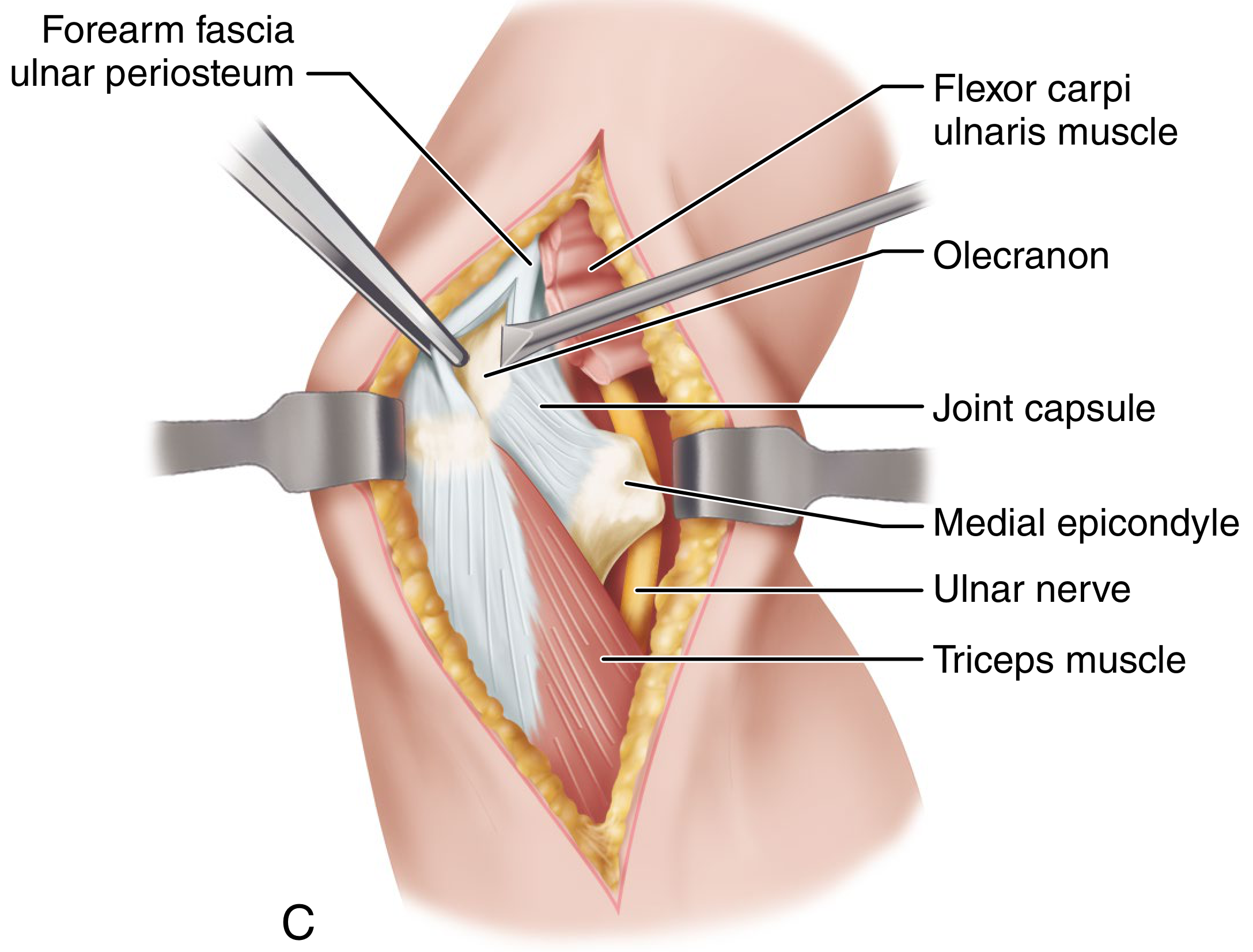
| Posterior | Bryan-Morrey | Elevate triceps mechanism from medial olecranon, reflect laterally |
| Posterior | Extended Kocher / Ewald | ECU and anconeus / triceps |
| Lateral | Kocher (J approach) | Between anconeus and ECU |
| Lateral | Simple lateral | Between triceps and ECRL/brachioradialis |
| Medial | Molesworth-Campbell | Osteotomy of medial epicondyle |
| Medial + Lateral | Technique 1.114 | Bilateral capsule incisions |
| Global (Circumferential) | Patterson, Bain, Mehta | Posterior midline + medial/lateral fasciocutaneous flaps |
| Anterior | Henry | Brachialis / brachioradialis interval |
1. Posterior Approaches
1a. Posterolateral Approach (Campbell)
Indications: Old posterior dislocations, distal humerus fractures involving the joint, elbow arthroplasty.
Key steps:
- Skin incision begins 10 cm proximal to the elbow on the posterolateral aspect, extends 13 cm distally
- The triceps aponeurosis is fashioned into a tongue-shaped flap with its base at the olecranon, retracted distally
- If triceps is not contracted, the muscle and aponeurosis are split longitudinally in the midline
- Periosteum is elevated from the posterior distal humerus for 5 cm
- The ulnar nerve must be protected at all times during medial capsule stripping
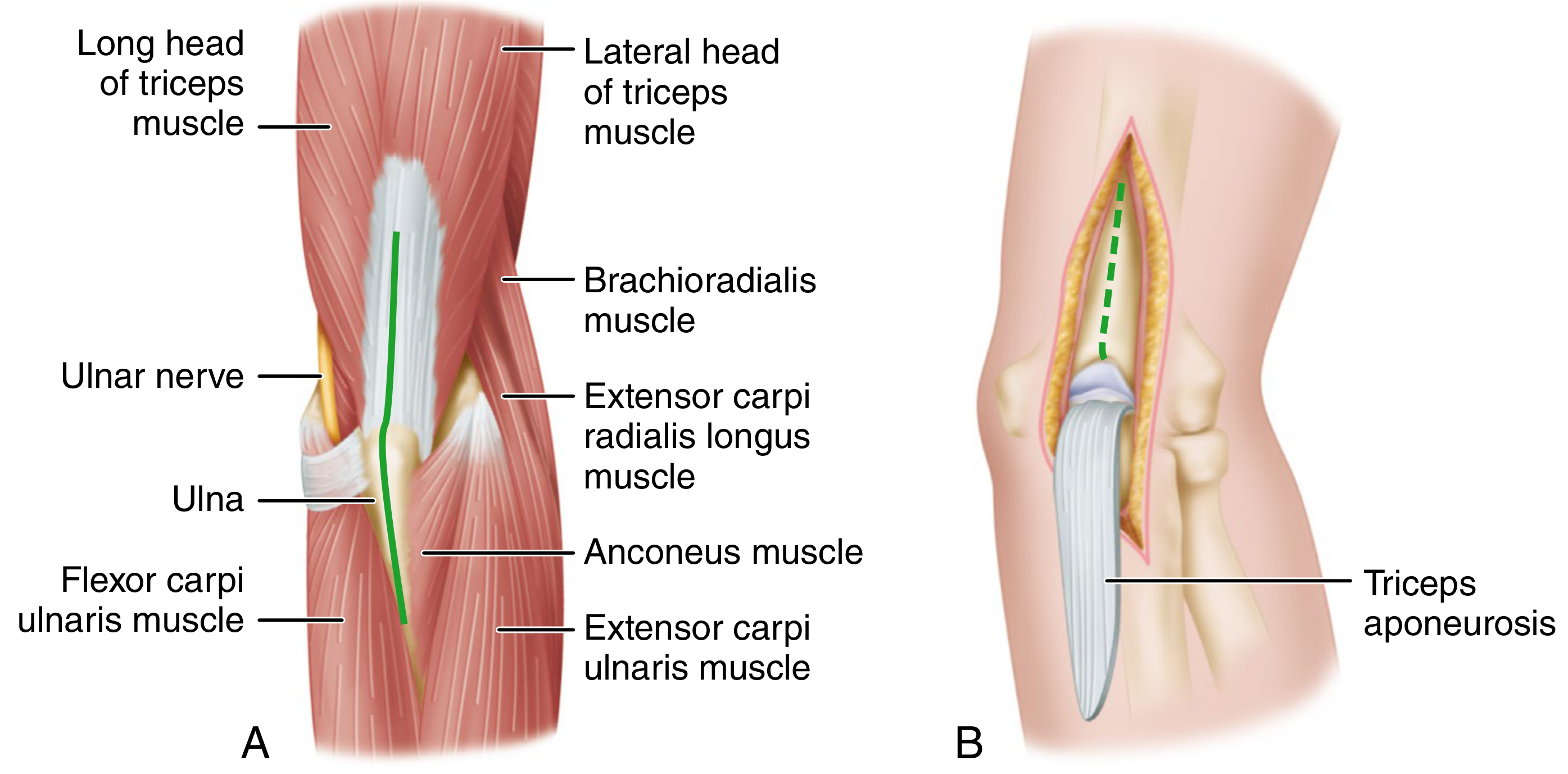
1b. Extensile Posterolateral Approach (Wadsworth)
Indications: Displaced distal humeral articular fractures, synovectomy, total elbow arthroplasty, any procedure requiring maximal posterior exposure.
Key steps:
- Patient prone, elbow flexed 90° over support, forearm dependent
- Curved skin incision from proximal posterior arm, down to the posterolateral epicondyle, then medially to the posterior ulnar border 4 cm distal to the olecranon tip
- The ulnar nerve is identified and released from its tunnel by dividing the arcuate ligament between the two heads of flexor carpi ulnaris, then retracted with a rubber sling
- A tongue of triceps tendon is fashioned with its base attached to the olecranon; the remaining peripheral tendinous rim stays attached for later repair
- The incision extends distally through the triceps aponeurosis to separate the anconeus from the extensor carpi ulnaris
- The posterior capsule is divided in the same line
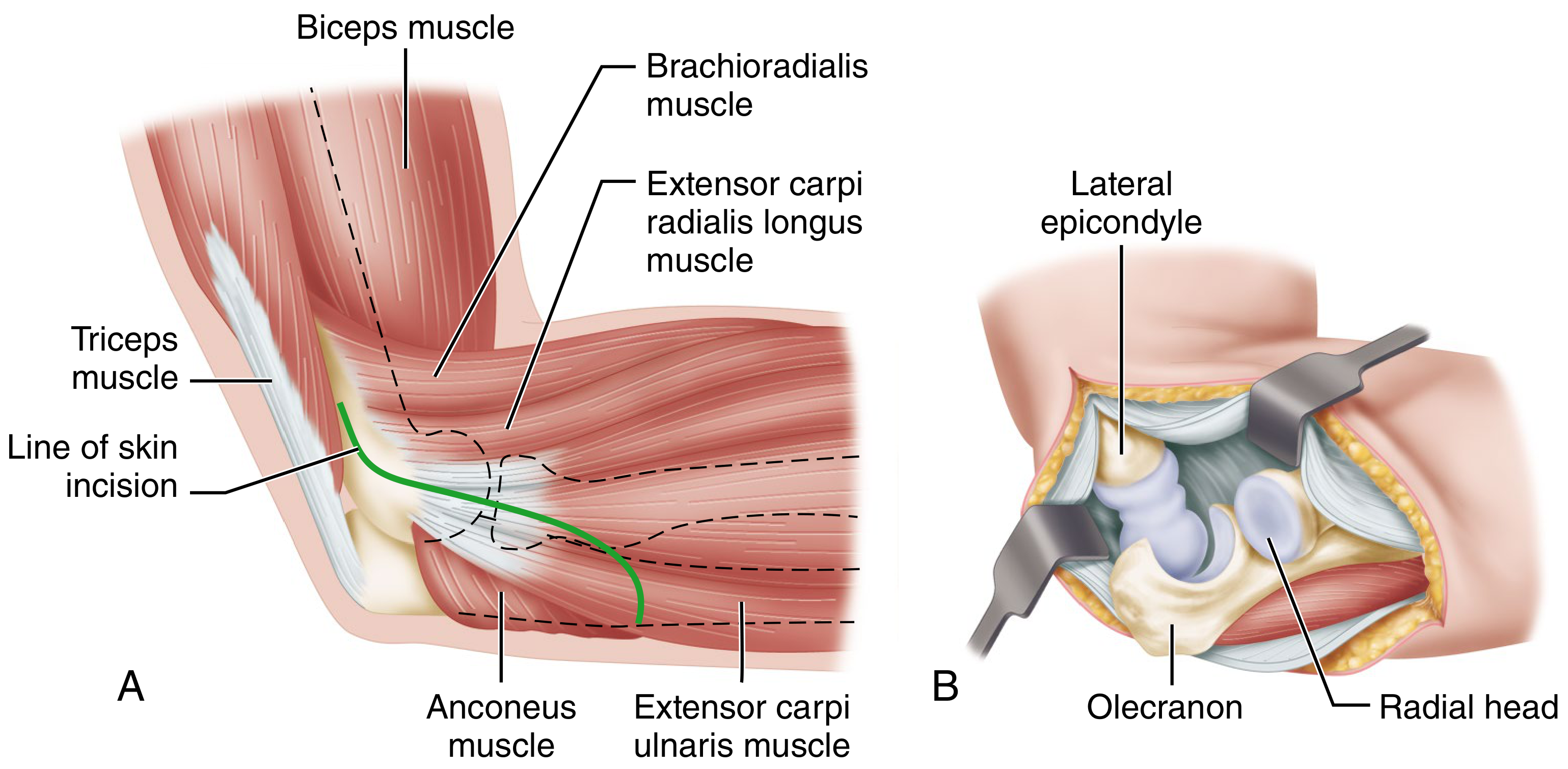
2. Lateral Approach
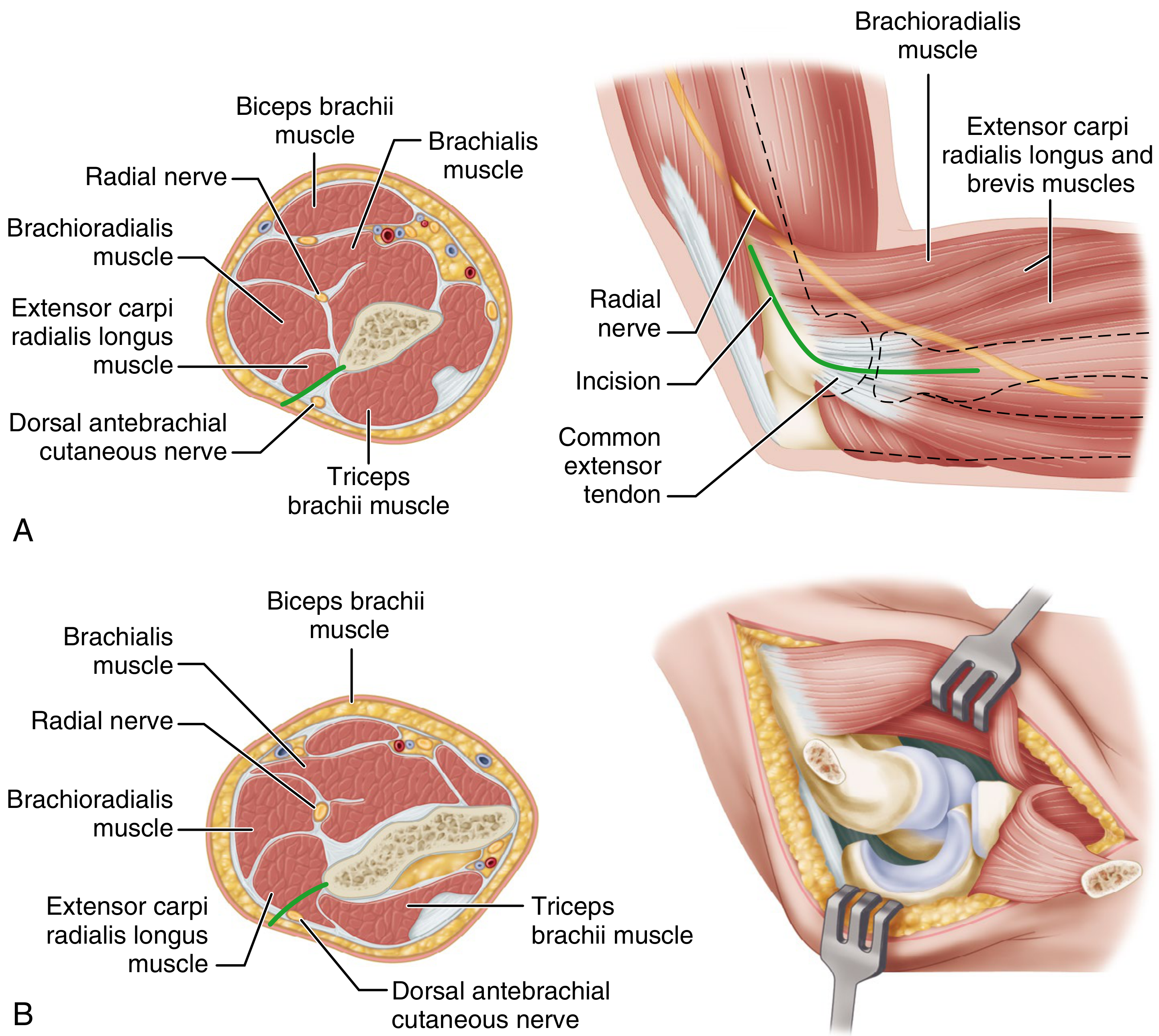
2a. Lateral (Simple) Approach
Indications: Access to the radiohumeral joint, radial head, lateral epicondyle.
Key steps:
- Incision begins ~5 cm proximal to the lateral epicondyle, extends distally to the epicondyle, then 5 cm along the anterolateral forearm
- Develop the interval between the triceps (posterior) and the origins of extensor carpi radialis longus and brachioradialis (anterior)
- In the proximal wound, avoid the radial nerve where it enters between brachialis and brachioradialis
- Separate the common extensor origin from the lateral epicondyle (or elevate it with a thin flake of bone)
- Reflect the common extensor origin distally to expose the radiohumeral joint
- Always protect the deep branch of the radial nerve as it enters the supinator
2b. Kocher Lateral J Approach
Indications: Radial head fractures, lateral ligament reconstruction, posterolateral instability, capitellum/lateral condyle procedures.
Key steps:
- Incision begins 5 cm proximal to the elbow over the lateral supracondylar ridge, extends to the epicondyle, then 5 cm distal to the radial head, curving medially and posteriorly to end at the posterior ulnar border
- The dissection plane is between the anconeus (posterior) and extensor carpi ulnaris (anterior)
- The elbow can be dislocated laterally when full exposure is needed
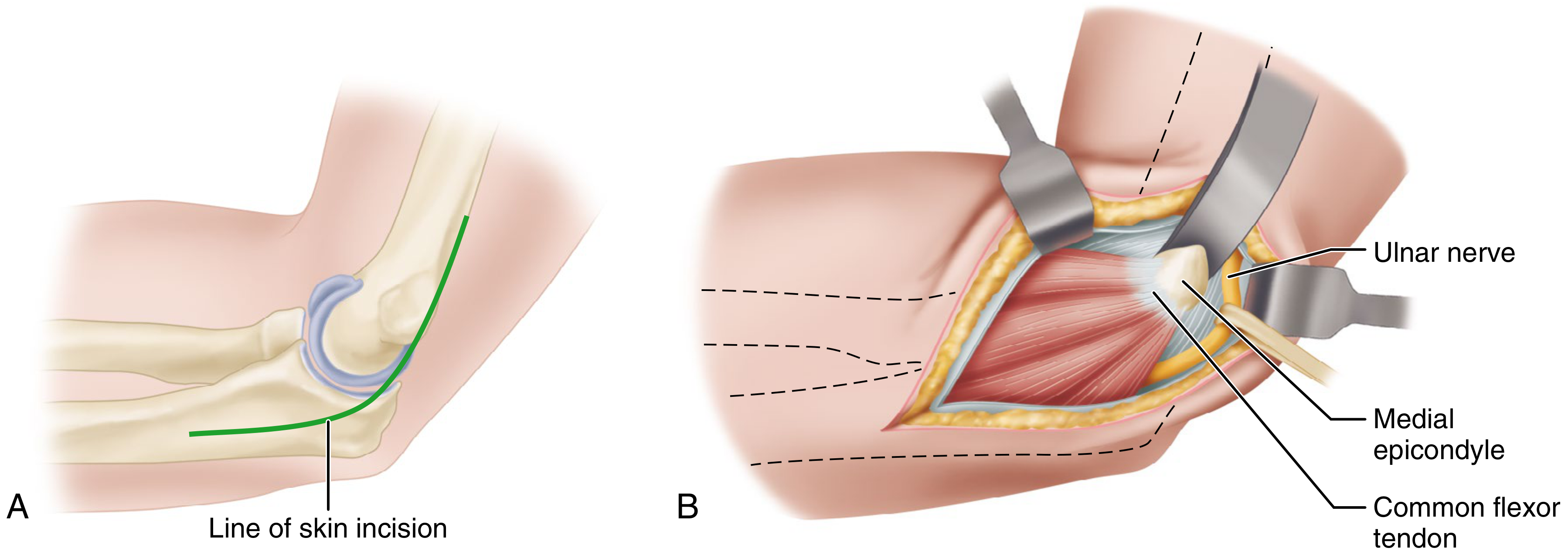
3. Medial Approach
3a. Medial Approach with Osteotomy of the Medial Epicondyle (Molesworth-Campbell)
Indications: Fractures of the medial epicondyle (especially incarcerated), medial capsule/ligament procedures, access to the anterior joint.
Key steps:
- Elbow flexed to a right angle; medial incision centered over the tip of the medial epicondyle (5 cm proximal to 5 cm distal)
- Isolate the ulnar nerve in the groove posterior to the epicondyle and retract it posteriorly
- Detach the medial epicondyle with a small osteotome (with common flexor origin undisturbed) and reflect it distally
- Continue subperiosteally to free the medial coronoid process; incise the capsule
- Strip periosteum and capsule anteriorly and posteriorly as needed
- Avoid the median nerve which crosses the anterior joint
- With the lateral capsule as a hinge, the joint can be dislocated
4. Medial and Lateral (Bilateral) Approach
Indications: Moderate exposure of both sides of the joint without the need for full extensile exposure.
Key steps:
- An incision 5-7 cm long on either or both sides of the joint, just anterior to the condyles, parallel with the epicondylar ridges
- The flexion crease of the elbow lies proximal to the joint line (a useful landmark)
- Capsule incised from proximal to distal on each side
- On the medial side: carefully avoid the ulnar nerve
5. Global (Circumferential) Approach (Patterson, Bain, Mehta)
Indications: Complex instability, circumferential exposure for collateral ligaments, coronoid process, anterior joint capsule.
Key steps:
- Straight posterior midline incision
- Sharp dissection through deep fascia to the triceps tendon and subcutaneous border of the ulna
- If medial exposure needed: open cubital tunnel, isolate ulnar nerve, transpose anteriorly, protect with Penrose drain
- Develop full-thickness medial or lateral fasciocutaneous flaps as needed
From the posterolateral side:
- Develop the Kocher interval (anconeus-ECU) to expose the elbow capsule and lateral epicondyle
- Reflect anconeus and triceps medially to expose the olecranon fossa and posterior distal humerus
From the posteromedial side:
- Reflect the medial fasciocutaneous flap to expose the posteromedial joint and sublime tubercle
Key Nerves at Risk - Summary
| Approach | Nerve at Risk | Where |
|---|---|---|
| Posterolateral (Campbell) | Ulnar nerve | Medial side during capsule stripping |
| Extensile posterolateral (Wadsworth/Bryan-Morrey) | Ulnar nerve | Released from cubital tunnel early |
| Lateral / Kocher | Radial nerve (posterior interosseous) | Entering supinator, proximal wound |
| Medial epicondyle osteotomy | Ulnar nerve (posterior), Median nerve (anterior) | Groove / anterior joint |
| Anterior approach | Radial nerve, Median nerve, Brachial artery | All anterior structures |
Quick Reference: Choosing the Right Approach
| Procedure | Preferred Approach |
|---|---|
| Total elbow arthroplasty | Bryan-Morrey or Wadsworth extensile posterior |
| Distal humerus fracture ORIF | Posterolateral (Campbell) or Paratricipital |
| Radial head fracture | Kocher lateral J or simple lateral |
| Medial epicondyle fracture | Medial (Molesworth-Campbell) with osteotomy |
| Lateral ligament reconstruction | Kocher / lateral |
| Complex instability / terrible triad | Global (Patterson-Bain-Mehta) |
| Olecranon fracture | Direct posterior |
Campbell's Operative Orthopaedics, 15th Ed. 2026 - Chapter 1: Surgical Approaches, Table 1.1 and Techniques 1.107-1.115
Different Surgical approaches to ankle explain it with appropriate images and diagrams
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Surgical Approaches to the Ankle
Source: Campbell's Operative Orthopaedics, 15th Edition (2026)
Overview
The ankle joint can be approached from six main directions, each offering different exposure of the tibiotalar joint, malleoli, and surrounding structures. The choice depends on the pathology, fracture pattern, required exposure, and structures at risk.
Summary Table
| Approach | Author/Technique | Primary Exposure | Main Use |
|---|---|---|---|
| Anterolateral | Technique 1.15 | Ankle, talus, tarsus | "Universal" - pilon, arthrodesis, talectomy |
| Anteromedial (Extensile) | Assal-Ray-Stern | Medial ankle, tibial plafond | High-energy pilon fractures |
| Lateral to Distal Fibula | Technique 1.17 | Lateral malleolus, syndesmosis | Fibula ORIF, ankle fractures |
| Kocher Lateral | Technique 1.20 | Subtalar, ankle, midtarsal | Talectomy, triple arthrodesis |
| Ollier | Technique 1.21 | Talonavicular, subtalar, calcaneocuboid | Triple arthrodesis |
| Transfibular Posterolateral | Gatellier-Chastang (1.22) | Posterior tibia, lateral talar dome | Posterior malleolus, OCD lateral talus |
| Posterior | Technique 1.24 | Posterior ankle, subtalar | Ankle arthrodesis, posterior fusions |
| Medial to Medial Malleolus | Technique 1.25 | Medial malleolus, anterior talus | Medial malleolus fractures |
| Transverse Medial (Osteotomy) | Koenig-Schaefer (1.27) | Entire ankle joint | OCD talus, fracture-dislocations |
| Medial to Posterior Tibia | Colonna-Ralston (1.28) | Posteromedial tibia, posterior malleolus | Posterior malleolus fractures |
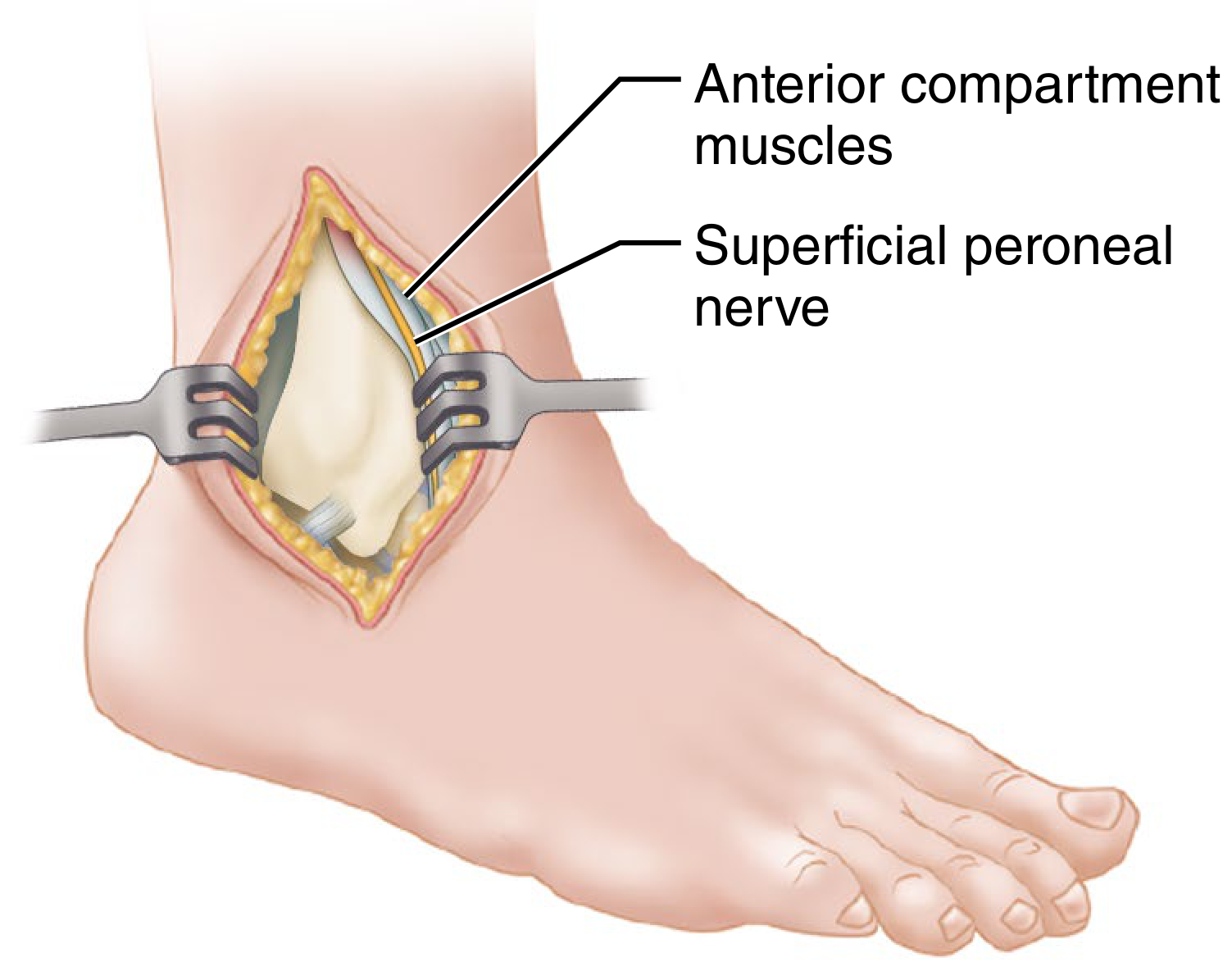
1. Anterolateral Approach - The "Universal Incision"
Indications: Ankle arthrotomy, talus excision, pilon fractures, single-incision triple arthrodesis, pantalar arthrodesis, talonavicular/subtalar/calcaneocuboid joint surgery.
This approach gives access to the ankle joint, talus, most other tarsal bones, and the anterior tuberosity of the calcaneus - while avoiding all critical vessels and nerves.
Key steps:
- Incision begins over the anterolateral leg, medial to the fibula, 5 cm proximal to the ankle joint
- Carried distally over the joint, anterolateral talus, calcaneocuboid joint, ending at the base of the 4th metatarsal
- Incise fascia and superior/inferior extensor retinacula down to the periosteum and joint capsule
- Find and protect the intermediate dorsal cutaneous branches of the superficial peroneal nerve
- Divide the extensor digitorum brevis in the direction of its fibers
- Retract the extensor tendons, dorsalis pedis artery, and deep peroneal nerve medially; incise the capsule
2. Anteromedial Extensile Approach (Assal, Ray, Stern)
Indications: High-energy pilon fractures requiring wide tibial plafond exposure.
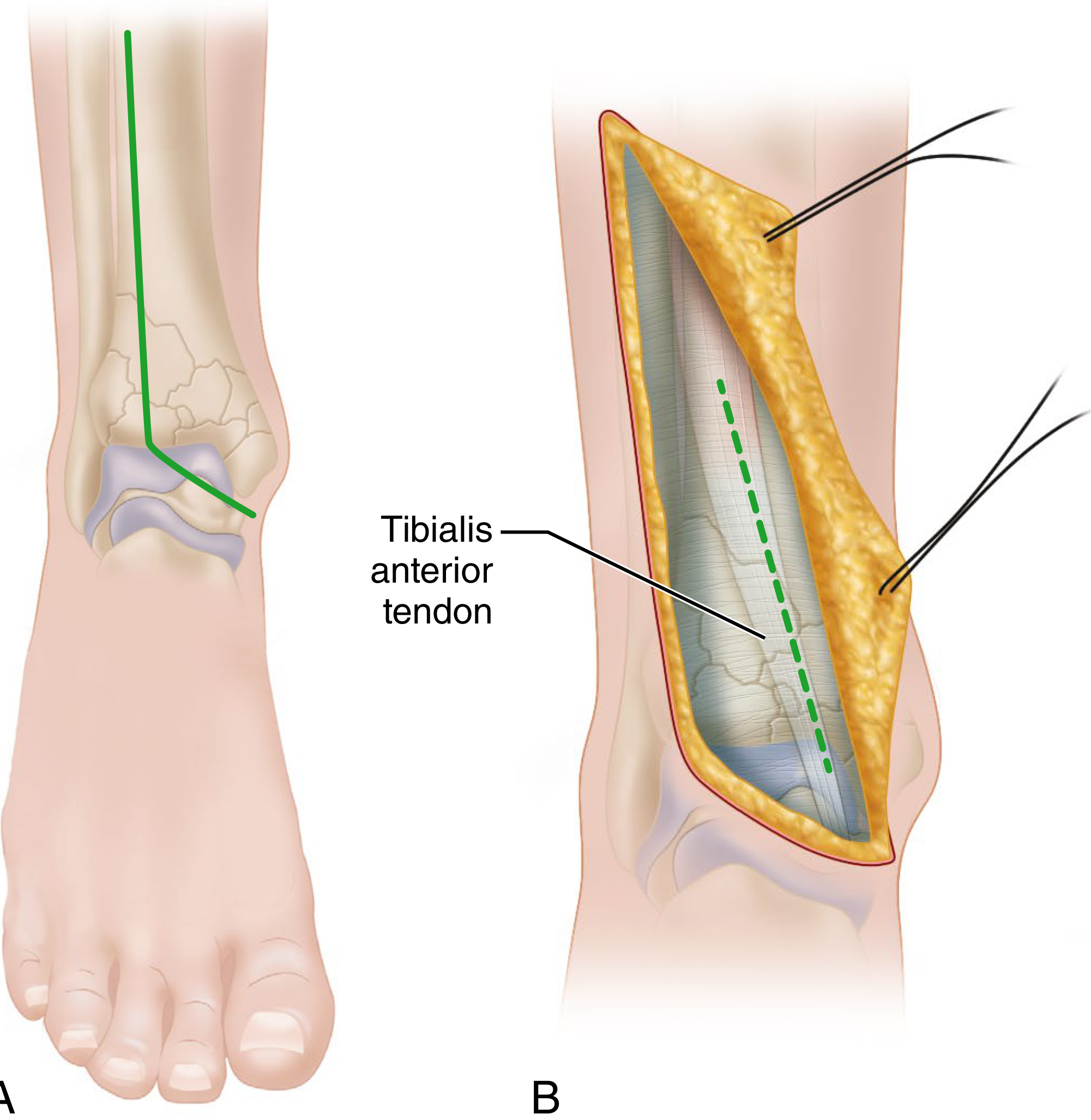
Key steps:
- Skin incision runs just lateral to the tibialis anterior tendon, then curves toward the tip of the medial malleolus
- Incise extensor retinaculum medial to the tibialis anterior tendon
- Develop the interval medial to the tibialis anterior to expose the anterior tibia and tibial plafond
- Protect the saphenous nerve and greater saphenous vein medially
3. Lateral Approach to the Distal Fibula
Indications: The most commonly used ankle approach - lateral malleolus ORIF, ankle fracture fixation, syndesmosis repair.
Key steps:
- Mark skin incision along anterior or posterior border of the distal fibula (surgeon preference)
- Elevate full-thickness flaps; avoid the superficial peroneal nerve (located ~10 cm proximal to distal fibular tip, range 3-18 cm)
- Incise fascia; elevate peroneal musculature posteriorly in a supraperiosteal fashion
- For posterior/posterolateral plating: partially incise the superior peroneal retinaculum (avoid complete disruption to prevent peroneal subluxation)
- For syndesmosis visualization: dissect anteriorly over fibula, partially incise extensor retinaculum; protect intact AITFL fibers
Key Precautions: The superficial peroneal nerve location is highly variable. Avoid complete disruption of the superior peroneal retinaculum. Do not inadvertently suture the superficial peroneal nerve during wound closure.
4. Kocher Lateral Approach to the Tarsus and Ankle
Indications: Midtarsal, subtalar, and ankle joint exposure; talectomy; access to the lateral talar articular surface.
Key steps:
- Incision begins just lateral and distal to the head of the talus
- Curves 2.5 cm inferior to the tip of the lateral malleolus, then posteriorly and proximally
- Ends 2.5 cm posterior to the fibula, 5 cm proximal to the lateral malleolus tip
- Incise fascia; retract peroneal tendons posteriorly - protect the lesser saphenous vein and sural nerve (posterior to incision)
- For larger field: divide peroneal tendons by Z-plasty
- Deepen distally; divide the calcaneofibular ligament to expose the subtalar joint
- Divide talofibular ligaments and dislocate the ankle medially for full articular access
Disadvantage: Risk of skin sloughing at incision margins, especially if ankle dislocation is performed (e.g., talectomy). In most cases the anterolateral approach is preferred.
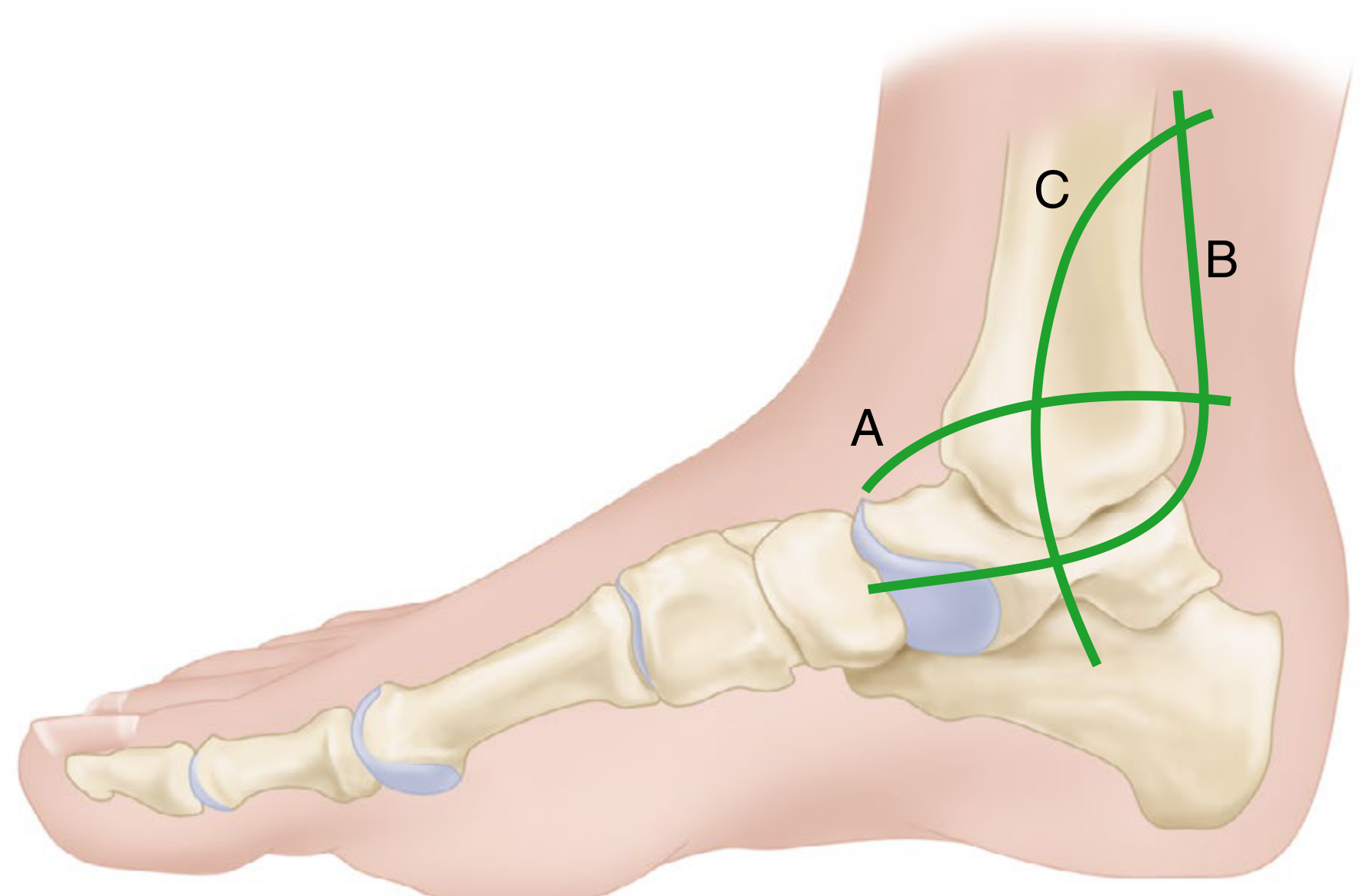
5. Ollier Approach to the Tarsus
Indications: Triple arthrodesis (talonavicular, subtalar, calcaneocuboid joints) - excellent exposure with minimal retraction.
Key steps:
- Skin incision begins over the dorsolateral aspect of the talonavicular joint
- Extends obliquely inferoposteriorly, ending ~2.5 cm inferior to the lateral malleolus (see line C in figure below)
- Divide the inferior extensor retinaculum in line with the incision
- Superiorly: expose long extensor tendons and retract medially
- Inferiorly: expose peroneal tendons and retract inferiorly
- Divide the origin of extensor digitorum brevis to expose all three joints
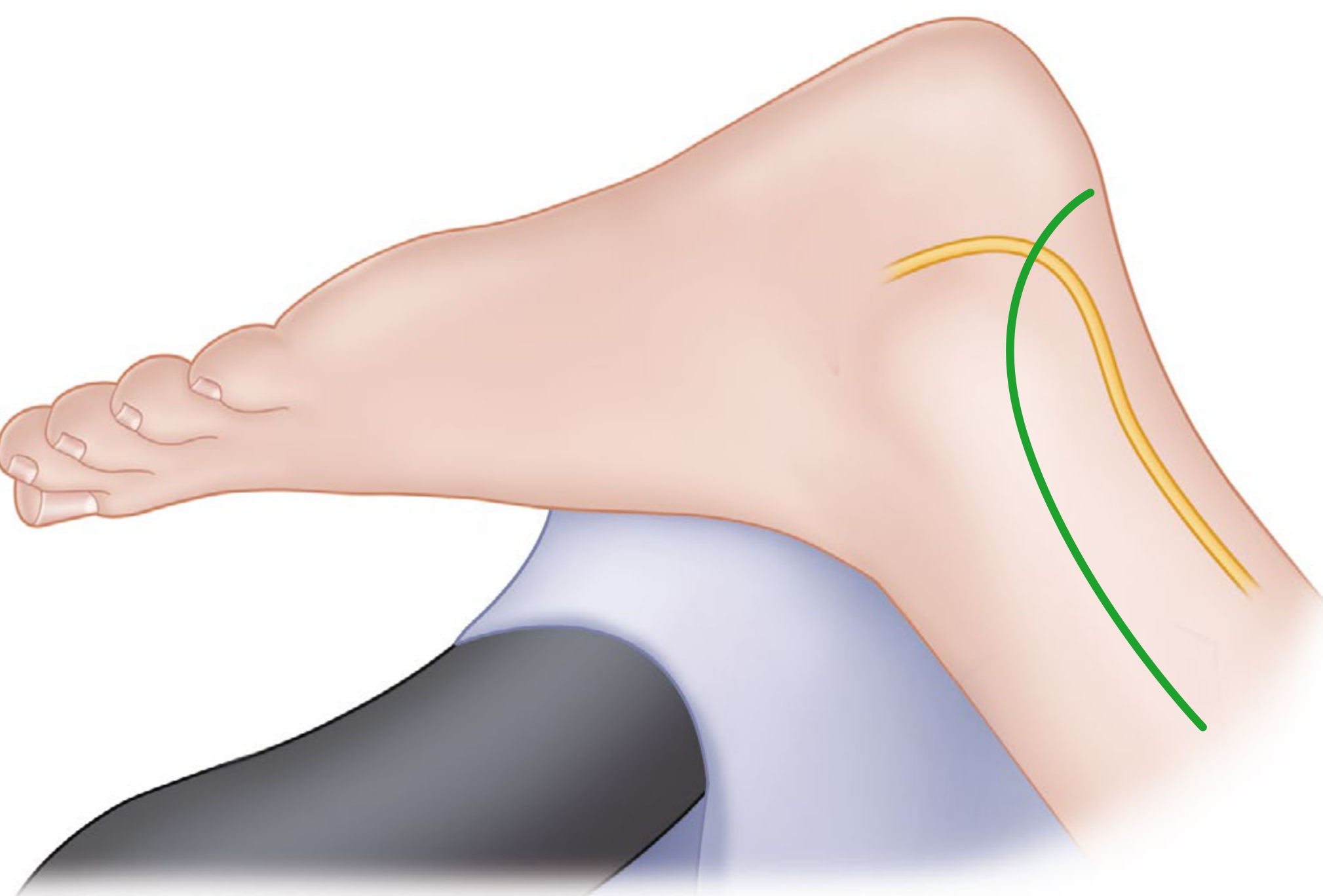
6. Transfibular Posterolateral Approach (Gatellier-Chastang)
Indications: Large laterally-situated posterior malleolus (posterior tibial lip) fractures; osteochondritis dissecans of the lateral talar dome; osteochondromatosis of the ankle; laterally-based total ankle replacement.
Key steps:
- Incision: 12 cm proximal to the lateral malleolus tip, along posterior margin of fibula, curving anteriorly 2.5-4 cm in line with peroneal tendons
- Expose fibula supraperiosteally; incise peroneal retinacula sheaths; displace peroneal tendons anteriorly
- If fibula is intact: osteotomize it 10 cm proximal to the lateral malleolus tip
- Divide the interosseous membrane and anterior/posterior tibiofibular ligaments
- Preserve the calcaneofibular and talofibular ligaments as a hinge
- Rotate the distal fibula laterally on this ligament hinge to expose the posterior tibia and lateral ankle
- Closure: Replace fibula; fix with transverse syndesmosis screw (overdrill fibula hole to allow compression). Dorsiflex ankle while tightening the screw (talar dome is wider anteriorly)
Key Precautions: In children with open physes - extra care to avoid fracture through the distal fibular physis. Always overdrill the fibula to get compression across the syndesmosis; failure causes mortise widening and arthrosis.
7. Posterior Approach to the Ankle
Indications: Direct posterior ankle arthrodesis (blade plate technique), posterior tibiotalar and subtalar fusion, posterior fracture fixation.
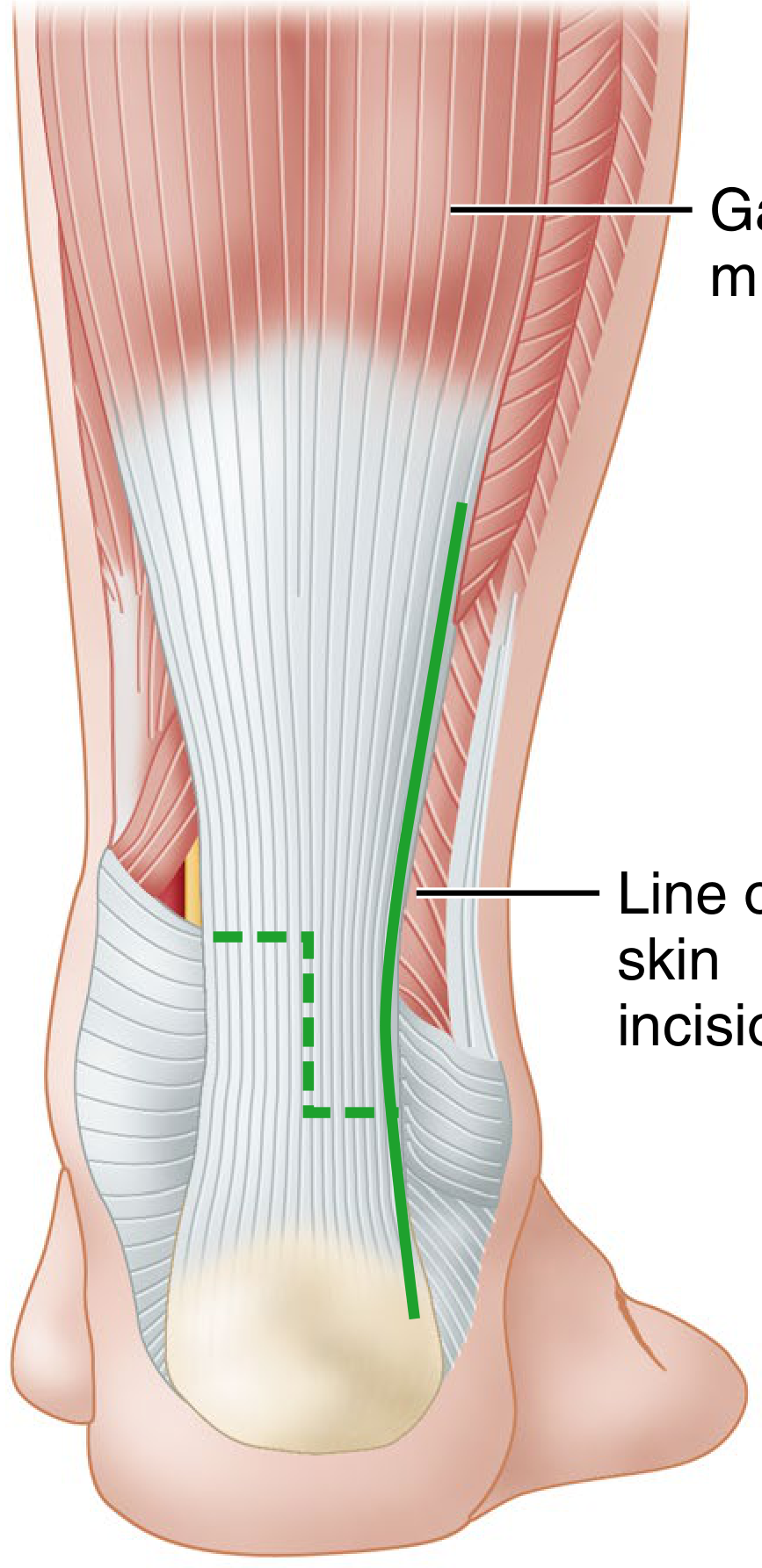
Key steps:
- Patient prone; 12-cm incision along the posterolateral border of the Achilles tendon down to its calcaneal insertion
- Divide superficial and deep fasciae; divide the Achilles tendon by Z-plasty or retract it
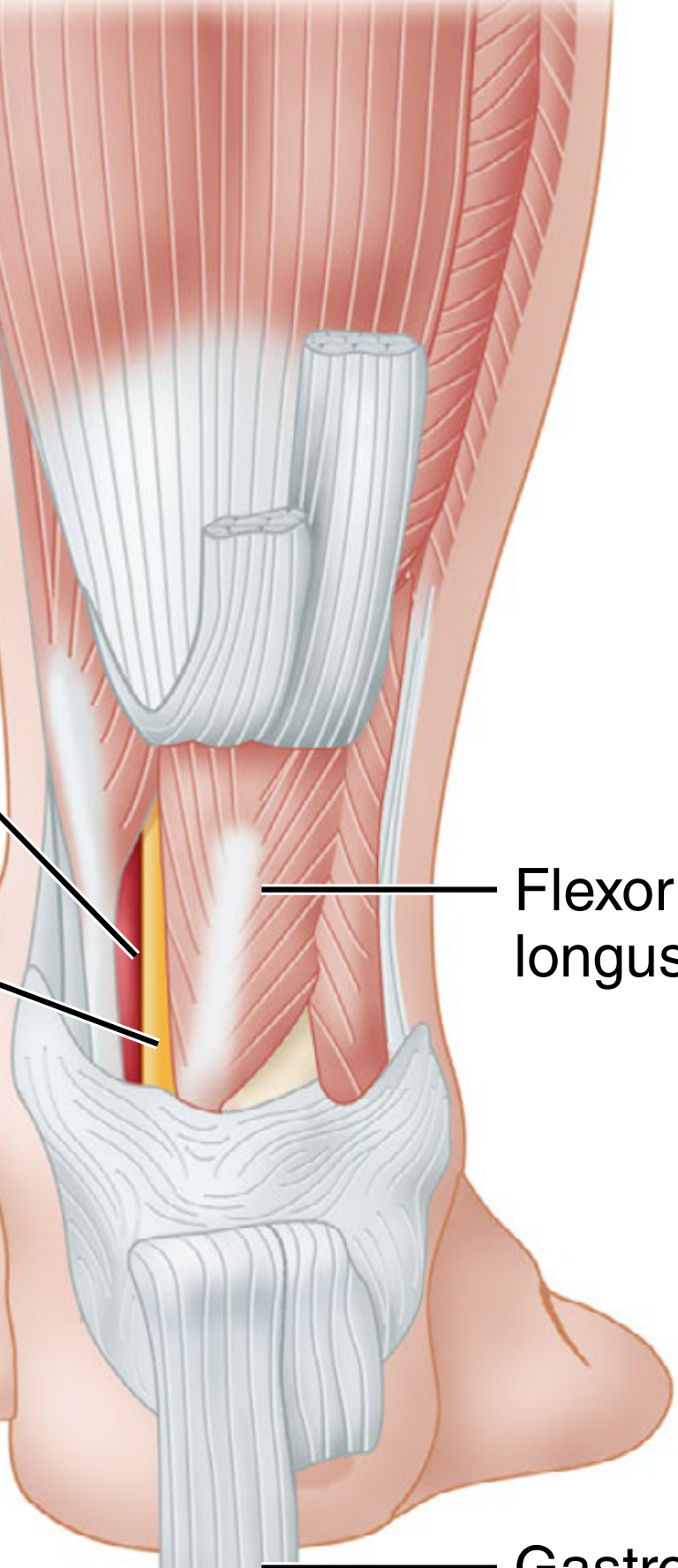
- Dissect through fat and areolar tissue to the posterior tibia, between the FHL and the peroneal tendons
- Retract the flexor hallucis longus (FHL) medially - this exposes 2.5 cm of the distal tibia, posterior ankle joint, posterior talus, subtalar joint, and superior calcaneus
- Keeping the dissection lateral to the FHL protects the posterior tibial vessels and tibial nerve (FHL acts as a barrier)
- Alternative: split the Achilles tendon longitudinally (lower wound complication rate, equivalent exposure)
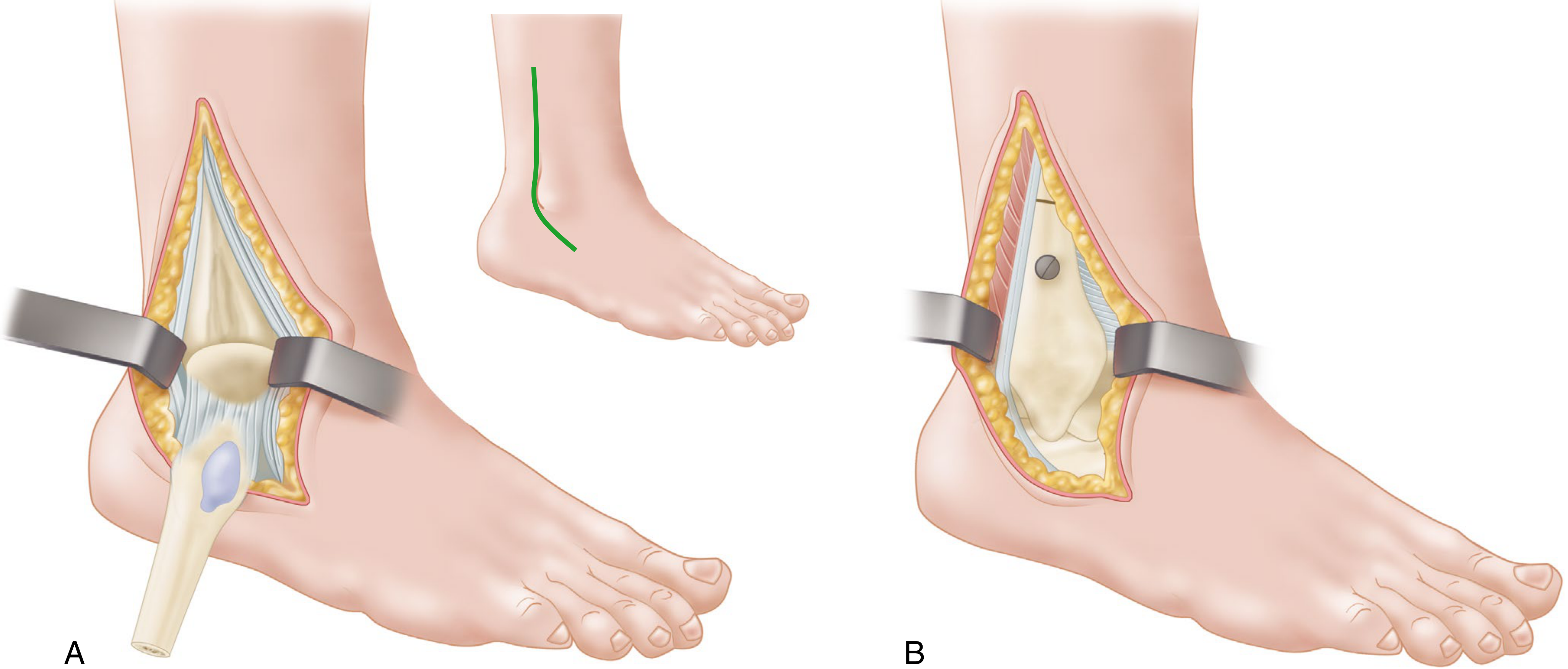
8. Medial Approach to the Medial Malleolus
Indications: Medial malleolus fractures; associated talar fractures requiring anteromedial exposure.
Key steps:
- Curved incision along the anterior aspect of the medial malleolus, ending at the tip of the anterior colliculus
- For associated talar fracture: apex posterior incision extending into an anteromedial talar approach
- Identify and protect the saphenous nerve and greater saphenous vein
- Incise through anteromedial joint capsule along the anterior border of the medial malleolus
- Gently retract medial malleolus; irrigate and inspect the ankle joint; reduce and fix with plate or screws
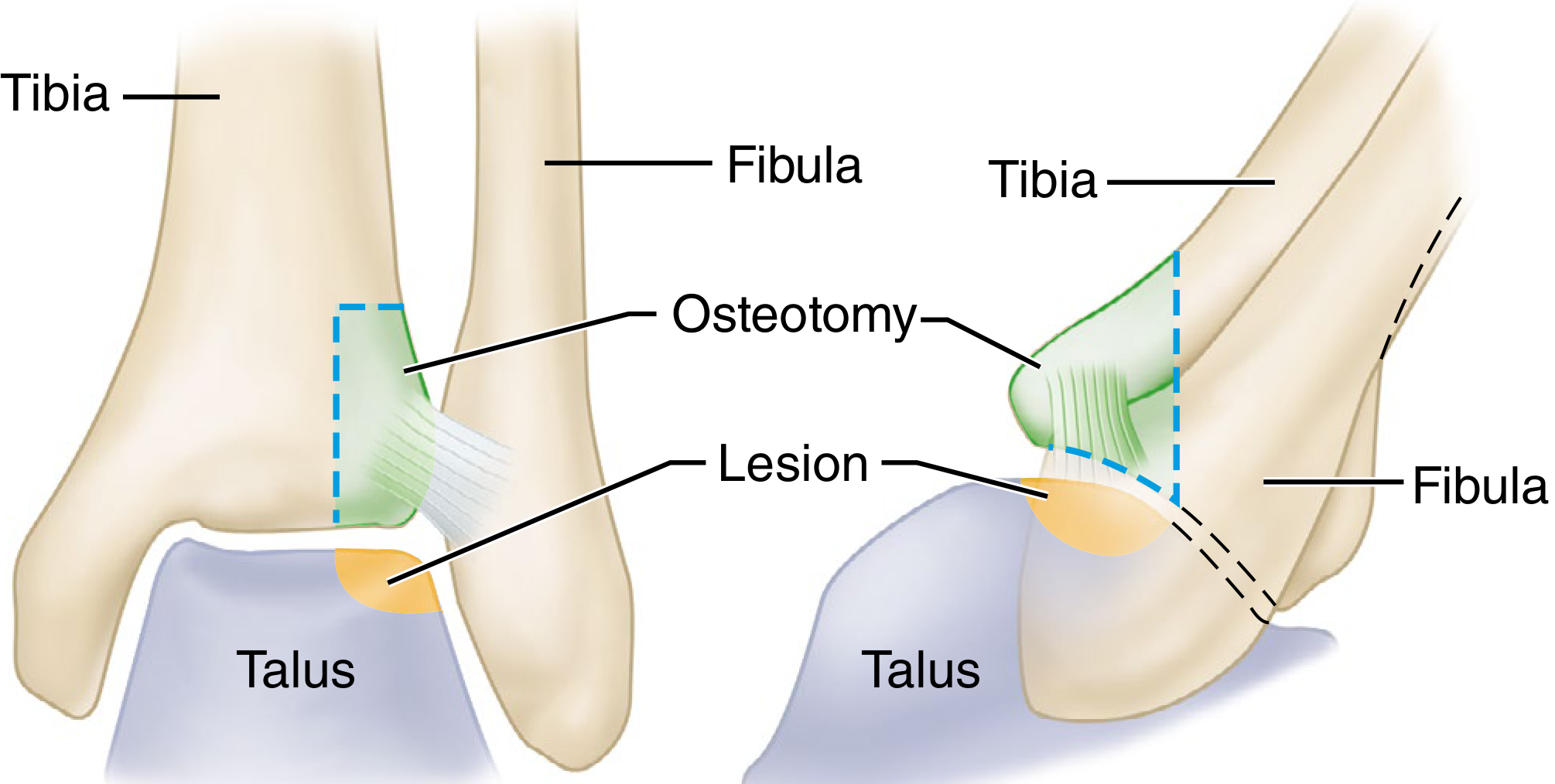
9. Transverse Medial Approach with Malleolar Osteotomy (Koenig-Schaefer)
Indications: Osteochondritis dissecans of the talus, fracture-dislocations of the talus, traumatic lesions of the ankle joint.
Key steps:
- Curved incision just proximal to the medial malleolus
- Osteotomize the malleolus with an osteotome or power saw; preserve the deltoid ligament attachment
- Subluxate the talus and malleolus laterally to expose all joint surfaces
- Pre-drill screw holes before the osteotomy (simplifies replacement)
- At closure: replace malleolus and fix with two screws using interfragmentary compression technique (prevents rotation)
Note: Not commonly used due to proximity of tibial vessels and nerve, and the transverse skin incision. The anterolateral approach is usually preferred.
10. Medial Approach to the Posterior Tibia (Colonna-Ralston)
Indications: Fractures of the medial part of the posterior malleolus requiring open reduction.
Incision line: Midway between the posterior tibial border and the medial border of the Achilles tendon, curving inferior to the medial malleolus to the medial foot border.
Key steps:
- Begin 10 cm proximal and 2.5 cm posterior to the medial malleolus; curve inferior to the malleolus
- Reflect capsule and periosteum
- Retract the posterior tibial tendon, flexor digitorum longus, flexor hallucis longus, and neurovascular bundle posteriorly and medially
- This exposes both the medial and posterior malleoli
Anterolateral Osteotomy for Lateral Talar Dome Lesions (Tochigi)
Indications: Centrolateral osteochondral lesions of the talar dome (OCD) not accessible by standard approaches.
Key Nerves and Vessels at Risk - Summary
| Approach | Structure at Risk | Location |
|---|---|---|
| Anterolateral | Intermediate dorsal cutaneous br. of superficial peroneal n. | In wound margins |
| Anterolateral | Deep peroneal nerve + dorsalis pedis artery | Retracted medially |
| Anteromedial | Saphenous nerve + great saphenous vein | Medial wound margin |
| Lateral to fibula | Superficial peroneal nerve | ~10 cm proximal to fibular tip (variable) |
| Kocher lateral | Sural nerve + lesser saphenous vein | Posterior to incision |
| Transfibular posterolateral | Distal fibular physis (in children) | At fibular osteotomy |
| Posterior | Posterior tibial vessels + tibial nerve | Protected by FHL (medial to FHL) |
| Medial malleolar | Saphenous nerve + vein | Anterior wound margin |
Quick Reference: Choosing the Right Approach
| Procedure | Preferred Approach |
|---|---|
| Pilon fracture (high energy) | Anteromedial extensile (Assal) ± posterolateral |
| Lateral malleolus ORIF | Lateral to distal fibula |
| Posterior malleolus (lateral) | Transfibular posterolateral (Gatellier-Chastang) |
| Posterior malleolus (medial) | Medial approach to posterior tibia (Colonna-Ralston) |
| Medial malleolus ORIF | Medial malleolus approach |
| Ankle arthrodesis (posterior) | Posterior approach (Technique 1.24) |
| Triple arthrodesis | Anterolateral or Ollier |
| OCD talar dome (lateral) | Tochigi anterolateral osteotomy |
| Talectomy | Kocher lateral (or anterolateral) |
| Subtalar fusion | Posterior or Kocher lateral |
| Total ankle replacement | Anterolateral or transfibular |
Campbell's Operative Orthopaedics, 15th Edition (2026) - Chapter 1: Surgical Approaches, Techniques 1.14-1.28
This is a shared conversation. Sign in to Orris to start your own chat.